
Abstract
Vibrio parahaemolyticus is the leading cause of seafood-related foodborne illness globally. In 2018, the U.S. federal, state, and local public health and regulatory partners investigated a multistate outbreak of V. parahaemolyticus infections linked to crabmeat that resulted in 26 ill people and nine hospitalizations. State and U.S. Food and Drug Administration (FDA) laboratories recovered V. parahaemolyticus, Salmonella spp., and Listeria monocytogenes isolates from crabmeat samples collected from various points of distribution and conducted phylogenetic analyses of whole-genome sequencing data. Federal, state, and local partners conducted traceback investigations to determine the source of crabmeat. Multiple Venezuelan processors that supplied various brands of crabmeat were identified, but a sole firm was not confirmed as the source of the outbreak. Travel restrictions between the United States and Venezuela prevented FDA officials from conducting on-site inspections of cooked crabmeat processors. Based on investigation findings, partners developed public communications advising consumers not to eat crabmeat imported from Venezuela and placed potentially implicated firms on import alerts. While some challenges limited the scope of the investigation, epidemiologic, traceback, and laboratory evidence identified the contaminated food and country of origin, and contributed to public health and regulatory actions, preventing additional illnesses. This multistate outbreak illustrates the importance of adhering to appropriate food safety practices and regulations for imported seafood.
Introduction
Vibriosis is a gastrointestinal disease caused by infection from pathogenic species of the family Vibrionaceae including Vibrio parahaemolyticus, which infects an estimated 92,400 people per year in the United States, with most infections linked to the consumption of raw or undercooked molluscan shellfish (Collier et al., 2021; Ghenem et al., 2017; Iwamoto et al., 2010; Scallan et al., 2011). In 2017, 3% of all the reported foodborne outbreaks with an identified etiology in the United States were caused by V. parahaemolyticus and it is currently recognized as the leading cause of seafood-related foodborne illness globally (Ghenem et al., 2017; Su and Liu, 2007; U.S. Centers for Disease Control and Prevention, 2017).
Roughly 19% of food consumed in the United States is imported, including ∼97% of fish and shellfish (Gould et al., 2017). Venezuela accounted for roughly 60% of the total crabmeat imports in 2018 (U.S. Department of Agriculture Foreign Agricultural Service, 2021). Although crabmeat handling and cooking methods can vary depending on regional customs and regulations, most crabs are cooked in steam retorts or in boiling water with varying times and temperatures (Ward, 2000). Generally, cooked crabs are cooled, and the crabmeat is picked and packed by hand (Ward, 2000). In 1971, two of the first three well-documented outbreaks of V. parahaemolyticus infections in the United States linked to crab consumption were caused by postcook cross-contamination from live crabs, while a third was due to insanitary preparation (Dadisman et al., 1972).
In 2018, federal, state, and local partners investigated a multistate outbreak of V. parahaemolyticus infections linked to refrigerated, cooked, ready-to-eat (RTE) crabmeat labeled “fresh” or “precooked” and sourced from Venezuela (U.S. Centers for Disease Control and Prevention, 2018b; U.S. Food and Drug Administration, 2018a). This outbreak investigation illustrated the importance of public health partnerships in outbreak response and food handling practices for seafood production.
Materials and Methods
Epidemiologic investigation
In 2018, through PulseNet (Swaminathan et al., 2001), the Maryland Department of Health (MDH) identified five ill people with isolates of V. parahaemolyticus associated with the consumption of crabmeat imported from Venezuela that shared a pulsed-field gel electrophoresis (PFGE) pattern combination (Hassan et al., 2019; U.S. Centers for Disease Control and Prevention, 2016a). Local and state investigators interviewed ill persons using the Centers for Disease Control and Prevention's (CDC) Cholera and Other Vibrio Illness Surveillance (COVIS) system, which included a questionnaire regarding food history and seafood exposures and the source(s) and country of origin of the seafood products (U.S. Centers for Disease Control and Prevention, 2019). Additional ill people associated with consumption of crabmeat were identified through PulseNet; Maryland's posting to The Epidemic Information Exchange (Epi-X), a nationwide public health notification system; and coordinated follow-up between CDC and jurisdictional partners on all V. parahaemolyticus ill people reported to the CDC.
An outbreak-associated ill person was defined as a gastrointestinal illness consistent with vibriosis occurring in a person with illness onset between April and July 2018, and (1) a V. parahaemolyticus isolate that matched either the primary or secondary PFGE pattern combination; (2) matched the cluster by whole-genome sequencing (WGS); or (3) an illness occurring in a person with a V. parahaemolyticus clinical isolate that was not further analyzed but who reported consumption of RTE crabmeat ≤7 d before illness onset.
Traceback investigation
A traceback investigation was initiated as per standard U.S. Food and Drug Administration (FDA) traceback practices (Council to Improve Foodborne Outbreak Response, 2014; Irvin et al., 2021). Individuals' exposure to crabmeat, including dates, receipts, and purchase documents, was analyzed. Ill people selected for traceback included those who reported eating crabmeat with confirmed dates of purchase or consumption. Crabmeat purchase and production records were collected from retailers, distributors, and importers along the supply chain. Information relevant to time line construction collected from suppliers included stock rotation, delivery frequency, and product shelf-life.
Laboratory investigation
Commercially packaged crabmeat samples were collected by the FDA and state partners throughout the distribution chain. Each FDA sample consisted of five plastic containers, each with one pound (0.45 kg) of cooked crabmeat. FDA samples were tested for the presence of Salmonella and Listeria spp. in addition to V. parahaemolyticus using standard methods (Andrews et al., 2021; DePaola et al., 2004; Hitchins et al., 2004). The State of Maryland Rapid Response Team (SMarRRT) collected six imported crabmeat samples (1–2 pounds or 0.45–0.90 kg), all representing different lots, from Venezuela. The SMarRRT-collected sample size depended on the product available at the time of collection.
As a screen, before WGS or PFGE analyses of isolates from the product samples, automated DNA extraction, using the Roche® MagNA Pure 24 instrument, followed by quantitative polymerase chain reaction (Roche) to determine the presence of the V. parahaemolyticus toxin genes tdh and tlh, was performed on the whole lump crabmeat, collected by SMarRRT, by the MDH Laboratories Administration (Ward and Bej, 2006). PFGE and WGS analyses for ill people identified or shared with PulseNet were completed using standardized protocols (Parsons et al., 2007; U.S. Centers for Disease Control and Prevention, 2018a; U.S. Centers for Disease Control and Prevention, 2016b). All patterns were assessed for similarity to the originally identified Maryland clinical isolates' PFGE patterns.
The CDC assessed genetic relatedness of representative clinical isolates from stool samples through WGS by performing a high-quality single-nucleotide polymorphism (hqSNP) analysis. The hqSNP analysis had phages and plasmids masked, used an internal reference (National Center for Biotechnology Information [NCBI] BioSample SAMN09488305); and was generated with Lyve-SET version 1.1.4f (Katz et al., 2017). Sequence data were uploaded to the NCBI Pathogen Detection database (Davis et al., 2015; National Center for Biotechnology Information, 2016).
Results
Epidemiologic investigation
A total of 26 outbreak-associated ill persons were identified from Colorado (1), Delaware (2), Louisiana (2), Maryland (15), New York (1), Pennsylvania (1), Virginia (1), and the District of Columbia (3) (Fig. 1). The illness onset dates ranged from April 1, 2018, to July 19, 2018 (Fig. 2). Ill people ranged in age from 26 to 78 years, with a median age of 55 years, and 54% were male. Among 25 people with available information, 9 (36%) were hospitalized and no deaths were reported. Of the 24 people interviewed about their food exposure, 22 (92%) reported eating crabmeat in homes or restaurants.

Outbreak-associated ill people with vibriosis, by jurisdiction of residence (n = 26).
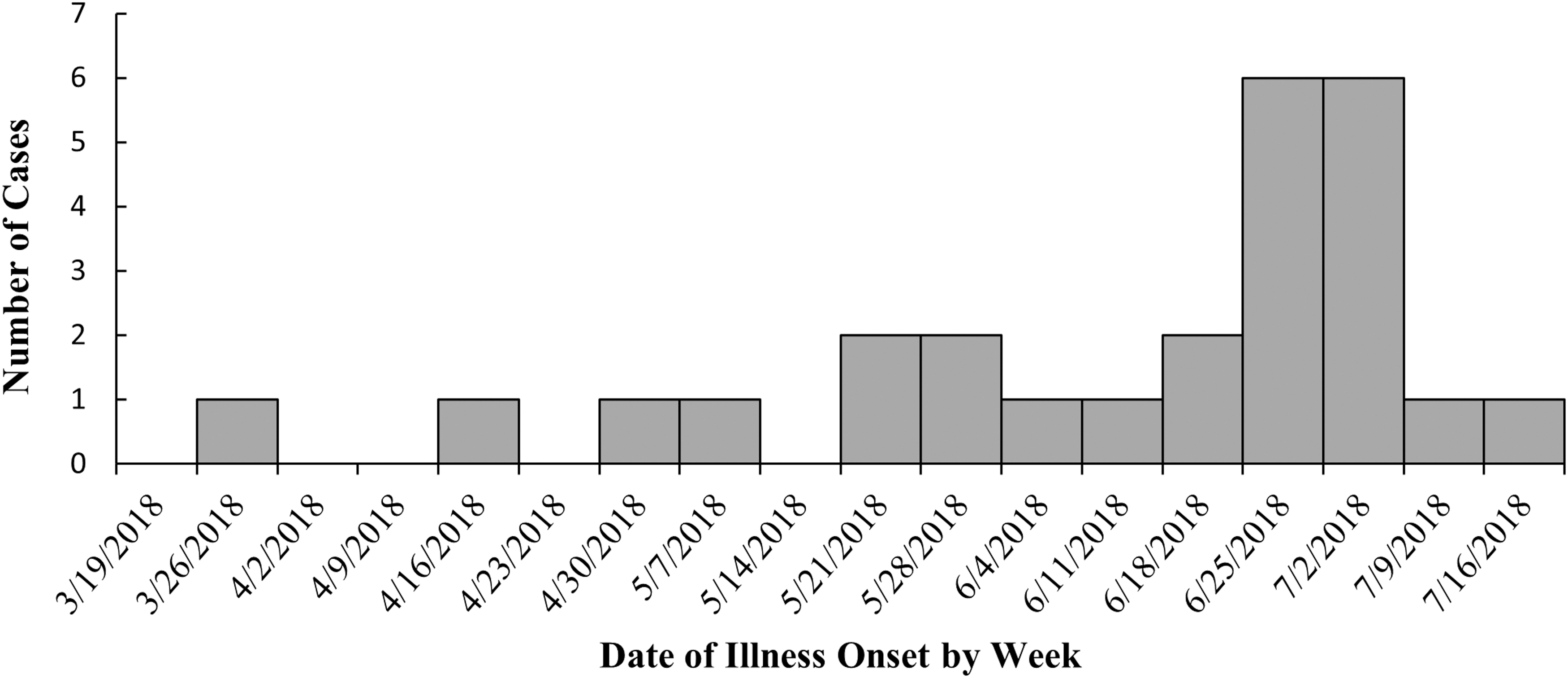
Outbreak-associated ill people with vibriosis, by week of illness onseta (n = 26). aWeek is based on the date of illness onset when available. When unavailable, date of specimen collection was substituted to provide an approximation of the date of illness onset.
Laboratory investigation
Eighteen (69%) outbreak-associated clinical isolates collected by local and state partners were identified through PulseNet; 17 (65%) shared one of the outbreak strain's PFGE pattern combinations and one (4%) did not undergo PFGE testing but had WGS results that were closely related to the other 17 (Fig. 3). These 18 outbreak-associated clinical isolates were related to each other by 0–16 SNPs, with most isolates closely related at 0–7 SNPs apart (Fig. 3) (Jackson et al., 2016; Katz et al., 2017; Pightling et al., 2018). These isolates were compared with historical isolates with similar PFGE pattern combinations; historical isolates were found to be less related to the outbreak isolates, at up to 25 SNPs apart (Fig. 3). V. parahaemolyticus clinical isolates from the eight other ill people that were included in the outbreak did not have PFGE or WGS test results available.

PFGE and WGS results for clinical Vibrio parahaemolyticus isolates from outbreak-associated ill people.
FDA samples
FDA collected 25 samples of crabmeat, 11 from a domestic distributor and 14 import samples (Table 1). V. parahaemolyticus isolates were not recovered from FDA samples. FDA import sampling recovered Salmonella spp. and Listeria monocytogenes isolates from three and two samples, respectively. WGS analysis showed that none of these isolates from crabmeat matched the clinical isolates at the time of analysis. The two Salmonella Infantis isolates were 15 SNPs apart from each other and were recovered from samples manufactured by two different firms, but both from the same geographic area of Venezuela (data not shown).
Summary of Venezuelan Crabmeat Samples Collected in Response to 2018 Outbreak of Vibrio parahaemolyticus
The limit of detection for this method is 0.3 MPN/g. The acceptable regulatory limit of nondetectable is <0.3 MPN/g.
FDA, U.S. Food and Drug Administration; MPN, most probably number; ND, not detected; NIIFT, not included in final traceback; NT, not tested.
State and district samples
The MDH collected six samples consisting of multiple brands of crabmeat from one seafood distributor (Table 1) and recovered 22 isolates of V. parahaemolyticus from four of the samples. Seven of the 22 isolates were tdh-positive and forwarded for PFGE and WGS analysis, but none matched the outbreak strain (data not shown). The tlh gene was detected in isolates recovered from all six samples, while the tdh gene was detected in isolates from two samples. Because the tdh gene was found in all the outbreak clinical isolates, 23 additional isolates from the two samples resulting in tdh-positive isolates were tested for the tdh gene, but it was not detected. The District of Columbia Department of Health (DC Health) collected and analyzed one sample from a seafood distributor identified in the traceback investigation but did not recover V. parahaemolyticus (data not shown).
Traceback and firm investigations
A traceback investigation was completed for seven ill persons who reported purchasing fresh lump or jumbo lump crabmeat at six points of service (POS), either a retail location or restaurant in Maryland or Washington, DC (Fig. 4). Five of six POS included in the traceback investigation received only Venezuelan crabmeat during the time frame before ill persons' purchase or meal. The traceback identified 10 U.S.-based suppliers of Venezuelan crabmeat to four distribution centers (Distributors A, B, D, and E). At least nine Venezuelan packers provided crabmeat to 13 Venezuelan shippers who provided crabmeat to the United States. Multiple Venezuelan packers and shippers provided multiple brands of crabmeat to at least two U.S. importers (Distributors F and G). SMarRRT, DC Health, and FDA traceback evidence indicated that fresh crabmeat from Venezuela was the common exposure among ill persons.

Traceback diagram for multistate outbreak of Vibrio parahaemolyticus infections associated with consumption of fresh crabmeat from Venezuela in 2018. Purchases of implicated products are traced from the point of service, through the distribution chain, to distributors and importers. Product originates from the foreign packers, denoted on the right side of the diagram. *Located in Venezuela.
A review of the Venezuelan processor's hazard analysis and critical control point plans identified critical limits at the cook step that would eliminate V. parahaemolyticus in fresh crab. Investigators did not identify a sole Venezuelan manufacturer or U.S.-based distributor that would account for all the ill persons of the traceback investigation.
The MDH investigated four POS reported by ill persons and three distribution centers identified through traceback. DC Health investigated a distribution center identified through traceback and investigated three POS in DC associated with two ill persons. The FDA investigated 10 domestic distributors and importers of the product. Conditions at distribution centers did not account for the contamination, as the containers of crabmeat were reportedly sealed during packaging in Venezuela. Importer and processor records included private laboratory results for several fresh crabmeat samples that showed detectable levels of V. parahaemolyticus and food safety documents incorrectly listing a limit for V. parahaemolyticus that was higher than the acceptable nondetectable limit for cooked, RTE crabmeat. Industry representatives were reminded that cooked crabmeat should not have any detectable level of Vibrio spp.
Public health actions
The outbreak investigation prompted increased sampling of crabmeat from Venezuela and as a result of the subsequent recovery of pathogens, four Venezuelan firms were placed on Import Alert 16–81 for Salmonella (Packer G and Distributor C) or 16–39 for L. monocytogenes (Distributor U and an additional firm) (Fig. 4) (U.S. Food and Drug Administration, 2018b; U.S. Food and Drug Administration, 2018c).
Public communication
On July 6, 2018, the MDH issued a media advisory warning people to avoid eating fresh crabmeat imported from Venezuela. On July 13, 2018, the FDA and CDC posted initial web advice providing similar recommendations (U.S. Centers for Disease Control and Prevention, 2018b; U.S. Food and Drug Administration, 2018a). DC Health publicized the MDH media advisory and on July 15, 2018, distributed a Health Notice for DC Healthcare Providers. On September 27, 2018, the CDC and FDA finalized their web postings to include recommendations for consumers, restaurants, and retailers to consider using pasteurized crabmeat or fully recooking fresh crabmeat, particularly for items served cold.
Discussion
This multistate V. parahaemolyticus outbreak investigation identified RTE crabmeat as the source of illness, demonstrating the potential for crabmeat to serve as an outbreak vehicle for V. parahaemolyticus in addition to the more commonly implicated bivalve molluscan shellfish. Similar to most reported cases of foodborne V. parahaemolyticus, most reported illnesses in this outbreak were not severe. Completion of a COVIS seafood investigation for each seafood exposure reported by the ill person as part of the standard case report form is necessary for successful identification of V. parahaemolyticus outbreaks, irrespective of the severity of the illnesses.
Although some reported ill people were clustered within a state or linked to common POS, laboratory testing with PFGE/WGS allowed public health officials to link additional related ill people from eight states. These ill people were identified through their related sequences, and the traceback and epidemiologic findings from them confirmed crabmeat as the common food source. In addition to typical underreporting challenges, increased use of culture-independent diagnostic tests (CIDT) to detect Vibrio spp. infections in recent years may have limited investigators' ability to identify all associated ill people in this outbreak. Culture confirmation and WGS should be completed for all specimens identified by CIDT as positive for Vibrio spp. Additional evaluation of WGS as a tool for identification of related ill people with vibriosis would help determine the most appropriate use of and prioritization for WGS by public health laboratories.
While the traceback investigation for this outbreak did not identify a sole Venezuelan manufacturer or U.S.-based distributor accounting for all ill persons, a single source may still have been responsible for the outbreak. Alternatively, it is possible that multiple processors were supplying contaminated product with a nearly identical strain of V. parahaemolyticus. Both possibilities align with the laboratory results showing a similar strain of Salmonella identified in two different brands of product.
There were multiple challenges in the traceback investigation. Five of the six POS identified by Maryland had a single ill person reporting exposure rather than the ideal three or more ill persons from the same POS (Irvin et al., 2021). Some records collected were not readily understandable due to illegibility of handwritten notes, documents with faint print, language differences, same invoice number on multiple airway bills, dates between documents not aligning, lack of addresses on foreign documents, and differences in how firms are referenced (i.e., “shipper,” “packer,” “supplier”). In some instances, brand names, product description, and amounts of product distributed did not match between documents. For example, a U.S. firm created a lot number from the airway bill number, however, a shipment could consist of multiple brands or a product from multiple packers. Several U.S. distributors and POS did not maintain brand and lot information for shipments.
During the incident, the U.S. Department of State was operating under a “Do Not Travel” advisory for U.S. government employees to Venezuela. In addition, at the time of the investigation, FDA did not have a cooperative agreement or other diplomatic relations with the competent authorities in Venezuela. Therefore, FDA investigators were unable to gather additional firm-specific information or observe processing facilities for potential routes of contamination at foreign firms.
Cooked RTE crabmeat with the presence of Salmonella, L. monocytogenes, or V. parahaemolyticus is adulterated under Section 402 (a)(1) of the Federal Food, Drug and Cosmetic Act, as it contains a poisonous or deleterious substance, which may render it injurious to health. FDA has the authority to refuse product offered for import into the United States if it appears from the examination of samples, or otherwise, that the product is adulterated [21 U.S.C. 381(a)]. Since “fresh” crabmeat is cooked, the presence of pathogens (e.g., Salmonella, L. monocytogenes, or V. parahaemolyticus) indicates that the cooking step was inadequate and/or that cross-contamination from insanitary conditions occurred after cooking. Pasteurization can be used to confer a food safety advantage over other methods, extend shelf-life of crabmeat, and is typically done after packaging.
Whether pasteurized or not, crabmeat products should not contain detectable levels of pathogens because both are required to be processed with heat treatment and sanitation controls. FDA engaged U.S.-based firms involved in the outbreak investigation to discuss pasteurization; alternatively, high-pressure processing (HPP) and irradiation were proposed by the involved firms as possible pathogen control options. In the case of HPP, it was implemented for some “fresh” crabmeat products during the time of the outbreak investigation. U.S.-based crab processors were informed that any importer or firm receiving cooked crabmeat with the presence of V. parahaemolyticus is receiving an adulterated product. Furthermore, any postcook processing such as HPP or irradiation of adulterated product would be considered reconditioning. Reconditioning proposals are needed to address all reasonably likely-to-occur hazards, including pathogen hazards from cross-contamination. Manufacturers should not use postcook processing such as HPP or irradiation instead of cooking and sanitation controls.
The FDA web postings included a new section for processors and distributors highlighting FDA's Bacteriological Analytical Manual (BAM) explicitly stating that “a heat-processed product should not contain viable V. parahaemolyticus and if so, would indicate a significant problem in manufacturing practices or post-process contamination” (DePaola et al., 2004). The new section explained that V. parahaemolyticus is an extremely heat-sensitive pathogen that will become nondetectable after a food is properly cooked and that previous outbreaks linked to cooked RTE crabmeat were associated with insanitary conditions after cooking. Also highlighted were the relevant guidance and regulation for sanitation procedures that include prevention of cross-contamination.
The update provided clarification for a “safety level” for V. parahaemolyticus that was listed in Appendix 5 of FDA's Fish and Fishery Products Hazards and Controls Guidance (U.S. Food and Drug Administration, 2020). Previously, Appendix 5 recommended a safety level of 1 × 104/g for “Ready-to-Eat Fishery Products (Minimal cooking by consumer).” During the investigation, there was discussion with industry as to whether cooked crabmeat should be considered in this category. Industry representatives were informed that this category of products was intended to describe raw, RTE products, such as oysters and other molluscan shellfish, because the safety level originated from the National Shellfish Sanitation Program “Guide for the Control of Molluscan Shellfish.”
As of March 2020, and due to discussions with industry during the outbreak, Appendix 5 was updated to clarify that previously cooked fish, including crustaceans such as crabs, should not have detectable levels of Vibrio spp., and that raw bivalve shellfish should not have ≥1 × 104/g V. parahaemolyticus (U.S. Food and Drug Administration, 2020). This updated distinction should limit future misinterpretations.
Conclusions
This vibriosis outbreak was first linked to processed crabmeat in the United States since 1971 and the first multistate outbreak of vibriosis linked to any crab product reported to CDC. This outbreak provided evidence of postcook cross-contamination from insanitary practices of packaged and processed crabmeat. The traceback investigation highlighted that significant challenges following the product throughout the supply chain and travel restrictions between the United States and Venezuela made FDA on-site inspections of cooked crabmeat processors impossible. While some challenges limited the scope of the investigation, epidemiologic, traceback, and laboratory evidence identified the contaminated commodity and country of origin, and informed actions that prevented additional illnesses.
Footnotes
Acknowledgments
The response efforts to this outbreak included federal, local, and state officials and laboratories including the MDH, the Maryland Rapid Response Team, and the DC Health, who were crucial in this investigation. Special thanks to Eric Keller from the MDH Laboratories Administration, as well as our partners from the Delaware Division of Public Health, the Pennsylvania Department of Health, and the New York City Department of Health and Mental Hygiene for their contributions to the investigation.
Authors' Contributions
S.L.S.: investigation, conceptualization, and writing—original draft preparation. B.M.W.: investigation, writing, and reviewing and editing. E.K.S.: conceptualization, writing, and reviewing and editing. E.L.E.: writing and reviewing and editing. K.P.: investigation and reviewing and editing. T.G.: investigation and reviewing and editing. S.B.: reviewing and editing. J.L.J.: writing and reviewing and editing. Je.C.: writing and reviewing and editing. Ja.C.: reviewing and editing. Y.L.: data analysis and reviewing and editing. D.L.W.: investigation and reviewing and editing. M.M.B.: investigation and reviewing and editing. J.C.: investigation and reviewing and editing. C.B.: investigation and reviewing and editing. L.M.W.: investigation and reviewing and editing. V.M.G.: investigation and reviewing and editing. S.S.: investigation and reviewing and editing. A.J.C.: investigation and reviewing and editing. M.C.B.: writing and reviewing and editing. S.V.: conceptualization, writing—original draft preparation, and reviewing and editing.
Disclaimer
The findings and conclusions of this report are those of the authors and do not necessarily represent the official position of the Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC).
Disclosure Statement
All authors declare that they have no conflicts of interest.
Funding Information
The authors received no financial support for the research, authorship, and publication of this article.