
Abstract
Listeriosis is a rare, life-threatening bacterial infection. Prompt, appropriate antibiotic treatment is essential to save lives. We aimed to investigate antibiotic selection and listeriosis knowledge among health care providers. We first performed a retrospective study on patients with listeriosis who were treated in a hospital in China from January 2013 to March 2023. Patient characteristics and antibiotic selections were recorded. Antibiotics were classified as effective or ineffective based on the efficacy classifications listed in The Sanford Guide to Antimicrobial Therapy (50th edition). We then conducted a questionnaire survey of health care providers to investigate their listeriosis knowledge and practices between April 2023 to May 2023. Fifteen listeriosis patients were identified, with a case fatality rate of 26.7% (4/15). Empirical treatments assessed as effective antibiotics or ineffective antibiotics were given to 33.3% (5/15) and 66.7% (10/15) of the patients, respectively. After Listeria monocytogenes was identified, 40% (6/15) of the patients received an adjustment to their antibiotics, although 50% (3/6) patients still received ineffective antibiotics. The questionnaire survey of 77 participating health care providers showed that 32.9% (24/73) of the clinicians were unaware of the appropriate antibiotics for listeriosis. Most participants (83.1%, 64/77) would read the drug sensitivity report before selecting the antibiotics. The selection of effective antibiotics differed between the infectious diseases department and other departments (p < 0.001), but did not differ between junior title and other titles (p = 0.088). Most patients with listeriosis did not receive appropriate antibiotics, which might have accounted for the high fatality rate, and may have resulted from inadequate listeriosis knowledge. More education and correct reporting of drug sensitivity results are urgently needed.
Introduction
Listeria monocytogenes (LM), a rare Gram-positive facultative intracellular parasite, is the only pathogen that causes listeriosis in humans. Pregnant women, newborns, the elderly, and immunosuppressed individuals are highly susceptible to listeriosis (Charlier et al., 2017; Hernandez-Milian and Payeras-Cifre, 2014). Liver disease, kidney disease, and gastrointestinal bleeding are the main predisposing factors for LM infection (Lu et al., 2023). The main cause of listeriosis is through the consumption of LM-contaminated foods, such as ready-to-eat food, products stored for a long time, deli meats, and especially dairy products. Clinical presentations of listeriosis include self-limited febrile gastroenteritis, septicemia, meningitis, or meningoencephalitis, as well as pregnancy-related complications, including stillbirth, spontaneous abortion, or neonatal sepsis (Salama et al., 2018). The insidious onset, long incubation period, and atypical clinical symptoms of listeriosis can easily lead to missed diagnosis and serious outcomes (Schlech, 2019; Zahedi Bialvaei et al., 2018). Thus, prompt and appropriate antibiotic treatment is essential to treat listeriosis (Arslan et al., 2015; Pagliano et al., 2016).
Listeriosis is a sporadic infectious disease with a low incidence of 0.1–1.6 cases per 100,000 in the population (European Center for Disease Prevention and Control, 2017; Lomonaco et al., 2015), but can have outbreaks (Ottesen et al., 2016). In China, listeriosis was an unreported disease until 2013, when isolated cases were included in the national surveillance program (Li et al., 2018). Thus, many clinicians have had limited encounters with listeriosis and, therefore, lack experience in diagnosing listeriosis and knowledge about how to manage its treatment.
This study retrospectively evaluated the selection of antibiotic therapy for patients with listeriosis in a local tertiary teaching hospital in China over the past 10 years. We also assessed the knowledge, attitudes, and practices of clinicians and clinical pharmacists in regard to the risk factors, diagnosis, and antibiotic treatments for listeriosis. The purpose of our study was to identify knowledge gaps and educational opportunities that could ultimately be used to improve healthcare for patients with rare LM infection.
Materials and Methods
Study design and participant selection
The study included two phases. The first phase included a retrospective review of patients who were admitted to the First Affiliated Hospital of Bengbu Medical University at Bengbu, China, between January 2013 and May 2023. The hospital is a 3828-bed tertiary teaching facility. The second phase included a questionnaire survey to assess the listeriosis knowledge and practices among clinicians and clinical pharmacists between April 2023 to May 2023. The study protocol was approved by the hospital ethics committee (protocol code 2020KY072; date of approval August 3, 2020). In the first phase, written informed consent from the patients was waived due to the retrospective study design. In the second phase, written informed consent was obtained from the clinicians and clinical pharmacists who were invited to participate in the questionnaire survey. The entire study was carried out in accordance with relevant guidelines and regulations.
For the first phase of the study, patients who were admitted to the hospital and who had listeriosis confirmed by laboratory tests (LM isolated from blood, cerebrospinal fluid [CSF], or fetal membrane secretion) were included in the study. Patients with incomplete medical records were excluded. For the second phase of the study, clinicians and clinical pharmacists in infection-related departments, including the Departments of Infectious Diseases, Rheumatology and Immunology, Intensive Care Unit, Emergency Surgery, Pharmacy, Pediatrics, Pulmonary, Neurosurgery, Cardiovascular, and Ophthalmology, were included. All participants in the second phase utilized a hospital infection WeChat communication group (Tencent, China, a social media app similar to Instagram, USA).
Data collection for retrospective chart review
Patient information, including demographics, infection diagnosis, underlying diseases, bacterial culture results, empirical antibiotic therapy, pathogen antibiotic therapy, clinical outcomes, and admitting department, were extracted from the hospital medical charts. The potential effective and ineffective antibiotics selected against LM before and after diagnosis of listeriosis were calculated. Appropriate antibiotic selections against LM were based on The Sanford Guide to Antimicrobial Therapy (50th edition) (Gilbert et al., 2021a). The standard first-choice antibiotics included ampicillin with or without gentamicin, which has a synergistic effect against LM. The second choice was trimethoprim/sulfamethoxazole. Other effective antibiotics included erythromycin, penicillin G (high dose), anti-Pseudomonas aminoglycosides, and β-lactams, which have potential synergistic effects. Cephalosporins were not recommended due to their LM resistance. We calculated the percentage of patients who received the effective antibiotics (ampicillin, penicillin, trimethoprim/sulfamethoxazole, gentamicin, azithromycin, anti-pseudomonas aminoglycosides, and β-lactams) and the percentage of patients who received ineffective antibiotics (cephalosporins).
LM detection was performed in the microbiology room of the hospital laboratory department. The drug sensitivity test was conducted using the microbroth dilution method. Cation-adjusted Mueller–Hinton broth was used to supplement 5% split horse blood, under the conditions of inoculum by direct colony suspension and 0.5 McAllisteria suspension, which was followed by incubation at 35°C and room air for 20–24 h (Clinical and Laboratory Standards Institute, 2015).
Treatment outcomes were categorized into death, cure, improvement, or spontaneous delivery. Cure was defined as negative for pathogens upon re-examination and resolution of clinical symptoms. Clinical improvement was defined as negative for pathogens upon re-examination and amelioration of clinical symptoms. Treatment outcomes were defined and calculated by the authors who extracted the hospital records.
Data collection for the questionnaire survey
The questionnaire survey was created by an expert panel, including four senior infectious diseases doctors and four senior clinical pharmacists. The final questionnaire consisted of four parts, including basic information on participants, diagnoses of listeriosis, antimicrobial therapy, and high-risk factors of listeriosis, as shown in the Supplementary Data S1. It was an anonymous, self-administered web-based survey that required 10–15 min to complete. The survey was distributed to the eligible participants through a hospital infection WeChat communication group.
Statistical analysis
Data were analyzed in SPSS 24.0 (IBM, USA). Continuous data were first examined for normality using the Shapiro–Wilk test. Data that followed a normal distribution are presented as the mean ± standard deviation (
Results
Patient characteristics
A total of 15 patients, including 10 adults, 4 neonates (diagnosed at 8 h, 8 days, 13 days, and 15 days after birth, respectively), and one infant aged 1 year and 8 months old. The adult patients had an average age of 45.6 ± 18.9 years (ranging from 20 years to 72 years) and an average body weight of 60.6 ± 5.5 kg. Patient characteristics are presented in Table 1. Finally, four patients died of listeriosis (case fatality rate of 26.7%, 4/15).
Patient Characteristics in Our Hospital
Note: CSF, cerebrospinal fluid; LM, Listeria monocytogenes.
Antibiotic selections before and after listeriosis diagnosis
The numbers of respondents who chose each antibiotic treatment before and after diagnosis of listeriosis are shown in Figure 1. Before the diagnosis of listeriosis, effective antibiotics were used in 33.3% of patients (5/15, with piperacillin and sulbactam in two cases, amoxicillin and sulbactam in two cases, and azithromycin in one case), and ineffective antibiotics were used in 66.7% (10/15) of patients. After the diagnosis of listeriosis, the antibiotics were adjusted in 40% (6/15) of the patients. However, 50% (3/6) of the patients still received ineffective antibiotics.
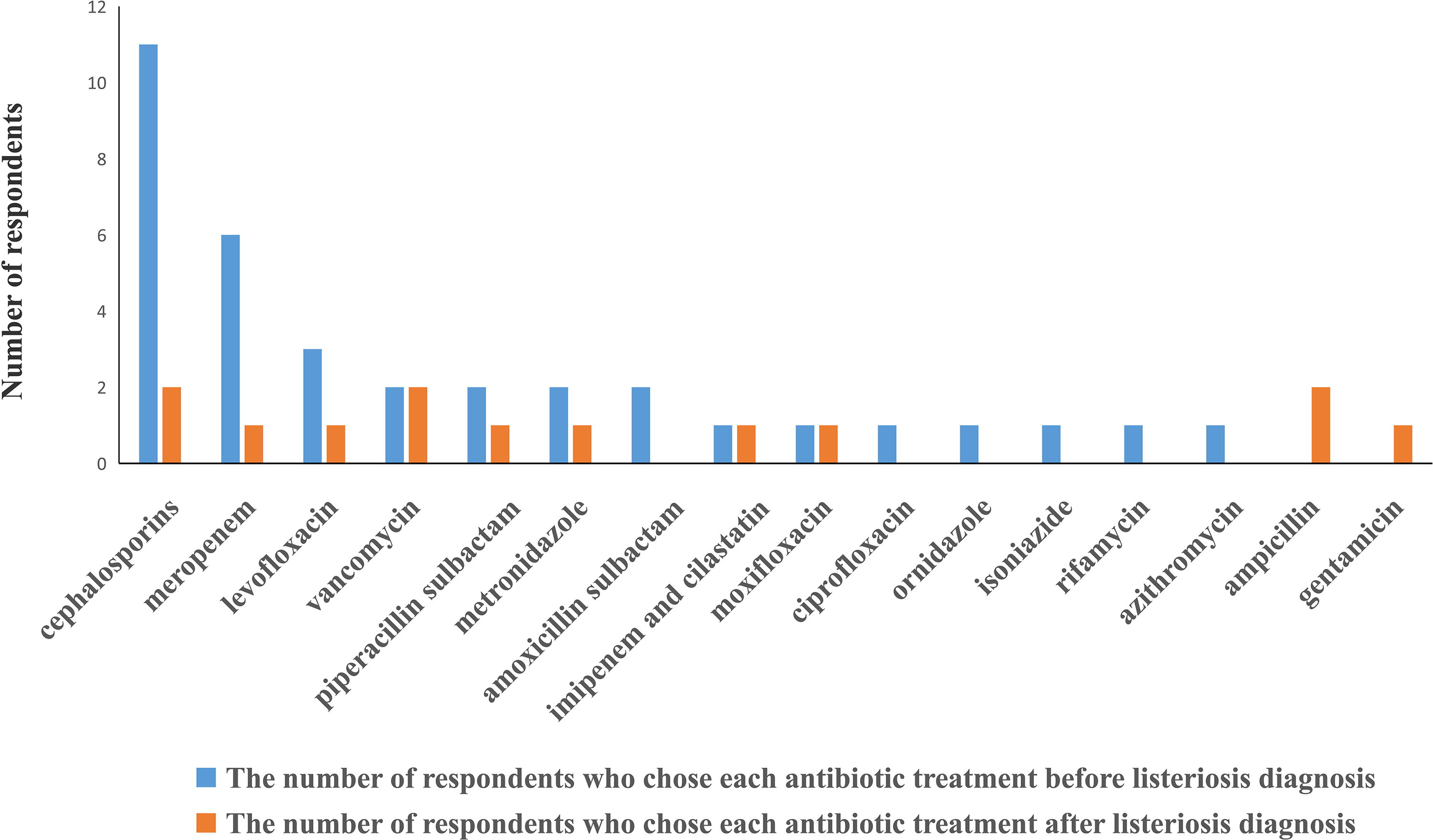
The numbers of respondents who chose each antibiotic treatment before (blue) and after (orange) diagnosis of listeriosis in the hospital.
The antibiotic sensitivity reports of LM in our hospital are shown in Table 2. According to Clinical and Laboratory Standards Institute (CLSI) recommendations, the appropriate antimicrobial agents for LM include penicillin, ampicillin, trimethoprim/sulfamethoxazole, erythromycin, and meropenem. The determination of the break point was based on the drug sensitivity test (mg/L). The minimum inhibitory concentrations (MIC) for penicillin ≤2, ampicillin ≤2, trimethoprim/sulfamethoxazole ≤0.5–9.5, and meropenem ≤0.25 were defined as Susceptible (S). For trimethoprim/sulfamethoxazole, the MIC of 1–19 to 2–38 was defined as Intermediate (I), and the MIC ≤4~76 was defined as Resistant (R) (Clinical and Laboratory Standards Institute, 2015). After the diagnosis of LM infection, only 13.3% (2/15) of the patients received ampicillin as the preferred antibiotics in our hospital. No penicillin or trimethoprim/sulfamethoxazole was selected. Cephalosporins with resistance to LM or drugs of uncertain efficacy were selected in the others. The clinical outcomes in patients with effective or ineffective antibiotics are shown in Table 3.
The Antibiotic Sensitivity Reports of Listeria Monocytogenes
I, intermediate; R, resistant; S, susceptible.
Clinical Outcomes in Patients with Effective or Ineffective Antibiotics
Questionnaire survey
There were 95 providers in the WeChat group, including 91 clinicians and 4 pharmacists. A total of 77 responses were received, with an overall response rate of 81.1%. The characteristics of participants are shown in Table 4. Approximately one-third of the participants were from the Department of Infectious Diseases (27, 35.1%). The majority of participants were clinicians (73, 94.8%).
Characteristics of Clinicians and Pharmacists Involved in the Questionnaire Survey (n = 77)
The questionnaire survey results are shown in Table 5. Most participants (42, 54.5%) who returned the survey had not treated a patient with LM infection. Most of these participants thought that blood culture was the diagnostic test (73, 94.8%). Most indicated that they knew the common site of infection to be the central nervous system. More than four-fifths of the participants (64, 83.1%) said that they would look at the drug sensitivity results to choose an appropriate antibiotic to treat LM infection. The antibiotics selected most frequently were penicillin (30, 39.0%) and ampicillin (28, 36.4%). Most participants could detect the risk factors for LM infection.
Questionnaire Survey Results
Published guidelines included The Sanford Guide to Antimicrobial Therapy (Gilbert et al, 2021b), National Guidelines for Antimicrobial Therapy (He et al, 2017), and Guiding Principles for Clinical Use of Antibiotic (version 2015) (The revised working group from clinical application of antibacterial drugs guiding principles, 2015).
There was a statistically significant difference in the selection of effective antibiotics (ampicillin, penicillin, and trimethoprim/sulfamethoxazole) between the Department of Infectious Diseases and other departments (excluding the Department of Pharmacy, with only four clinical pharmacists) (χ2 = 13.321, p < 0.001). There was no statistically significant difference in the selection of effective antibiotics (ampicillin, penicillin, and trimethoprim/sulfamethoxazole) between junior titles and other titles (χ2 = 6.546, p = 0.088) (Table 6).
Effective Antibiotic Selection Based on Department and Professional Title
Discussion
LM is an opportunistic intracellular pathogen that causes listeriosis. Despite the low incidence of listeriosis, its high mortality rate makes this bacterium one of the most dangerous foodborne pathogens (Grosboillot et al., 2022).
Invasive listeriosis carries a high mortality rate; therefore, timely and effective antibiotic therapy is essential to save lives. In the present study, 15 patients were confirmed to have LM infection by blood, CSF, or fetal membrane secretion cultures over a 10-year period (January 2013 to May 2023). The coverage rate of empirically selected LM-sensitive antibiotics was 33.3% (5/15). Cephalosporins were used for empirical anti-infective treatment in 73.3% (11/15) of the patients, despite not being recommended by The Sanford Guide. After listeriosis was confirmed, only 40% (6/15) of the patients received adjusted antibiotics. However, even after adjustments, only 50% (3/6) of the patients received the recommended effective antibiotics. It needs to be emphasized that only 13.3% (2/15) of the patients received ampicillin, which is considered as the first-line antibiotic by The Sanford Guide. One patient received a combination of vancomycin, ceftriaxone, and ampicillin due to listeriosis meningitis. The combination was inappropriate, and ampicillin alone was sufficient. No patients received trimethoprim/sulfamethoxazole. Four patients (26.7%, 4/15) received antibiotics with controversial clinical efficacy (vancomycin, imipenem, and meropenem), and two patients (13.3%, 2/15) still received cephalosporins. Drugs without antibacterial activity against LM (metronidazole, levofloxacin, and moxifloxacin) were administrated to 20% (3/15) of the patients. In a case of a mother who gave birth to a stillborn fetus by spontaneous abortion, LM was cultured in the fetal membrane secretions. The patient improved without effective antimicrobial treatment, which might have been related to the self-limitation of LM infection in normal immune patients. In our study, the mortality rate was 26.7% (4/15), which is similar to the mortality rate of 26.1% previously reported in 211 cases of listeriosis in China (Li et al., 2019).
To understand the rationale for antibiotic selection for patients with listeriosis in our hospital, we conducted a questionnaire survey among clinicians and clinical pharmacists in infection-related departments. There were 57.5% (42/73) of clinicians who did not encounter LM infection, while 100% (4/4) of anti-infective clinical pharmacists encountered LM infection. Nearly half of the clinicians (49.3%, 36/73) did not know the site of LM infection, while 100% (4/4) of anti-infective clinical pharmacists knew the site of infection. Most study participants (83.1%, 64/77) stated that they chose antibiotics based on the drug susceptibility report (Table 2). However, this was significantly different from what the CLSI recommends (Clinical and Laboratory Standards Institute, 2015). The drug sensitivity report may have misled clinicians in prescribing antibiotics. Therefore, it is suggested that the CLSI standard should be strictly followed to produce LM drug sensitivity, which cannot be replaced by a uniform drug sensitivity of Gram-positive coccus.
There were 23.4% (18/77) of clinicians and pharmacists who sought references from published guidelines. In addition, there were 32.9% (24/73), 19.2% (14/73), and 35.6% (26/73) of clinicians who knew that ampicillin, trimethoprim/sulfamethoxazole, and penicillin, respectively, were effective against LM, while 100% (4/4) of pharmacists selected the above drugs. Meropenem was selected by 17.8% (13/73) of clinicians and 75% (3/4) of pharmacists, despite the controversial efficacy and safety of meropenem in treating listeriosis (van de Beek et al., 2016). An in vitro study reported that meropenem had a markedly low MIC against LM, even lower than that of ampicillin (Carryn et al., 2003). However, limited clinical data showed that some pediatric patients with listeriosis could achieve satisfactory recoveries after meropenem treatment (Hassin et al., 2020; Hu et al., 2018; Kapuczinski et al., 2022; Seki et al., 2023; Zhang et al., 2021). One additional study showed that meropenem failed to treat a 25-month-old boy with listeriosis, although in vitro tests suggested that LM was highly susceptible to meropenem (Stepanović et al., 2004). Furthermore, two studies found that meropenem was associated with increased mortality in patients with listeriosis (Mitjà et al., 2009; Thønnings et al., 2016). Some clinicians (15.1%, 11/73) chose vancomycin that did not show clinical efficacy in a previous study (Lee et al., 2010). LM is resistant to cephalosporins that were selected by 17.8% (13/73) of the clinicians. Among these clinicians, 9.6% (7/73), 6.8% (5/73), and 1.4% (1/73) chose ceftriaxone, cefoperazone sulbactam, and ceftizoxime, respectively.
When comparing different departments, the Department of Infectious Diseases was more likely to choose effective antibiotics than other departments (excluding the Department of Pharmacy). There was no difference in choosing effective antibiotics among providers with different titles. Therefore, it is useful to consult with infectious diseases specialists for rare bacterial infections to improve patient outcomes (Chesdachai et al., 2020).
The strength of our study was that it reviewed listeriosis infections over the past 10 years, revealing a need to remind health care providers to pay attention to antimicrobial therapy for rare bacterial infections. We recommend that rare bacterial drug sensitivity reports should follow the CLSI standard. Physicians should strictly stick to the drug sensitivity list in the published guidelines for rare bacterial infections, such as The Sanford Guide to Antimicrobial Therapy, National Guidelines for Antimicrobial Therapy, or Guiding Principles for Clinical Use of Antibiotics (version 2015). Consultation with anti-infective pharmacists or infectious diseases specialists may be necessary if there is any question during the antibiotic selection. Our study also included several limitations, such as its single-center, observational, and retrospective design, as well as its relatively small sample size. Another limitation was that the second phase of the study used a questionnaire survey that was not validated.
Conclusions
The inappropriate selection of antibiotics reported in this study might have been due to inappropriate drug sensitivity reports as well as limited knowledge on LM among health care providers. The LM drug sensitivity report should follow the CLSI standard. Clinicians need to strengthen their knowledge of listeriosis. Anti-infective pharmacists and infectious diseases specialists who have better knowledge of listeriosis could also be consulted for active participation in selecting the appropriate antibiotics to ensure that patients with these rare bacterial infections receive timely and effective antibiotic treatments.
Ethics Approval and Consent to Participate
This work was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of The First Affiliated Hospital of Bengbu Medical University (protocol code 2020KY072 and date of approval: August 3, 2020). All methods were carried out in accordance with relevant guidelines and regulations. Written informed consent was obtained from all subjects involved in the study.
Footnotes
Acknowledgments
We thank Professor Yonghong Xiao from the State Key Laboratory for Diagnosis and Treatment of Infectious Diseases at The First Affiliated Hospital of Zhejiang University School of Medicine for providing research ideas and a paper review. We would also like to thank Medjaden Inc. for the scientific editing of this article.
Authors’ Contributions
All authors meet the ICMJE authorship criteria. Conceptualization, N.Z. and T.C.; methodology, N.Z.; software, T.C.; formal analysis, T.C.; investigation, N.Z.; resources, C.L., C.G., and Z.W.; data curation, N.Z.; writing—original draft preparation, N.Z.; writing—review and editing, Z.W., Z.L., Y.X., J.L., and T.C.; supervision, N.Z.; project administration, C.L. All authors have read and agreed to the published version of the article.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available due to limitations of ethical approval involving the patient data and anonymity but are available from the corresponding author on reasonable request.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was supported by the Natural Science Key Project of Bengbu Medical College (BYKY2019054ZD) the Domestic Visiting Training Program for Outstanding Young Backbone Teachers (gxgnfx2022035) and Project of China Hospital Reform and Development Research Institute, Nanjing University and Aid project of Jiangsu Ningai Medical Development & Medical Aid Foundation.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.