
Abstract
Cystic echinococcosis (CE), the second most significant foodborne parasitic disease worldwide, poses a significant global health burden. Understanding its clinical and laboratory features is crucial for effective management. This study aimed to investigate the epidemiological, laboratory, and clinical characteristics of pediatric CE in an Iranian referral hospital. A cross-sectional study reviewed hospital records of patients with CE admitted to Children’s Medical Center, Tehran, Iran, from 2011 to 2020. Data on demographics, diagnostics, clinical presentation, laboratory findings, and treatment were collected and analyzed. A total of 114 patients, with a mean age of 7.33 ± 2.9 years, were diagnosed with CE. The male-to-female ratio was 1.78, and 73.7% were urban residents. Abdominal pain (69%) and coughing (65%) were the most common symptoms. In confirming the cyst involvement across anatomical sites, pathology emerged as the most reliable method, with effectiveness ranging from 95% to 100%. Abdominal ultrasonography and computed tomography scan were frequently utilized imaging modalities, displaying effectiveness percentages of 71–85%. Liver and lung involvement predominated (66%), with 39% of cases showing multiorgan involvement. Spleen involvement was less common (6%), and neurological involvement was rare (1–2%). The majority of patients (n = 63, 67.7%) displayed cysts larger than 50 mm. All patients received albendazole treatment, and 104 patients (91.2%) underwent surgical procedures, with three postsurgical deaths. In conclusion, hospital records over 9 years indicate an increasing prevalence of CE, emphasizing the need for heightened awareness and effective public health interventions to control this parasitic infection.
Introduction
Cystic echinococcosis (CE), caused by the Echinococcus granulosus, is the second most significant foodborne parasitic disease worldwide (Hogea et al., 2024). Despite its classification as a neglected disease by the World Health Organization (WHO), CE poses substantial public health risks due to its prevalence, particularly in regions such as Eurasia, Australia, Africa, and South America (Grosso et al., 2012; Moldovan et al., 2012). Effective control and prevention strategies, including enhanced animal care practices and public health education, are imperative to mitigate the spread of CE.
The WHO estimates that over one million individuals may be living with CE at any given time, contributing to significant morbidity and mortality worldwide. Pediatric CE remains a significant health concern in developing nations, notably in the Middle East, including Iran (Mahmoudi et al., 2019; Mohammadi et al., 2021). In Iran, CE is recognized as a hyperendemic area, with prevalence rates ranging from 0.61 to 2 per 100,000 population (Rokni, 2008). The predominant genetic variants identified in Iran include the G1 strain, affecting sheep, goats, cattle, and camels, as well as the G6 strain, which affects camelids (Harandi et al., 2002). While asymptomatic cases are common in the early stages of CE infection, symptomatic patients often present with liver and lung involvement, as well as involvement of other organs such as the brain, muscles, kidneys, bones, heart, and pancreas (Frider et al., 1999).
Despite prevalence and the burden of CE, epidemiological studies focusing on pediatric CE have been notably scarce. The lack of recent investigations into pediatric cases in such settings poses a critical gap in understanding the epidemiology, clinical characteristics, and diagnostic approaches specific to this vulnerable population. This study aimed to comprehensively investigate pediatric CE in an Iranian referral hospital in Tehran. It sought to determine the frequency and trends of cases, characterize organ involvement, evaluate symptoms, and assess diagnostic methods and laboratory findings.
Materials and Methods
Patients with hydatid cysts from 2011 to 2020 (except for 2012) were examined and studied at Children’s Medical Center Hospital. The protocol was approved by the Ethics Committee of the Tehran University of Medical Sciences (IR.TUMS.CHMC.REC.1399.041).
Data collection
Hospital records are extracted based on specific disease codes from the International Classification of Diseases (ICD), including 122.9 and 122.8 for ICD-9, and B67.8, K77.0, B67.9, and J99.8 for ICD-10. Data comprised age at diagnosis, gender, rural/urban residency, history of animal contact, family history of hydatid cysts, diagnostic methods used, affected organs, number and size of cysts, clinical and laboratory test results, and treatment received.
Patients diagnosed with CE infection were identified based on a multifaceted diagnostic approach. A positive diagnosis was established if the patient’s blood sample tested positive for anti-echinococcus antibodies, as detected by enzyme-linked immunosorbent assay, indirect hemagglutination antibody test, or indirect fluorescent antibody test. Additionally, clinical characteristics indicative of CE were identified through various imaging techniques, including computed tomography (CT) scan, magnetic resonance imaging (MRI), chest X-ray, ultrasonography, bronchoscopy, and radiology. Furthermore, pathological properties suggestive of CE were assessed through histopathological examination of tissue samples obtained via biopsy or surgical procedures (Mahmoudi et al., 2019).
Laboratory findings encompassed parameters such as aspartate transferase (AST), alanine transferase (ALT), alkaline phosphatase (ALP), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), blood urea nitrogen, creatinine, and complete blood counts.
Statistical analysis
Statistical analysis was done by using the Statistical Package for Social Sciences (SPSS) version. 27.0.1 (SPSS Inc., Chicago, IL, USA). Descriptive data are presented as frequency, percentage, mean, and standard errors in numbers and percentages in the form of tables and graphs. The chi-square test was used in the analysis of nominal variables. Fisher’s exact test was used when the distribution was not compatible with the chi-square test in the analysis of nominal variables. A p value of <0.05 was considered significant.
Results
The study included 114 hospitalized patients presenting with CE from 2011 to 2020, excluding the year 2012. The overall prevalence of CE in our hospital was found to be 0.07% (114 out of 154,993 hospitalized patients), as depicted in Figure 1. Among all the patients, 73 (64%) were male, resulting in a male-to-female ratio of 1.78. The mean age of patients was 7.33 ± 2.9 years, with an age range spanning from 2 to 16 years. Notably, the majority of patients (78.7%) fell within the age range of 5 to 11 years, whereas the frequency decreased in the age-group above 15 years (Table 1). Regarding residential locations, 84 patients (73.7%) originated from urban areas, while 30 patients (26.3%) resided in rural regions. In terms of animal contact history, 80 patients (70.2%) reported previous interactions with dogs or sheep, whereas 34 patients (29.8%) did not mention any such history of contact.
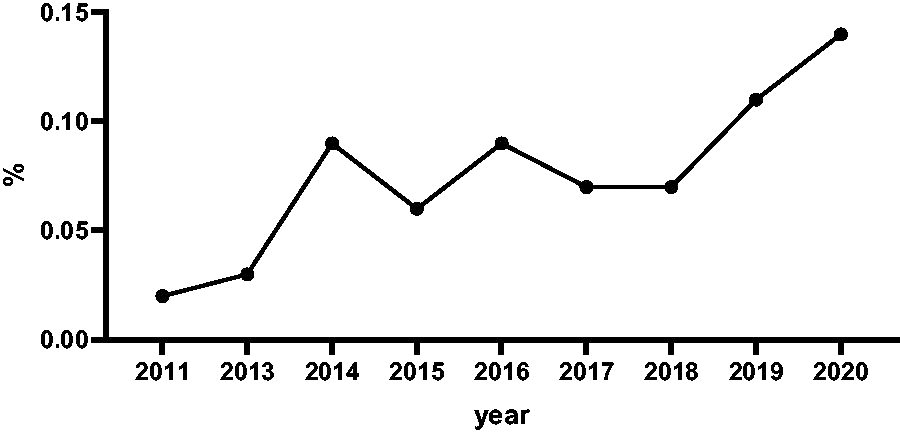
Prevalence of cystic echinococcus in an Iranian referral hospital.
Demographics and Diagnostic Characteristics of the Patients with Cystic Echinococcosis
CT, computed tomography; ELISA, enzyme-linked immunosorbent assay; MRI, magnetic resonance imaging.
Among patients diagnosed with CE, the clinical symptoms reported varied widely, reflecting the diverse presentation of the disease. The most commonly reported symptom was abdominal pain, observed in 69% of cases, suggesting cysts located in abdominal organs such as the liver or spleen. Coughing was the second most prevalent symptom, noted in 65% of cases, potentially indicative of pulmonary involvement. Nausea and vomiting were reported by 26% and 28% of patients, respectively, possibly due to pressure exerted by the cysts or systemic inflammation. Anorexia was observed in 19% of cases, likely resulting from gastrointestinal disturbances caused by the cysts. Tachypnea, a sign of respiratory distress, was less common, noted in 5% of patients. Convulsions and headaches, indicative of neurological involvement, were reported in 1% and 4% of cases, respectively. Additionally, 17% of patients reported other nonspecific symptoms such as fatigue or malaise (Fig. 2).

Clinical symptom presentation in cystic echinococcosis cases.
The distribution of CE across different anatomical sites highlights varying patterns of organ involvement. Liver and lung involvement were predominant, observed in 66% of cases (n = 75). Similarly, a substantial proportion of patients exhibited single lung involvement, noted in 92% of cases (n = 69). Conversely, spleen involvement was less frequent, observed in 6% of cases (n = 7). Brain involvement was detected in 2% of cases (n = 2), indicating the potential for cysts to impact neurological structures. Abdominal involvement was rare, noted in only 1% of patients (n = 1). Additionally, kidney involvement was present in 4% of patients (n = 4). Remarkably, no patients exhibited cysts in the gallbladder or pelvic region (Fig. 3).

The distribution of echinococcosis across different anatomical sites:
Overall, 44 (39%) of patients had multiorgan involvement. The most prevalent combination observed was liver and lung involvement, identified in 39 cases. Spleen, lung, and liver involvement was noted in 5 cases. Additionally, other combinations were observed in smaller numbers, each highlighting the potential for CE to affect various organ systems concurrently (Fig. 3).
Among the patients, ∼25% (n = 28) underwent CE serological testing, with about 75% testing positive for serology (immunoglobulin M [IgM] positive, immunoglobulin G [IgG] positive, or both). Abdominal ultrasonography was utilized in 76% of patients (n = 87), followed by abdominal CT scan, which was employed in 78% of cases (n = 89). Additionally, 91.2% of patients (n = 104) underwent pathology-based diagnostic procedures to confirm the presence of cysts. A small fraction of patients, 3% (n = 3) and 2% (n = 2), utilized brain CT scans and MRI, respectively, for diagnosis (Table 1).
In the diagnostic landscape of CE across diverse anatomical sites, distinct patterns emerge regarding the utilization and effectiveness of various diagnostic modalities. For spleen involvement, abdominal ultrasonography and abdominal CT scan each exhibit a comparable level of utilization, with ∼71% effectiveness in detecting the disease. However, pathology stands out as the most reliable diagnostic method, demonstrating 100% effectiveness in confirming splenic echinococcosis. Lung manifestations of CE present a similar trend, with imaging modalities such as abdominal ultrasonography, abdominal CT scan, and chest X-ray displaying high effectiveness percentages ranging from 77% to 85%, while pathology showed 95% effectiveness. In cases involving the liver, imaging modalities and pathology emerge as the most effective diagnostic methods, with percentages of 76% and 97% effectiveness, respectively. Notably, for peritoneal involvement, abdominal CT scan and pathology are the predominant diagnostic methods, both exhibiting 100% effectiveness. Brain echinococcosis poses unique challenges, with pathology being the sole method showing high effectiveness at 100%, whereas serology and imaging modalities demonstrate lower effectiveness percentages. Lastly, for kidney involvement, abdominal CT scan and pathology prove highly effective, each exhibiting 100% effectiveness, while serology and other diagnostic methods demonstrate varying degrees of utilization and effectiveness (Fig. 4).
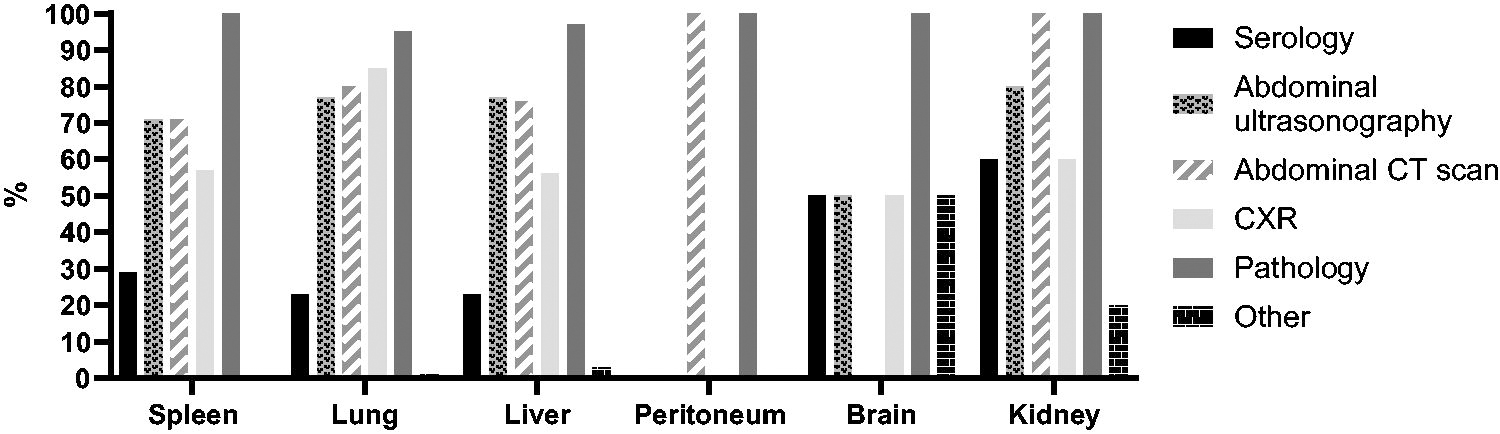
The diagnostic landscape of cystic echinococcosis across diverse anatomical sites.
Among the 114 patients with CE, the distribution of cyst numbers was as follows: 51 patients (44.7%) had one cyst, 26 patients (22.8%) had two cysts, 16 patients (14.0%) had three cysts, 2 patients (1.8%) had four cysts, and 19 patients (16.7%) had multiple cysts, defined as five or more (Table 1). The distribution of cyst sizes revealed that 3 patients (3.2%) had cysts smaller than 25 mm, 27 patients (29%) had cysts sized between 25 and 50 mm, and 63 patients (67.7%) had cysts larger than 50 mm.
In this study, the laboratory findings and CE serological tests were evaluated (Table 2). Among the 114 patients assessed, leukocytosis was observed in 56 individuals (49%), while thrombocytosis was noted in 22 patients (19.3%). Neutrophilia was present in 36 patients (31.6%), whereas lymphocytosis and eosinophilia were found in 38 (33.3%) and 37 patients (32.5%), respectively. Evaluation of liver enzymes among 89 patients revealed elevated levels in some cases, with 13 patients (14.6%) exhibiting elevated AST (>40 U/L), 11 patients (12.3%) with elevated ALT (>40 U/L), and 2 patients (2.2%) showing elevated ALP (≥1200 U/L). Furthermore, ESR and CRP were tested in 77 patients, with a significant proportion showing abnormal results; 73 patients (94.8%) had elevated ESR levels, while 47 patients (61%) had elevated CRP levels.
Laboratory Findings of the Patients with Cystic Echinococcosis
NA, not applicable.
Regarding serological tests, 28 patients underwent testing, with 21 patients (75%) showing positive serology results. Among patients with lung involvement who underwent serology testing, 11 patients (64.7%) tested positive for IgG, 6 patients (35.3%) tested negative for IgG, 4 patients (23.5%) tested positive for IgM, and 13 patients (76.5%) tested negative for IgM. Additionally, among patients with liver involvement for whom IgG and IgM levels were measured, 14 patients (82.3%) tested positive for IgG, while 3 patients (17.7%) tested negative.
In this study, hospitalized patients diagnosed with CE underwent albendazole treatment (400 mg/day) involving both medication and surgical intervention. Specifically, all patients received medication, and a substantial majority, comprising 104 patients (91.2%), underwent surgical procedures.
After undergoing surgery, 3 of the 114 patients included in the study tragically passed away, representing a mortality rate of 2.6%. Conversely, 101 patients were discharged following surgery, while the remaining 10 patients received ongoing monitoring and drug treatment.
Discussion
The findings of this study provide valuable insights into the epidemiology, clinical characteristics, and diagnostic approaches of pediatric CE in Iran. The increasing prevalence of CE in recent years in Iran underscores the need for heightened awareness and effective control measures to control the disease burden (Hamzavi et al., 2011; Kamali et al., 2018; Mahmoudi et al., 2012; Mahmoudi et al., 2019). According to a meta-analysis conducted by Mahmoudi et al., the pooled prevalence of CE in Iran was estimated to be 5% (95% confidence interval: 3–6%) (Mahmoudi et al., 2019). The highest occurrence of CE in children aged 5 to 11 years aligns with observations in other regions such as central Turkey (Eyüboğlu et al., 2019) and India (Gupta et al., 2014). This age-group may be particularly susceptible due to increased exposure to environmental risk factors and activities involving contact with dogs or sheep, as evidenced by the majority of patients having a history of such contact.
In the present study, the majority of patients (70.2%) reported a previous history of contact with dogs or sheep, aligning with findings from previous reports in this referral center (Mahmoudi et al., 2012).
CE can manifest with a wide range of symptoms and complications depending on the site of cyst rupture and the involvement of various anatomical structures. When cysts rupture into different areas of the body, they can lead to diverse clinical presentations, ranging from abdominal symptoms such as pain, nausea, and vomiting to respiratory symptoms such as coughing, chest pain, and dyspnea. The study conducted in Turkey indicated that abdominal symptoms were most common, with a significant portion of patients being asymptomatic and incidentally detected (Sen et al., 2019). However, the present study found rarer symptoms such as seizures and headaches when cysts were located in the brain, as well as respiratory symptoms.
The diagnosis of CE can be made easily by the combination of clinical symptoms, serologic tests, and imaging modalities (Goussard et al., 2022). The analysis of the diagnostic landscape for CE across various anatomical sites reveals differing levels of effectiveness among diagnostic methods. Pathology consistently emerges as the most dependable approach for confirming CE. While imaging techniques such as CT scans and ultrasonography are widely employed and offer valuable insights, they exhibit slightly lower effectiveness compared with pathology. This highlights the significance of integrating both imaging and pathological assessments for achieving accurate diagnosis and ensuring optimal management of CE in various clinical scenarios.
The most frequently involved organs were the liver and lung, which was consistent with the previous reports (Goussard et al., 2022; Mahmoudi et al., 2019; Mohammadi et al., 2021; Paduraru et al., 2024).
A significant proportion of patients (68%) had large cysts, exceeding 50 mm, indicating potential disease advancement. However, these findings differ from other studies (Ahmed et al., 2022), where cyst sizes were smaller, suggesting variations in disease severity or patient populations. Studies from Central Ethiopia (Belachew et al., 2019) and Turkey (Bayrak and Altıntas, 2019) also reported varying cyst sizes, highlighting global heterogeneity in echinococcosis presentation. Larger cyst sizes observed in our study may necessitate more aggressive interventions, such as surgical removal. Further research is needed to understand the reasons behind these differences in cyst sizes across populations and regions.
Variations in laboratory findings across different geographic regions suggest differences in the clinical presentation and laboratory profile of patients with CE. A substantial proportion of patients, about 95% and 60%, respectively, demonstrated elevated levels of ESR and CRP. These findings align with a study conducted by Padayachy et al., which similarly reported increased ESR and CRP levels in cases of hydatid disease affecting the brain and spine (Padayachy and Ozek, 2023). Elevated levels of these inflammatory markers suggest ongoing inflammation and immune response, which are common features of CE. Monitoring liver enzymes, ESR, and CRP can provide valuable insights into disease activity and response to treatment, aiding in the management of CE.
In our study, most patients tested positive for IgM or IgG antibodies, with ∼65% and 83% positive for IgG antibodies in cases of pulmonary and liver involvement, respectively. Negative IgM results were observed in about 77% and 65% of these cases. These findings support the utility of serological testing, particularly for IgG antibodies, in identifying hydatid cysts, especially in pulmonary and liver cases. Monitoring antibody levels before and after cyst removal can offer insights into disease progression and treatment response (Qasim and Yousif, 2020).
In this study, hospitalized patients diagnosed with CE received a combination of medication and surgical interventions as part of their treatment regimen. Notably, over 90% of the patients underwent surgical procedures. The treatment approach aligns with recommendations proposed by Yorganci et al., based on the Gharbi classification system. They suggested that surgery should be considered as the primary treatment option for type III hydatid cysts, characterized by fluid collection with septa (also known as the honeycomb sign), as well as for type IV hydatid cysts, which present with heterogeneous echographic patterns and may have cysts opening into the bile ducts or peritoneal cavity. Conversely, they indicated that therapy may often not be necessary for type V hydatid cysts, which typically exhibit thick walls. This treatment strategy emphasizes the importance of individualized management approaches tailored to the specific characteristics and classification of hydatid cysts, with surgery reserved for cases where it is deemed most beneficial in addressing the particular features and complications associated with the cysts (Yorganci and Sayek, 2002).
The study encountered limitations primarily due to data availability within the hospital records. Notably, cases from 2012 were inaccessible for analysis, representing a significant gap in the dataset. Additionally, incomplete recording of patient information posed a significant challenge, particularly regarding serological tests, liver enzymes, and details on cyst size and number. Furthermore, the lack of data on disease recurrence rates in patients represents another notable limitation. Understanding recurrence patterns is crucial for informing treatment strategies and assessing long-term outcomes.
Conclusion
In conclusion, this study contributes to our understanding of pediatric CE in Iran, highlighting the increasing prevalence of the disease. Continued efforts to enhance surveillance, early diagnosis, and targeted interventions are essential for mitigating the burden of CE and improving outcomes for affected pediatric populations. Further research is needed to address knowledge gaps and inform evidence-based strategies for disease prevention and control.
Footnotes
Authors’ Contributions
S. Mahmoudi and S. Mamishi had the idea for and designed the study and had full access to all data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. S. Mahmoudi, M.R.A., M.D., and B.P. contributed to the case finding. M.D. collected all data regarding the patients. S. Mahmoudi analyzed the data. G.M.T. contributed to the writing of the first draft of the article and S. Mahmoudi revised it. All authors read and approved the final article.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure Statement
The authors declare that they have no competing interests. All authors confirm that their research is supported by an institution that is primarily involved in education or research.
Funding Information
The work of S. Mahmoudi received partial support from the European Commission––European Research Executive Agency under grant agreement No. 101130873.