
Abstract
Campylobacter is one of the leading causes of bacterial foodborne diarrheal diseases throughout the world. Reported outbreaks of Campylobacter are infrequent in China. This article described such an outbreak among students from a junior high school in East China during November 2019. A total of 40 samples were collected as follows: 24 stool samples from patients, 12 stool samples from kitchen staff members, and 4 water samples from cafeteria. The stool samples were tested for the presence of Salmonella, enterotoxigenic Escherichia coli, Shigella, Vibrio parahaemolyticus, Vibrio cholera, Listeria monocytogenes, Staphylococcus aureus, Yersinia enterocolitica, Bacillus cereus, Clostridium perfringens, norovirus, rotavirus, adenovirus, astrovirus, and sapovirus by real-time polymerase chain reaction (PCR). Pulsed-field gel electrophoresis (PFGE), next-generation sequencing, and antimicrobial susceptibility testing were performed to determine the relatedness of the Campylobacter jejuni isolates in this outbreak. Forty-seven cases were reported with diarrhea among 569 seventh grade students and staff. In these 47 cases, we detected that C. jejuni through real-time PCR in 16 fecal samples was positive, whereas the remaining fecal samples were tested negative by real-time PCR. Only three C. jejuni strains were isolated from stool samples of case patients, and all of them showed 100% PFGE similarity to strain ST6913. Whole genome sequencing analysis revealed no single nucleotide variation in the three isolates. This is one of the few reports in China about outbreak caused by C. jejuni. C. jejuni ST6913 was responsible for this outbreak.
Keywords
Introduction
Campylobacter spp. are a primary cause of bacterial foodborne diarrheal diseases globally, with most human campylobacteriosis cases being infected by Campylobacter jejuni (C. jejuni) (Costa and Iraola, 2019; Kaakoush et al., 2015). Typical symptoms of a Campylobacter infection include diarrhea, fever, and abdominal pain, which may be accompanied by nausea and vomiting. In addition, Campylobacter infection may give rise to the development of sequelae beyond gastroenteritis, such as reactive arthritis, Guillain–Barré syndrome (GBS), and irritable bowel syndrome (Moffatt et al., 2017; Willison et al., 2016).
C. jejuni usually transmits to humans through the consumption of poultry meat, raw milk, other insufficiently heated meat, and contaminated water (Burakoff et al., 2018; Karki et al., 2018; Kuhn et al., 2017; Pergola et al., 2017). C. jejuni infection is the predominant bacterial etiology of diarrheal illness in the United States (Tack et al., 2019). Data from the Foodborne Diseases Active Surveillance Network indicate that about 20 cases are diagnosed each year for every 100,000 people (Tack et al., 2019). And C. jejuni infection is also the most commonly reported foodborne illness in the European Union (2018). It was reported to cause 64.9 cases per 100,000 populations in 2017 (2018). The mandatory reporting of C. jejuni is not currently enforced in China; however, the National Public Health Emergency Event Surveillance System (PHEESS) has been monitoring significant and/or severe outbreaks, including those attributed to C. jejuni, since 2004. Nevertheless, the rarity of campylobacter-induced outbreaks in China can be attributed to the sporadic nature of most human campylobacter disease cases (Qu et al., 2019; Taylor et al., 2013; Zhang et al., 2010).
For the past decade, pulsed-field gel electrophoresis (PFGE) has been the standard method of subtyping outbreaks (Lahti et al., 2017). Next-generation sequencing (NGS) provides more detailed and precise data for identifying outbreaks than PFGE (Duarte et al., 2016). Instead of only having the ability to compare bacterial genomes using 15–30 bands that appear in a PFGE pattern, NGS has millions of bases to compare. Using NGS, some bacteria appeared to be different for which PFGE would appear from the same source. This has helped solve some outbreaks sooner.
According to the PHEESS and the local school health surveillance system, many students from a junior high school had acute diarrhea from November 14, 2019 to November 18, 2019. Sixteen cases were confirmed for C. jejuni, and three C. jejuni isolates were collected. The aim of this study is to describe both the epidemiological and genomic characterization of the C. jejuni outbreak in China using PFGE and NGS technologies (Llarena et al., 2017).
Materials and Methods
Epidemiological investigation
The outbreak was located at a junior high school in Lishui, an inland city in eastern China. The average daytime temperature of Lishui in November is 21°C. The junior high school was a boarding school from the 7th to 9th grades with a total of 36 classes, 1596 students, 167 staff, and 3 cafeterias. Each of the 3 cafeterias is designated for only one grade from the 7th to the 9th. Forty-seven cases were reported with diarrhea, and all the cases were students from seventh grade. The 7th grade has 12 classes, 534 students, 23 teachers, and 12 kitchen staff.
Someone who received a positive test for C. jejuni by polymerase chain reaction (PCR) test was considered as a confirmed case. Anyone who had diarrhea between November 14, 2019 and November 18, 2019 at this school without having a stool sample or either a positive test was considered as a probable case.
Sample collection and strain isolation
Twenty-four students went to hospitals and left stool samples (Table 1). Stool samples from the 24 students and the 12 cafeteria staff were tested for the presence of Salmonella, enterotoxigenic E. coli, Shigella, Vibrio parahaemolyticus, Vibrio cholera, Listeria monocytogenes, Staphylococcus aureus, Yersinia enterocolitica, Bacillus cereus, Clostridium perfringens, Campylobacter jejuni, norovirus, rotavirus, adenovirus, astrovirus, and sapovirus by real-time fluorescent PCR kits (Mabsky Bio-Tech Co., Ltd, Shenzhen, China) following the manufacturer’s instructions. Since food leftovers were not available, four direct drinking water samples from seventh grade cafeteria were collected and tested for Campylobacter spp.
Sample Information and Detection Results in the Campylobacter jejuni Outbreak, Lishui, 2019
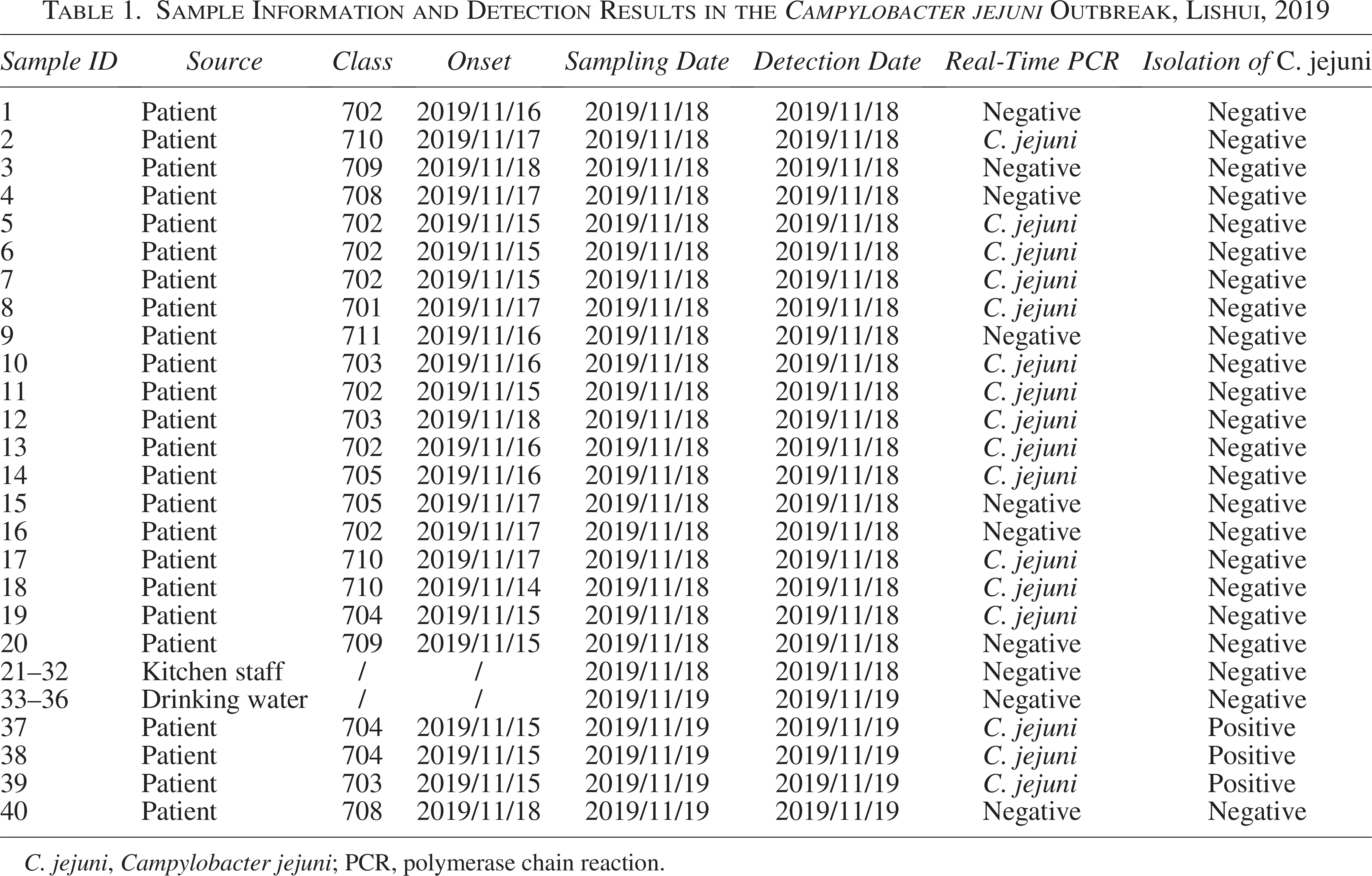
C. jejuni, Campylobacter jejuni; PCR, polymerase chain reaction.
For Campylobacter spp. collection, all specimens were pre-enriched with Preston selective broth (Oxoid Ltd, Basingstoke, UK) with Campylobacter growth supplement (Oxoid Ltd, Basingstoke, UK), selective supplement (Oxoid Ltd, Basingstoke, UK), and 5% sterile defibrinated sheep blood. Samples were incubated at proper conditions of 42°C, 5% O2, 10% CO2, and 85% N2 for 24 h. Five 20-μL drops of the pre-enrichment (100 μL total) were applied to the 0.45 μm pore-size filter, which was left on the surface of a Columbia blood agar plate. After 20 min, the filter was discarded. The plates were incubated at 37°C under microaerobic conditions for 48 h. Suspected Campylobacter colonies were identified by Gram stain, matrix-assisted laser desorption ionization-time of flight mass spectrometry, 16S rRNA gene sequencing, and API Campy identification system test (API Biomerieux, Vercieu, France).
PFGE typing, whole genome sequencing, and bioinformatic analysis
The PFGE method was performed for all C. jejuni isolates following the PulseNet standardized protocol (Ribot et al., 2001). The specific operation methods (including PFGE and whole genome sequencing [WGS]) were the same as our previous research (Chen et al., 2020). Core genome multilocus sequence typing (cgMLST) results were derived from using the C. jejuni/C. coli cgMLST scheme v 1.0, a cgMLST scheme of 1,343 loci, in the C. jejuni/C. coli PubMLST database (http://pubmlst.org/campylobacter). Distance matrices calculated for cgMLST were used in SplitsTree to create phylogenetic trees ( Huson and Bryant, 2006). Core genome single-nucleotide polymorphism analysis was performed with Snippy v4. MEGA7 was used to visualize the trees (Kumar et al., 2016).
Antimicrobial susceptibility testing
The minimum inhibitory concentrations (MICs) of 11 antimicrobials (erythromycin, azithromycin, nalidixic acid, ciprofloxacin, gentamicin, streptomycin, chloramphenicol, florfenicol, tetracycline, telithromycin, and clindamycin) were determined for all C. jejuni isolates using a Campylobacter Agar Dilution Method (MIC) Detection Kit (Qingdao Zhongchuang Biotechnology Co., Ltd., Qingdao, China).
The breakpoints for resistance used in this study were those with a MIC value greater than or equal to the standard values used in the National Antimicrobial Resistance Monitoring System (NARMS-2014) for Campylobacter in the United States as follows: erythromycin (≥32 μg/mL), azithromycin (≥8 μg/mL), nalidixic acid (≥64 μg/mL), ciprofloxacin (≥4 μg/mL), gentamicin (≥8 μg/mL), streptomycin (≥16 μg/mL), chloramphenicol (≥32 μg/mL), florfenicol (≥8 μg/mL), tetracycline (≥16 μg/mL), telithromycin (≥16 μg/mL), and clindamycin (≥8 μg/mL). C. jejuni ATCC 33560 was used as a control.
Results
Epidemiological investigation
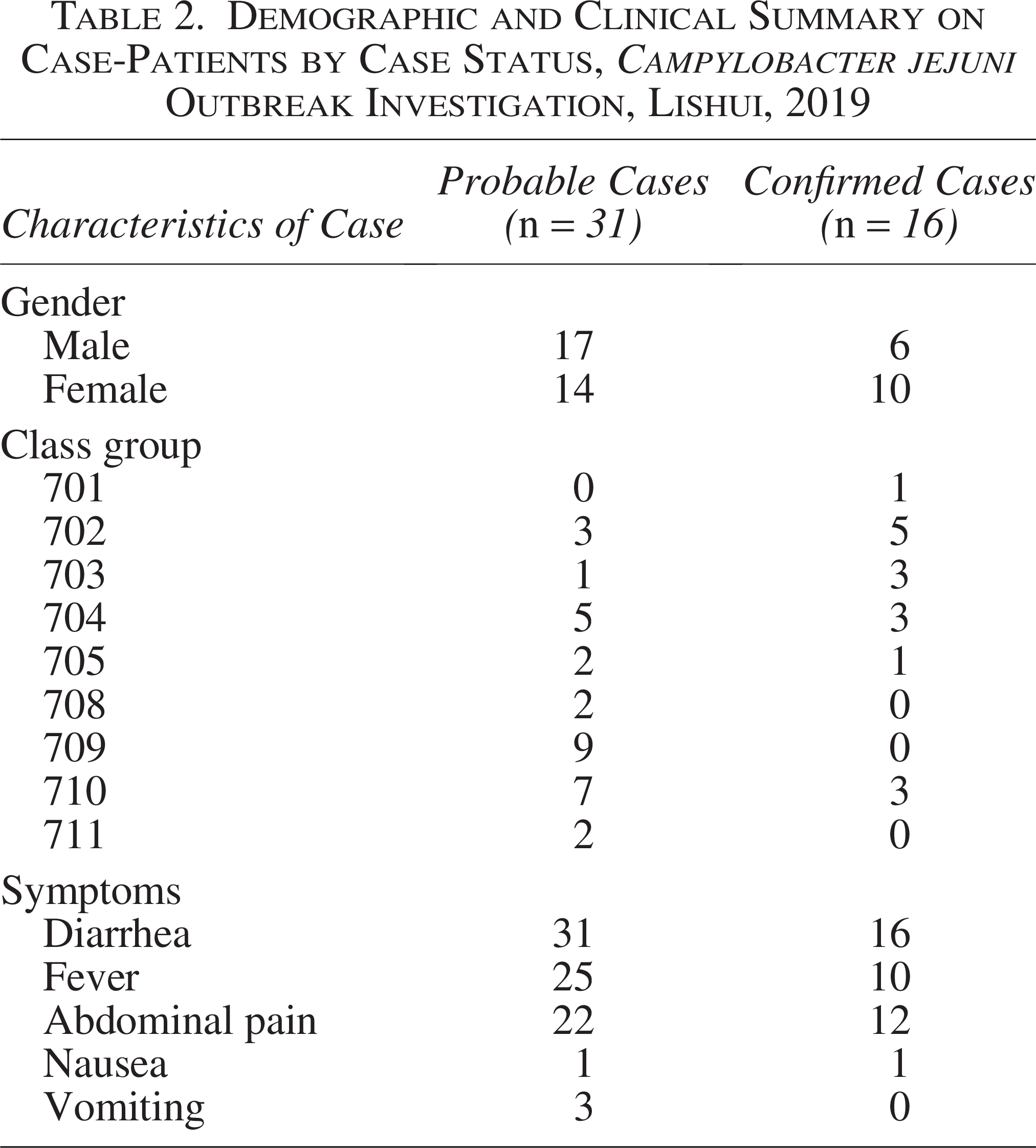
From November 14, 2019 to November 18, 2019, a total of 47 cases were identified in this outbreak, and none of the staff members reported gastrointestinal illnesses. Among them, 16 patients were considered as confirmed cases because they were tested positive for C. jejuni, whereas other cases were considered as probable cases. Illness onset occurred during November 14–18, 2019. Most of the cases began their symptoms on November 15th and 17th (Fig. 1). All of the patients (confirmed and probable) were in seventh grade from nine respective classes. Among 47 cases, 23 (48.9%) were male, and the most frequent symptoms included diarrhea (100.0%), fever (74.5%), and abdominal pain (72.3%) (Table 2).

Number of Campylobacter cases (confirmed and probable) by onset dates during an outbreak in a school in Lishui, 2019.
Demographic and Clinical Summary on Case-Patients by Case Status, Campylobacter jejuni Outbreak Investigation, Lishui, 2019
Microbiological analysis
Stool samples collected from 24 probable cases and 12 kitchen staff members were negative for Salmonella, enterotoxigenic E. coli, Shigella, V. parahaemolyticus, V. cholera, L. monocytogenes, S. aureus, Y. enterocolitica, B. cereus, C. perfringens, norovirus, rotavirus, adenovirus, astrovirus, and sapovirus. In all 24 stool samples from patients, 16 cases were positive for C. jejuni by real-time PCR. In addition, samples from canteen staff and drinking water samples tested negative.
PFGE was performed for all isolates (Fig. 2). Three isolates from confirmed cases (LSH19-01, 2, 3) showed 100% PFGE similarity and were different from all other analyzed strains. Namely, all other strains from the local PFGE database showed a PFGE similarity <60% to the outbreak strains.
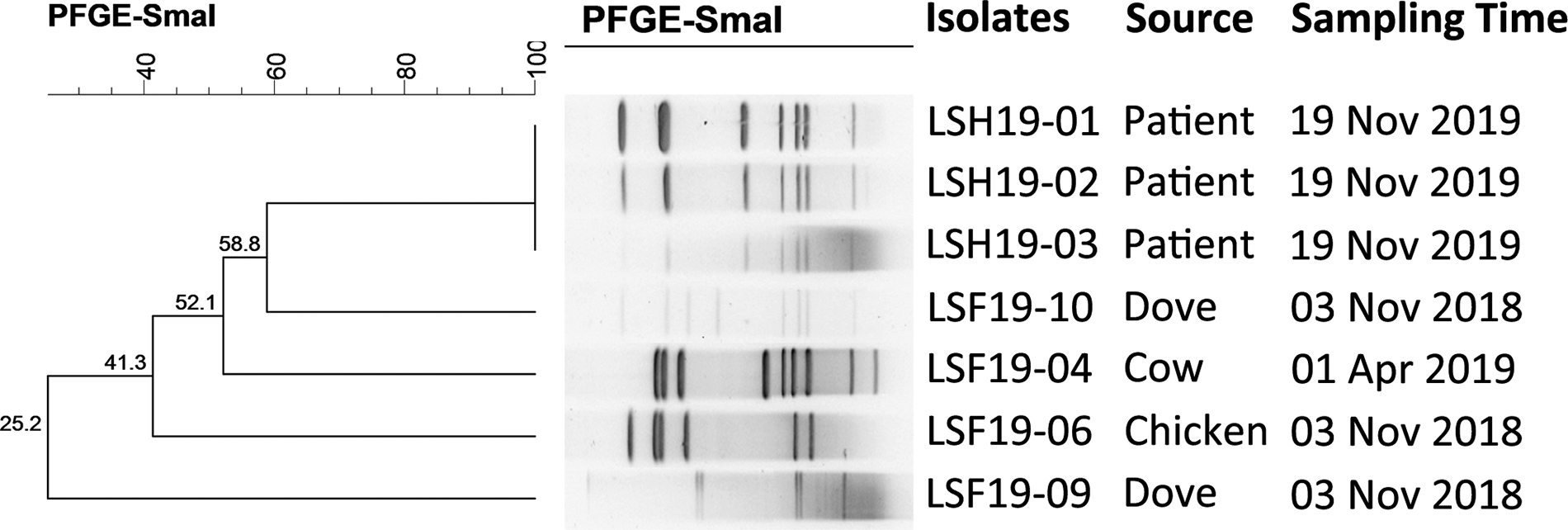
PFGE (pulsed-field gel electrophoresis) pattern and origin of the samples, which tested positive for Campylobacter jejuni during an outbreak in a school in Lishui, 2019.
Three outbreak isolates (LSH19-01, 2, 3) and local PFGE database isolates were included in the WGS analysis (Fig. 2). The cgMLST analysis showed that three case-patient isolates were generally clustered together sharing >99% similar alleles (Fig. 3). Core SNP analysis showed that no SNPs separated the three human outbreak isolates (LSH19-01, 2, 3), which differed by 100–7942 SNPs from the local food isolates (LSH19-04, 6, 9, 10) and 117–217 SNPs from PubMLST database ST6913 isolates (ID-81317 and ID-101233) (Fig. 4). According to the MLST alleles extracted from WGS data, three outbreak isolates represented the same ST6913.
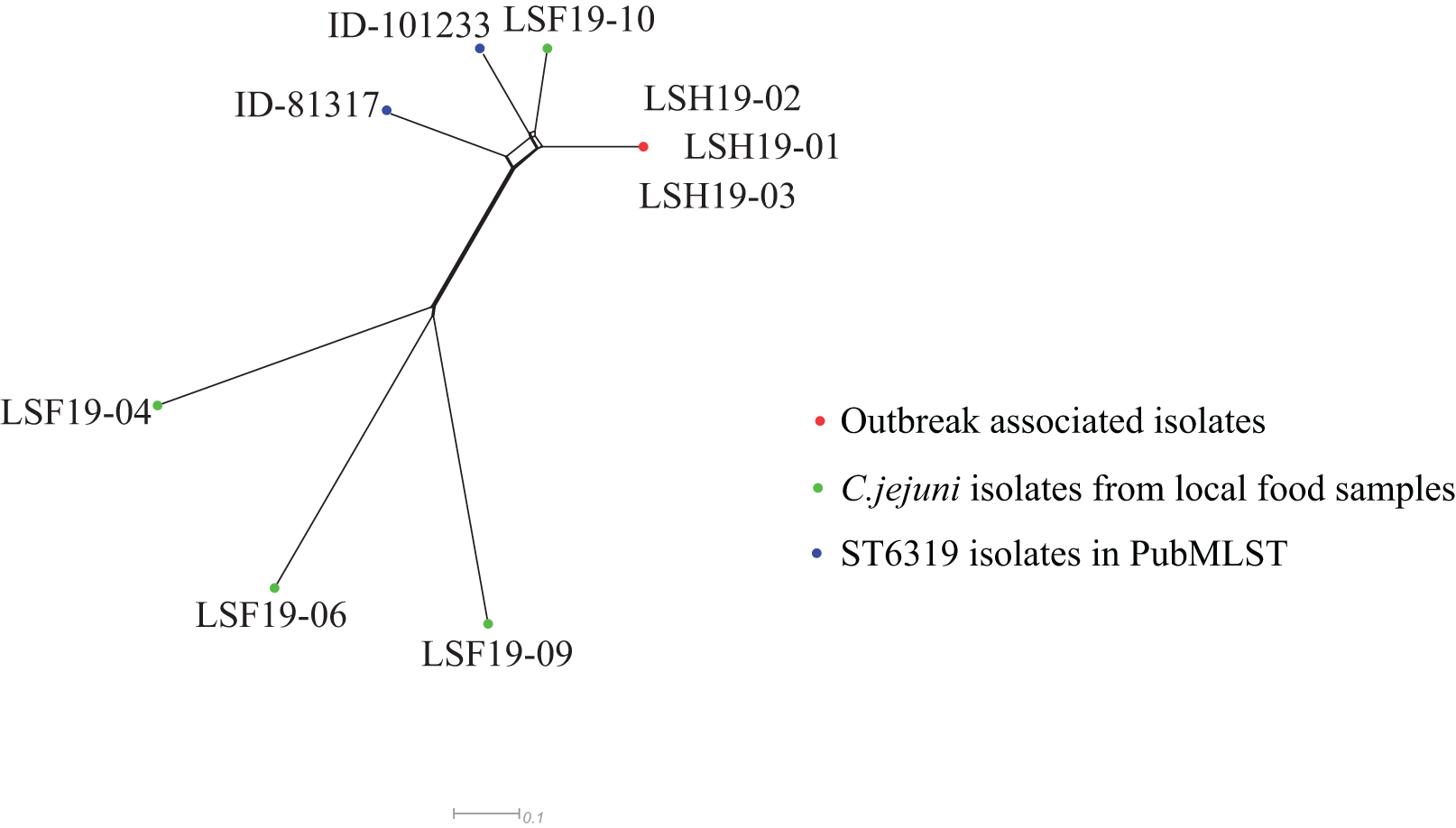
Results of the core genome multilocus sequence typing (cgMLST) among Campylobacter jejuni analysis during an outbreak in a school in Lishui, 2019.

Results of the core genome single-nucleotide polymorphism (cgSNP) among Campylobacter jejuni analysis during an outbreak in a school in Lishui, 2019.
Antibiotic susceptibility
Antibiotic susceptibility tests were performed for a total of seven isolates, including three outbreak strains and four strains isolated from food preserved in our laboratory. Three outbreak strains of C. jejuni were susceptible to 11 tested antimicrobials, including erythromycin, azithromycin, nalidixic acid, ciprofloxacin, gentamicin, streptomycin, chloramphenicol, florfenicol, tetracycline, telithromycin, and clindamycin (Supplementary Table S1).
Discussion
Outbreaks of C. jejuni are rare in China. In June 2007, the first outbreak was reported in a small town in northern China, resulting in 36 cases of GBS among 117 diarrheal cases (Zhang et al., 2010). The second C. jejuni outbreak was reported in a high school in Beijing in 2018. After a trip to Southern China, 36 students suffered diarrhea and vomiting (Qu et al., 2019). In 2019, a previous outbreak had been noticed in a school in Hangzhou, a city 200 km from Lishui. A total of 84 cases were involved, including 15 confirmed and 69 probable cases (Yu et al., 2020). Between 1999 and 2008, 4936 Campylobacter outbreaks were reported by the Centers for Disease Control and Prevention (CDC) in the United States (Batz et al., 2012). Fifty-six confirmed and 13 suspected outbreaks were recorded in the U.S. National Outbreak Reporting System between 2009 and 2010. Of these, 1550 illnesses and 52 hospitalized cases were reported (Hall et al., 2013). A total of 143 outbreaks were reported in England and Wales, United Kingdom between 1992 and 2009, among which 114 cases of infection were transmitted through food, 5 cases were transmitted through humans, 2 cases were transmitted through animals, and 19 cases were transmitted through unknown means of transmission (Little et al., 2010). Large and/or severe outbreaks, including those resulting from Campylobacter, have been monitored by the PHEESS since 2004. Since Campylobacteriosis is not a notifiable disease in China, it may be the reason that Campylobacter outbreaks were rarely reported in China.
The epidemiological curve suggested a common source of exposure. Furthermore, 16 cases were confirmed among 47 cases. PFGE showed that one unique strain being identified among stool specimens that was positive also led us to a common source. Furthermore, WGS revealed no SNP variation between the outbreak-associated isolates. This indicated a very close genetic relationship among the isolates, further supporting the common source described above.
The rates of salmonellosis and campylobacteriosis have apparently increased around the world in the last decade (2018, Tack et al., 2019). The rise is largely attributed to a shift in eating habits, with consumption of raw or undercooked chicken (Rosenberg Goldstein et al., 2016). This shift in eating habits may have developed without fully understanding the potential risks of raw or undercooked foods, as evidenced by the rapidly expanding number of chickens, veal, or beef liver associated campylobacteriosis outbreaks (Gaulin et al., 2018; Glashower et al., 2017; Lahti et al., 2017; Moffatt et al., 2016). According to a meta-analysis of major foodborne pathogens in Chinese food commodities, Campylobacter ranks second in terms of prevalence with an overall average prevalence of 10.8% (Paudyal et al., 2018). The junior high school was a boarding school, and all of the cases were students from the seventh grade. Furthermore, there is a cafeteria that only serves the seventh grade, which indicates that it might be an outbreak associated with contaminated foods.
MLST results showed that the outbreak strain belongs to a distinct sequence type (ST6913), which is rare. In 2011, ST6913 was first isolated from children with diarrhea in Shanghai (the ID in the Campylobacter jejuni/coli PubMLST database is 25691), a city next to Zhejiang Province (Pan et al., 2016). ST6913 isolates have also been found in the United States (the IDs in the Campylobacter jejuni/coli PubMLST database are 81317 and 101233). The results of this investigation suggest that ST6913 may result in outbreaks of foodborne diseases or sporadic human diarrhea.
The MLST phenotype is completely different compared with the local (Hangzhou, Zhejiang) outbreak strains, which belong to ST2988 and ST8149 (Yu et al., 2020). It showed great diversity in the MLST phenotype, as widely documented in other countries (Oh et al., 2017; Zeng et al., 2016).
In conclusion, we reported that the C. jejuni epidemic clone ST6913 was responsible for this outbreak, and this is one of the few reports about outbreaks caused by C. jejuni in China.
Authors’ Contributions
X.C., M.Z., H.C., and Y.G. conceived and designed the works. J.M. and Y.L. performed the experiments. X.C. and Y.J. completed the writing and translation of the article. J.M., Y.L., and B.Y. completed the data analysis and interpretation of the article. All authors read and approved the final article.
Footnotes
Funding Information
This work was supported by the
Ethics Approval
This study was supported by the Ethics Committee of Zhejiang People’s Hospital (Ethics Committee Approval of Biomedical Research Involving Humans, Approval No.: 2019KY311) and in accordance with the ethical standards of the Declaration of Helsinki.
Availability of Data
The raw sequence dataset is available in the NCBI database with BioProject accession number PRJNA665606.
Disclosure Statement
No competing financial interests exist.