
Abstract
Foodborne illnesses are a global public health issue. Responsibility to prevent foodborne disease is shared by many actors along the food supply chain, including consumers. However, consumers often lack knowledge about food safety and behaviors that can reduce risk. Consumers are often targeted for interventions to address these gaps, but a current comprehensive analysis of such interventions globally by type, geography, and outcome is lacking in the literature. In addition, there is a need to understand how individual interventions could be broadened to include the relationships between consumers and other actors in the food system, and how targeted communication strategies can affect behavior. We conducted a rigorous scoping review to assess consumer-facing food safety interventions carried out globally over the past 20 years, and categorized and analyzed them by type of intervention, methods, and outcomes to understand which interventions might be effective in changing consumer behavior, knowledge, attitudes, beliefs, and perceptions on food safety. Ninety-two interventions were reviewed, the majority of which were published in the last 10 years in North America. Most target adults, and 25% are directed at women and mothers. Health or risk communication interventions are becoming increasingly common to move beyond skill-based education and address risk perceptions of food safety that might motivate consumers. Only two studies addressed risk perception in consumers to potentially change food handlers' behavior outside of the home. This review suggests that focusing on risk perception combined with strategies that leverage emotion and trusted sources, such as respected peers or family members, might be useful strategies for interventions.
Introduction
Food safety generally refers to the assurance that food will not cause harm to the consumer when it is prepared and/or eaten according to its intended use (World Health Organization: Food and Agriculture Organization of the United Nations, 2020). In operational terms, it also refers to the actions performed to control adverse human health effects associated with consuming foods containing chemical or biological hazards (Nayak et al., 2019).
The World Health Organization (WHO) estimates that every year almost one in every 10 people will fall ill due to a foodborne illness, causing 420,000 deaths (World Health Organization, 2021a). One-third of these occur among children younger than 5 years (World Health Organization, 2021a) and are attributed to diarrheal diseases, most often caused by food contaminated with pathogens such as norovirus, pathogenic Escherichia coli, and Salmonella (World Health Organization, 2021b).
An estimated 33 million years of healthy life (DALYs, i.e., disability adjusted life years) are lost every year due to foodborne disease, much of which affects low- and middle-income countries (LMICs; defined by the World Bank as having a Gross National Income per capita of $1025 or less for low income and between $1026 to $12,375 for middle income) (World Bank, 2021). Importantly, regulation of food production, handling, and processing is usually less restrictive in these countries, and consumers have less access to equipment needed to safely handle food at home, such as clean water and adequate food storage (World Health Organization, 2021a), leading to poorer health outcomes (Wagstaff, 2002).
Consumers play important roles in food safety, both by how they handle food after acquiring it and by how they influence the supply chain. In all these roles, consumers' impact is affected by their knowledge, attitudes and drivers, and resulting behaviors and actions. Most consumers have some knowledge of the quality and safety of the foods they eat (Groth, 1999). Yet many have a poor understanding of how to properly prepare and cook foods to reduce risk of foodborne illness once they are home, including proper handwashing, preparing food to reduce cross-contamination, and cooking and storing foods at the correct temperature (Kunadu et al., 2016; Lando et al., 2016).
This risk can then be exacerbated by the sources of food consumers have to choose from, which in LMICs are often primarily informal outdoor “wet” markets and street vendors, where the handling of food at point of sale often fails to comply with food quality and safety standards (Grace, 2015). Thus, reducing risk across the food value chain, from production to distribution and preparation and consumption at home, is needed to reduce the risk of negative effects of poor food safety (Allard, 2002). Importantly, consumers can be potential “agents of change” by elevating their desire for a positive “food safety culture” that then influences food handlers and food suppliers. However, there is little evidence of effective, sustainable, and scalable consumer-facing interventions that can lead to improved food safety both inside and outside of the home.
Interventions aimed at consumers have mostly focused on changing attitudes and behaviors related to food safety at home (Sivaramalingam et al., 2015). More recent attempts at changing risk perception, defined as the subjective judgment a person makes about how risky something is to him or her such as the chance of contracting a foodborne illness, through risk communication principles have added new potential avenues to not only change individual behavior and attitudes but also affect social/cultural factors to create a food safety culture driven by consumer demands (Powell et al., 2011).
The purpose of this scoping review is to examine the literature from the past 20 years on interventions aimed at changing consumer perceptions, attitudes, and behaviors on food safety. Our analysis includes a categorization by intervention type, theory, method, and geography to elucidate strategies for intervention design. We discuss how these findings might be used to identify research gaps and advance the conceptualization of food safety, and we also consider the importance of communication strategies to address risk perception and affect food safety behavior.
Methods
The methodology for this review was conducted in accordance with the methodologies of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the scoping review framework outlined by Arksey and O'Malley (Arksey et al., 2005; Moher, 2009). This framework outlines five key phases for a scoping review: (1) identifying the research questions, (2) identifying relevant studies, (3) selecting studies for review, (4) charting the data, and (5) collating, summarizing, and reporting the results. The review was guided by the following questions: What are the characteristics of food safety interventions, including target audience, geography, theory, methods, and channels/modalities? How are the interventions evaluated, including research design and outcome measurements? Which interventions are associated with positive outcomes?
Data sources and search strategy
The initial search was done on June 16, 2020, in seven electronic databases: PubMed (National Library of Medicine), Embase (Elsevier), Web of Science (Clarivate Analytics), Cochrane Central (Wiley), CINAHL (EBSCOhost), GreenFILE (EBSCOhost) and
The search was limited to English and to publications since 2000. All citations were first uploaded to Endnote X.7 and duplicates removed. Remaining citations were then imported into the web-based systematic review software DistillerSR (Evidence Partners Incorporated, Ottawa, ON) for subsequent title and abstract review. The full search details are provided in Supplementary File S1.
Eligibility criteria
Studies were eligible for inclusion if they had a consumer focus (vs. only food handlers such as workers or vendors), addressed food safety (vs. interventions to treat or target diseases directly, such as vaccinations, drugs, or other therapies or studies or clinical studies of disease pathogens), and were an intervention attempting to change knowledge, attitudes, beliefs, or behaviors/practices related to food safety. They also had to be from peer-reviewed, nonpredatory journals (Committee on Publication Ethics, 2021; Stop Predatory Journals, 2021).
Articles that described the development of an intervention or development and psychometric testing of a measurement tool, or were review articles, were not included as they did not have outcomes related to answering the research questions. References, however, were reviewed to identify additional studies that may not have been captured in the search. Any relevant study found via reference screening had to also comply with the search (published since 2000 and available in English) and eligibility criteria (i.e., intervention study with a consumer- and food-safety focus).
Title and abstract relevance screening—levels 1 and 2
For the level 1 screening, citations were screened for inclusion by title and abstract by two independent reviewers for the first 1500 entries. Once a kappa of at least 0.80 was achieved (Dohoo et al., 2012), we used a “one reviewer to include, two reviewers to exclude” review. As recommended by Levac et al. (2010), reviewers met regularly to resolve conflicts and discuss the selection process. For level 2 screening, included citations were carefully reviewed for applicability, eligibility criteria, and duplicates.
Data characterization and synthesis
Once a final list of citations was created, all full-text articles were retrieved. If a full-text article was not available through institutional holdings or through interlibrary loans, attempts were made to reach out to authors or the journal. A data extraction form was used to categorize each study by the following information: author/title/journal/year of publication, intervention description, theory(ies) used, summary of study, outcomes, location, and sample description. Theory was defined as any set of constructs that authors used to frame the intervention or design intervention content. Any study found to not fit the eligibility criteria at this level was flagged and reviewed. The final summary table was then used in analysis (see Supplementary File S2). Descriptive statistics were calculated to summarize the data, including frequencies and percentages to depict nominal data, and then analyzed by outcomes.
Results
The initial search resulted in 21,397 studies (149 from gray literature sources); 3221 duplicate studies were found and omitted. After relevance screening, 322 met the eligibility criteria. Level 2 screening eliminated 149 duplicates not identified previously or because the article was not peer-reviewed or was out of the date range. An additional 50 were hand-added from reference screening and gray literature searches for a final sample of 223 citations. This included 92 interventions, 85 cross-sectional surveys, 21 qualitative studies, and 25 mixed-methods studies; this review is based on the intervention studies only. A summary of the screening process is presented in the PRISMA diagram in Figure 1.
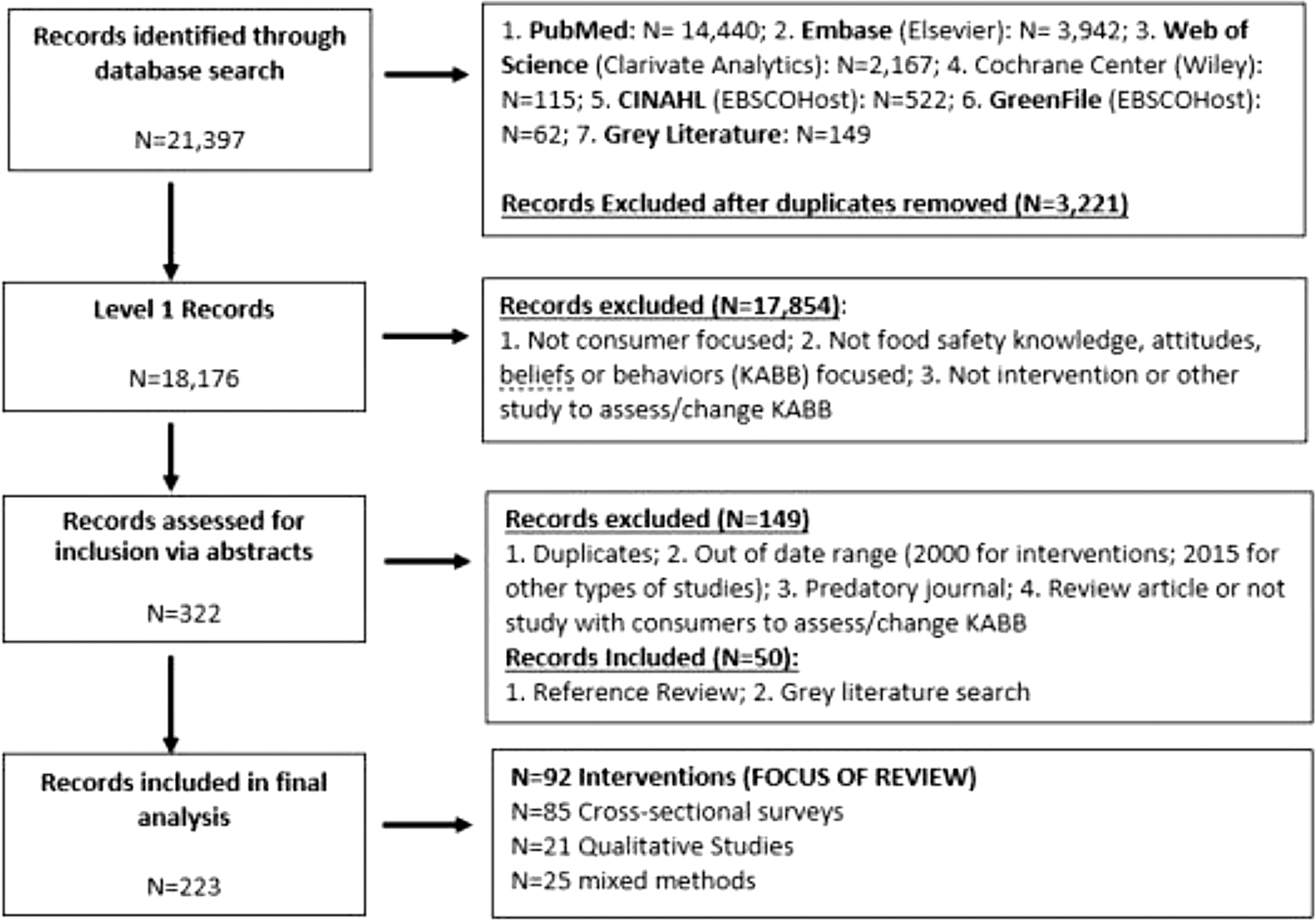
PRISMA diagram of scoping review of consumer food safety interventions. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
General characteristics of intervention studies
Of the 92 intervention studies, two-thirds had been published since 2010; 40% (n = 37) occurred in North America and 23.9% (n = 22) in Asia. Using the abovementioned World Bank characterization, 57.6% (n = 57) of the studies were conducted in high-income countries, and 8% (n = 8) in low-income countries (Table 1).
General Characteristics of Consumer Food Safety Interventions
High income = GNI per capita of $12,696 or higher; upper middle income = GNI per capita of $4096 to $12,695; lower middle income = GNI per capita of $1046 to $4095; lower income = GNI per capita of $1045 or less (World Bank, 2021).
GNI, Gross National Income.
Evaluation study design, theory, and target groups
Thirty-nine percent (n = 36) of studies used a one-group, pre/post-test evaluation study design with no control group, and 23.9% (n = 22) were quasiexperimental studies where the control group was selected from a similar community. Only 20.7% (n = 19) were randomized-controlled trials (RCTs). These RCTs were carried out in all regions of the world, but proportionately more occurred in Australia and Europe. North America had the fewest RCTs or randomized experiments (8/37; 22%).
The majority of studies in North America were one-group, pre/post or post-test only (21/37; 56.8%). In Asia, most studies were either quasiexperimental (8/22, 36%), using geographic location as controls, or one-group, pre/post or post-test-only designs (9/22, 40.9%). In Africa, 6 of the 14 were one-group, pre/post or post-test only (42.9%), five were RCTs or randomized experiments (35.7%), and three were quasiexperimental (21.4%) (Table 2). One-third of the studies indicated a theoretical underpinning for the intervention. The most commonly used theory was the Theory of Planned Behavior/Theory of Reasoned Action (TPB/TRA) (8.5%, n = 8/94) (Ajzen, 1991). In these studies, the constructs of perceived behavioral control, behavioral intention, and subjective norms were used to develop interventions that would increase perceived risk in the target audience (Mullan et al., 2010; Abbot et al., 2012; Milton et al., 2012; Gold et al., 2014; Lagerkvist et al., 2015; Barrett et al., 2020; Ghaffari et al., 2020).
Consumer Food Safety Interventions by Study Design, Theory, and Target Audience
Total accounts for studies with multiple country sites, intervention theories, or target groups.
Other behavior theories were used (e.g., Health Belief Model, Social Cognitive Model) as well as theories from the fields of communication and decision-making, including the Theory of Cognitive Biases (Furnham et al., 2011) and the anchoring effect (Shan et al., 2019), Prospect Theory (Tversky et al., 1992; Verbeke et al., 2008), and Mediatization Theory (Lundby, 2009; Yeasmin et al., 2014).
A variety of audiences were targeted. Adults, regardless of gender, were the most targeted group (39/98, 39.8%). Six studies targeted vulnerable adult groups, including those with low income or low literacy, minority groups (e.g., Latinos in the United States), or refugees/recent immigrants (Dharod et al., 2004; Ghebrehewet et al., 2004; Ratnapradipa et al., 2011; Gold et al., 2014; Mosby et al., 2015; Adedokun et al., 2018). Many specifically targeted women (21/98, 22%), and there was a strong focus on mothers (15/21, 71%). Finally, another target audience for food safety interventions were students, from primary school through university (34/98; 34.6%).
Characterizing intervention strategy: channels and intervention modalities
Studies represented a wide range of delivery channels/locations and intervention modalities. Seven delivery channels were identified: schools (primary/secondary; n = 20; 21.7%), schools (college/university; n = 12; 13%), communities (n = 25; 27.2%), clinics (n = 4; 4.3%), homes (n = 13; 14.1%), “population-based” (n = 16; 17.5%), and mixed (n = 2; 2.2%) (Fig. 2).
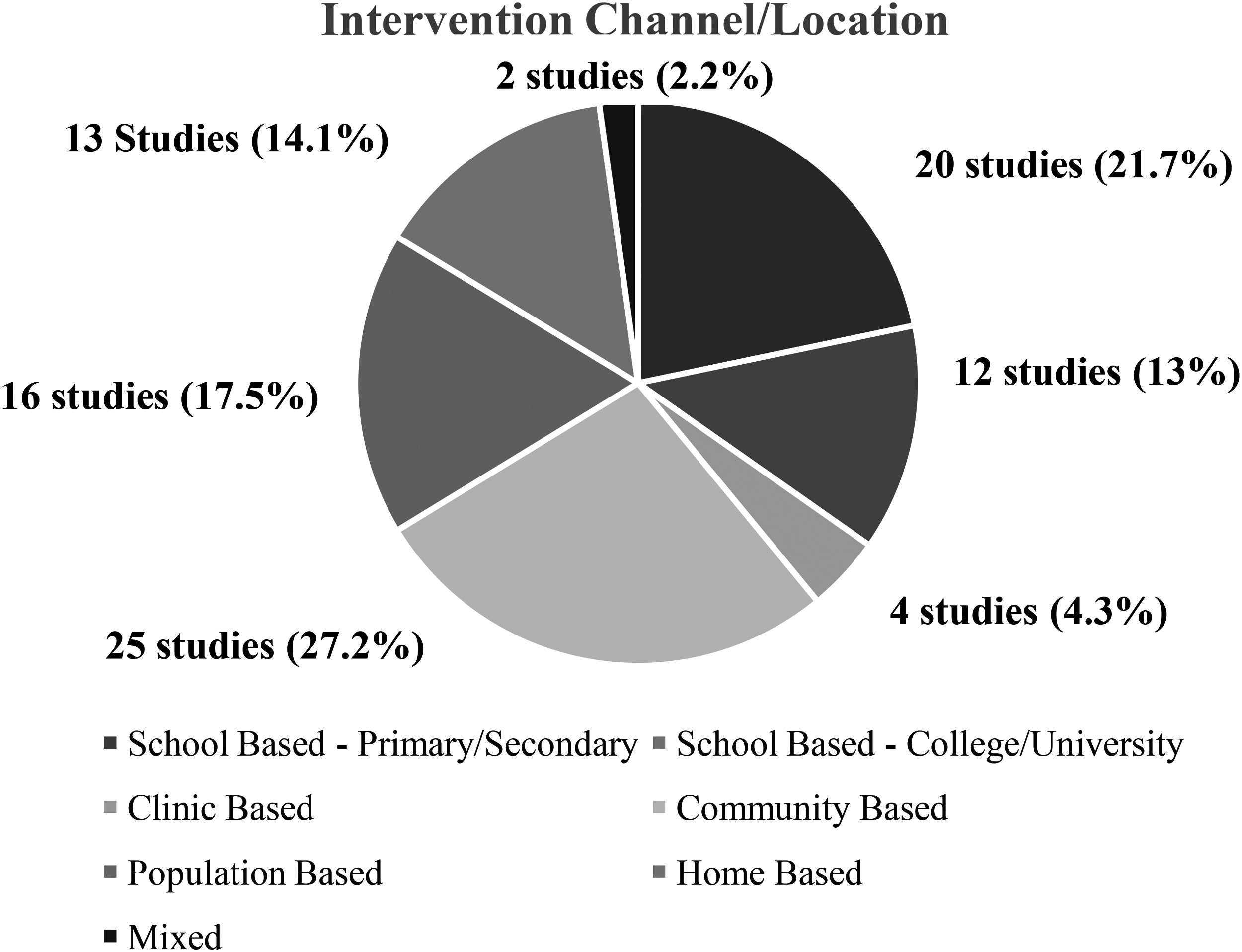
Proportion of consumer food safety interventions by channel/location.
Table 3 highlights the types of intervention modalities. Many were specific to the channel delivery (i.e., in-class curricula most often occur in school settings), but some modalities can be seen across channels. For example, health communication interventions—which included a wide range of communication tactics, including the use of mass media (television, radio) or social media (Facebook), often bundled into a campaign—were found in both community-based and population-based interventions. Overall, communication was integral to almost all the interventions reviewed, no matter the setting or intervention type. Communication methods varied, from social marketing, mass media, risk messaging, community or school health education, to interpersonal communication/counseling to deliver consumer food safety information.
Consumer Food Safety Interventions by Channel and Modality
WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
Characterizing evaluation design: outcomes, study designs, and study effectiveness
Because over half of the reviewed studies used either a one group, pre/post-test or post-test-only study design, most evaluation metrics involve measuring knowledge, self-reported behavior, or intentions (Table 4).
Outcome Variable Categories Used to Evaluate Consumer Food Safety Interventions
Most studies had more than one outcome variable and so percentages will not add up to 100%.
Four studies only assessed process-related outcomes and are not included in the total number.
Theory of Planned Behavior construct definitions: Perceived behavioral control: a person's perception of the ease or difficulty of performing the behavior of interest; Volitional control: cognitive process when person commits to particular choice; Anticipated regret: regret a person may feel in the future after a decision is made.
Other outcomes include incorporating direct observations of behavior or biomedical testing (i.e., presence of pathogens) to assess intervention effectiveness, increasing the rigor of the evaluation. By far the most common outcome is knowledge of food safety (52/88, 59.1%). Examples of knowledge variables measured include proper meat temperature, hygiene (e.g., handwashing), or specific knowledge of a disease caused by improper food handling. Similarly, 35 studies (39.8%) asked participants to self-report their behavior, usually from a pre- to post-test to assess potential change. Only 14 studies (15.9%) conducted actual observations of behavior. Risk perception was assessed in only 10 of the studies (11.4%).
Table 5 describes the outcome by study design. In RCTs, self-reported behavior was the most common type of outcome measured (11/19; 57.9%). In contrast, change in knowledge of food safety was the most common outcome assessed in nonexperimental studies (27/40; 67.5%). Randomized experiments, most often testing different types of messages on food safety, predominately assessed perceived risk of foodborne illness (5/7; 71.4%).
Proportion of Outcomes in Consumer Food Safety Interventions by Study Design
Four studies were process outcomes only and not included in the table.
RCT, randomized-controlled trial; TPB, Theory of Planned Behavior.
Finally, effectiveness of studies was assessed by examining whether statistically significant findings were achieved in the main study outcomes. In studies with multiple outcomes, effectiveness was assessed based on whether the majority of those outcomes had reached statistically significant results. If a study was effective on a minority of outcomes, it was rated as “marginally” effective. Overall, all types of studies except for one-group, post-test-only studies showed effectiveness. One-group pre/post-test designs have an overall effectiveness of 79.4% (27 of the 34 studies) compared with 86.4% of quasi experimental studies (19 of 22 studies) and 84.2% of RCTs (16 of 19 studies). All seven of the randomized experiments showed significant results.
Discussion
This review showed that the majority of the evaluated food safety interventions were conducted in the last 10 years and used a quasiexperimental study design. Although most studies assessed self-reported knowledge and behavior, the intervention type and target groups varied. While logistically it is easier to use a one-group, pre/post-test study design and to gather self-reported behaviors, results can be skewed due to the Hawthorne effect (overestimation of effects because participants answer how they know they should answer or because they are being observed) (McCambridge et al., 2004) or environmental or other biases, such as societal expectations or accepted gender roles (Bhattacharyya et al., 2011) that may affect results.
About a quarter of the studies were randomized interventions, through either RCTs in community, clinic, or school settings, or randomized experiments presenting different types of risk information to understand what messages are most effective. These studies may have more generalizable results due to the rigor associated with the study design.
There are approaches that resulted in positive outcomes that merit further discussion. Studies examining the concept of risk perception as an important antecedent to purchasing food or food safety behavior showed significant effects related to changing behavior. Risk perception research has shown that consumers or “lay people” perceive hazards and risk differently than experts (Slovic et al., 2005), based on overall knowledge and how risk is prioritized in everyday life. Risk perception might be heightened if the persons feel they do not have control or if they do not trust those providing the risk information (Slovic et al., 2004). Often risk is conceptualized at an emotional level (affect) (Kahneman et al., 1982), and decisions are made using heuristics or “short cuts” that are influenced by psychological or cultural factors (Kahneman et al., 1982; Siegrist et al., 2006, 2014).
This was illustrated in studies in this review where consumer risk perceptions were changed by manipulating the messaging strategy and designed as brief controlled experiments in which consumers were randomly exposed to different message strategies and then were asked to disclose their perceived risk for foodborne illness or self-efficacy in being able to act on food-safety directives. For example, Nauta et al. (2008) tested web-based messages in the Netherlands that embedded cues to improve food safety. One group received basic information; a second received the same messages but with “aggressive” language, colors, and images that evoked an emotional response; a third group received messages meant to evoke disgust along with risk information that was embedded with a behavioral cue to perform self-protective food-related behaviors.
Finally, a fourth group was given control information on nutrition. In this study, risk information increased food safety behavior intention, and behavior and emotional reactions such as disgust were associated with intended and actual food safety behavior. Other types of risk perception studies were done through consumer experiments (Verbeke et al., 2008, 2014), in-market experiments at points of sale (Lagerkvist et al., 2015), or consumer education (Yarrow et al., 2009; Takeuchi et al., 2017).
Only three studies were found that tested risk perception and risk communication strategies in market settings (Lagerkvist et al., 2015; Takeuchi et al., 2017; Chalak et al., 2019). Chalak et al. (2019), for example, tested messages based on quantitative risk reduction attributes of purchasing street food (specifically “shawarma”) with families in Lebanon. They found that disclosing food safety attributes and food safety certification of street vendors were two independent factors that affected consumer preferences and willingness to pay for shawarma that was assessed to be safer.
Another study by Lagerkvist et al. (2015) was a field experiment that provided shoppers with information about actions that a vendor had taken to minimize food safety risks from kale (washing, gloves, proper storage, etc.). The experiment showed that, compared with customers who were not exposed to information on safety-enhancing attributes at point of sale (control group), customers who were exposed reported less perceived risk and higher volitional control, which led them to choose vendors who had taken measures. They also were willing to pay more for kale that was handled safely than customers in the control group. The results of these studies illustrate that risk evaluations may not be based on real risk or quantifiable estimates, but on how individuals perceive that risk and whether it has been deemed to be important.
In high-income countries, where there is generally a higher level of perceived trust in food systems and where people are generally positive about the food supply, communicating about the risks associated with consumption of unsafe food has not been shown to be important in consumer food decision-making (Green et al., 2003; Siegrist et al., 2006). However, little is known about how risk perceptions may differ in LMICs or when there is far less trust or understanding of how the food chain is managed. There are few national-level surveys on food safety issues in these countries, but some smaller studies have indicated significant concern over food safety (Grace, 2015; Lloyd's Register Foundation, 2019).
Importantly, we found only three studies focused on the interactions between the consumer and food handlers (Lagrekvist et al., 2015; Takeuchi et al., 2017; Chalak et al., 2019); Interventions are either focused on the food handler or the consumer only. This gap is significant given the importance of the whole food chain in ensuring the safety of food, especially in LMICs where food chains are often fragmented and involve multiple actors (Grace, 2015), making it difficult to monitor food handling practices. Building or leveraging trust in the consumer/vendor relationship, using consumers to persuade food vendors to pay greater attention to food safety, or both, may be useful to improve behavior on both sides. This is an important area for future study.
In addition to risk perception and decision theory, “nudge theory” (Thaler and Sunstein, 2009), a subfield of behavioral economics, is an approach that draws on positive reinforcement and subtle environmental changes to change behavior (Sunstein, 2014). Nudge theory has been used in the nutrition behavior field (Guthrie, 2017), but there were no studies that applied this approach in this review. However, some formative work in Vietnam indicates how nudge theory might be applied to food safety by expanding on how people see their individual behavior in relationship with other actors (Hennessey et al., 2020). Drawing on the MINDSPACE framework, the authors in that study reported several “nudges” that merit further examination, such as emotions, trust, reputation, as well as the type of visuals and message framing used in interventions. These nudges can be applied across all actors of the value chain, not just consumers.
Another important communication intervention strategy was the use of social marketing, an approach that adapts commercial marketing techniques used to sell products to change social behaviors, such as food safety (Partnership for Food Safety Education, 2021). Studies that used this approach were able to effectively change community risk perceptions of food safety. Biran et al. (2014), for example, deployed a social marketing campaign called SuperAmma (means SuperMom) in rural villages in India. In that study, the authors used “emotional drivers” by focusing on “disgust,” or the desire to avoid and remove contamination, along with the maternal emotional driver of “nurturing” to influence behaviors.
The campaign consisted of flipcharts and posters, a campaign truck, school and community events, and household visits. This social marketing campaign was shown to significantly affect handwashing behavior in the intervention villages, indicating that this approach may be an important way to affect community or peer influences in food safety behavior.
Mass media, another communication channel often used in social marketing campaigns, has also been used effectively to change food safety awareness and knowledge. Wogu et al. (2018) used mass media in Nigeria to increase awareness and personal hygiene behaviors through social media, radio, and television. It was not found to change behaviors or increase awareness of Lassa fever and its transmission, but the intervention did increase understanding of hygiene behaviors directly related to food safety.
In the United States, Dharod et al. (2004) created a food safety media campaign using materials from the Fight Bac! Campaign from the U.S. Department of Agriculture (Partnership for Food Safety Education, 2021) and disseminated it through several channels (radio, television, newspapers) aimed specifically at reaching Latino populations in Connecticut and southwest Massachusetts. This intervention showed that a third or more of the respondents remembered seeing campaign advertisements, and those who had were significantly more likely to have adequate food safety knowledge in a pre/post-test assessment. However, mass media is less effective at changing actual behavior (Wakefield et al., 2010) and therefore should not be the only intervention modality to address consumer food safety.
Another common intervention strategy, especially in LMICs, was in-person education. Often these interventions are meant to increase skills, especially of mothers in preparing food for infants and feeding them. Some of these studies included the use of “promoters” or other types of community health volunteers (Richards et al., 2008; Chidziwisano et al., 2020). Chidziwisano et al. (2020) relied on local residents in the Chikwawa District in Malawi and trained them on complementary food hygiene behaviors, such as handwashing with soap, washing kitchen tools, and reheating food. This study showed that a psychosocial approach was effective with significant improvements in handwashing and proper cleaning and storage of kitchen utensils.
Other studies have used this approach to not only include one-on-one instruction in the home but also provide supportive adjunct messaging through the community and schools (Sheth and Obrah, 2004; Metwally et al., 2006; Sheth et al., 2006; Shen et al., 2015; Andrade et al., 2019; Edward et al., 2019; Gizaw and Addisu, 2020).
In a multinational study by Edward et al. (2019), for example, communities in four countries (Cambodia, Guatemala, Kenya, and Zambia) were provided a package of interventions and implementation instructions they could choose to implement, including household-level training by community health workers, “social accountability” mechanisms using scorecards to enhance community knowledge about resources, and community management councils that provided targeted counseling about handwashing and infant feeding. This study found that handwashing behavior in intervention sites was significantly improved, and this was directly correlated with a lower incidence of diarrhea in children.
Another benefit of in-person interventions is the relationship that can develop between the messenger and recipient. Trust, specifically using trustworthy “messengers” of food safety information through the use of community health workers or peers, is associated with positive outcomes. Consumer trust influences how consumers receive and respond to information, including risk information (Nardi et al., 2020), and so, the community health worker strategy addresses this by providing health information by trusted sources to their peers.
A systematic review on the use of community health workers in maternal and child health interventions, for example, showed that they were particularly effective in promoting exclusive breastfeeding (Gilmore et al., 2013). While promoting breastfeeding per se is not a food safety intervention, improving this outcome can have a “trickle down” effect to overall food safety for families by training women in proper handwashing and other hygiene behaviors.
In our review, this strategy was used most often in LMICs and to target households, women, or mothers, all showing significant or marginally significant results on outcomes, including changing food safety knowledge and attitudes, self-reported and observed behaviors, and changes to the home environment (Sheth et al., 2004; Metwally et al., 2006; Forster-Cox et al., 2009; Safari et al., 2017; Takeuchi et al., 2017; Geresomo et al., 2018; Andrade et al., 2019; Edward et al., 2019; Ghaffari et al., 2020; Morse et al., 2020). Thus, messengers of food safety information should be considered when developing interventions to ensure effectiveness.
Finally, interventions that target children in school, after school, or through community-based events also appear to be an important strategy. Children can be powerful motivators of parental behavior, modelers of new behaviors, and a conduit of new information to families. Evidence suggests that young people can effectively share health knowledge in an upward direction (Wingert et al., 2014; Burrows, 2017). Kang et al. (2017), for example, showed that you could combine community health volunteers with community-based education for adults and children through the use of role plays, demonstrations, group discussions, and events as a way to focus on whole communities for changing food safety culture.
Others have showed the utility of developing and embedding curricula in the school day to increase awareness and knowledge of food safety concepts, using multimedia strategies that use more than one medium of communication, such as videos, videogames, or other “entertainment education” strategies to provide information that engages children and young adults. For example, Quick et al. (2013) developed and tested a videogame called “Ninja Kitchen” to enhance food safety information, which uses games, a “fun” spokes-character who models safe food handling behaviors, and 15 levels of gaming that has “hazards” that players have to navigate (i.e., leaving food out or cross-contamination).
The evaluation indicated that students who used the game were more likely to believe themselves to be at risk for foodborne illness, had stronger attitudes about the importance of food safety, and had greater intention to practice proper handwashing behaviors. This can then have effects at home when children bring back this information to their families. Thus, school and community-based channels, with focus on children and their families, may be useful in helping communities understand the role all members have in food safety.
Limitations
This scoping review has some limitations. First, only articles available in English were included, although interventions published in other languages may have enriched the review. In addition, some potentially relevant articles may have been missed by the search; this was mitigated as much as possible by a comprehensive search strategy, working with a medical librarian, and a search that encompassed seven databases, a gray literature search, and a hand citation search to spot-check results.
In addition, as the review focused on food safety, it did not include other fields that could be relevant to designing consumer-facing food safety interventions, such as water quality or other aspects of public health. In addition, positive publication bias, which relates to how studies with positive results are more favorably discussed than those with null results (Jannot et al., 2013; Duyx et al., 2017), can confound interpretation of results. Multiple analyses illustrate that studies with positive results are not only more likely to be published but are also more likely to be accepted by high-ranking journals (Olson et al., 2002; Fanelli, 2012), making the number that shows results conflated. This could affect interpretation of results of this review.
Finally, the review only encompasses interventions over the past 20 years. This could limit the results; although we found that the majority of the interventions reported on in the past two decades had occurred in the past 10 years.
Conclusions
We used a structured scoping review methodology to elucidate interventions tested on consumers to address food safety issues over the last 20 years. Interventions that seek to affect consumer food safety behavior have focused primarily on improving the individual's knowledge about food safety practices. This review suggests that focusing on risk perception combined with strategies that leverage emotion and trusted sources, such as respected peers or family members, is a useful strategy for interventions.
Footnotes
Acknowledgments
We would like to thank Stephanie Roth, MLIS, medical librarian at the Ginsberg Health Science Library at the Temple University Lewis Katz School of Medicine, for her help in developing and implementing the search strategy. We also thank Sarah Tomkins and Carlos Cruz, undergraduate interns in the Temple University Risk Communication Laboratory, for their administrative assistance.
Authorship Confirmation Statement
All authors contributed to the analysis or writing of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was made possible through support provided by Feed the Future through the United States Agency for International Development (USAID), under the terms of the EatSafe Cooperative Agreement No. 7200AA19CA00010. The opinions expressed herein are those of the author(s) and do not necessarily reflect the views of USAID, the U.S. Agency for International Development, or the U.S. Government.
Supplementary Material
Supplementary File S1
Supplementary File S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.