
Abstract
This study aimed to investigate the clinical and molecular characteristics of Giardia duodenalis (G. duodenalis) infection and identify potential risk factors in children and teenagers with malignancies in Shiraz, southwestern Iran. A total of 200 fresh fecal samples were collected from children and adolescents suffering from 32 different cancer types at Amir, Nemazee, and Saadi hospitals affiliated with Shiraz University of Medical Sciences between October 2021 and May 2022. Direct microscopy using saline and iodine wet mount was conducted, and all fecal samples were rechecked by SSU-PCR. Subsequently, a specific fragment of the tpi gene was amplified on all samples for prevalence, sequencing, and assemblage identification. Our study found a 4% (8/200) prevalence of G. duodenalis using microscopy and PCR. The molecular findings were consistent with the microscopic results. All eight positive samples with SSU-rRNA gene were also detected as positive with tpi gene and were correctly sequenced. Among the examined cancer patients, two assemblages were identified: A [sub-assemblage AI (2/8, 25%) and sub-assemblage AII (3/8, 37.5%)] and B [sub-assemblage BIV (3/8, 37.5%)]. Notably, patients were more vulnerable to G. duodenalis infection after receiving at least 8 treatment episodes (p < 0.05) and displaying gastrointestinal symptoms (p > 0.05). The demographic characteristics of cancer patients with G. duodenalis infection and the statistical conclusions were separately detailed. The small sample size and low prevalence rate in this study hindered precise epidemiological conclusions. Nonetheless, the results suggest that G. duodenalis infection among cancer patients in Shiraz city originates from humans, without any specific animal groups (C–H) involved.
Introduction
Intestinal parasitic infections (IPIs) are caused by a diverse group of parasitic agents and are more prevalent in developing countries due to poor hygienic infrastructure. Therefore, screening for IPIs is of utmost significance in the general population, particularly in individuals with immunodeficiency such as organ transplant recipients, patients undergoing hemodialysis, those with HIV/AIDS, and cancer patients (Esteghamati et al., 2019; Nooshadokht et al., 2017). Chemotherapy treatment for cancer patients occurs at varying intervals, making them highly susceptible to IPIs, which can result in severe diarrhea (Mahdavi et al., 2021a).
Diarrhea is a significant gastrointestinal complication in developing countries, with an annual mortality range of 1.9–2.2 million cases among children (Saaed and Ongerth, 2019). According to the World Health Organization (WHO), diarrheal diseases are among the top 10 causes of death worldwide (Wu et al., 2022). Despite viral and bacterial diarrhea receiving considerable attention, parasitic diarrhea has been overlooked (Mahdavi et al., 2021b). Giardiasis, caused by Giardia duodenalis (G. duodenalis, also known as G. lamblia or G. intestinalis), is a common parasitic infection in humans, affecting approximately 10% of the population (Xie et al., 2018). The infection can be asymptomatic or present as acute or chronic diarrhea, along with symptoms such as abdominal pain, nausea, flatulence, vomiting, and bloating (Agresti et al., 2021; Chen et al., 2019). Additionally, affected children have been observed to experience growth and developmental retardation (Mahdavi et al., 2021b). Several host (such as age and health status) and parasite factors (such as the virulence of the parasite and the number of cysts in hosts) may substantially impact the evolution and severity of G. duodenalis infection (Belkessa et al., 2021). Consumption of contaminated food/water sources and direct contact with infected animals are the primary transmission routes for G. duodenalis infection (Zhao et al., 2022).
Considerable heterogeneity exists within G. duodenalis isolates, which are sorted into eight assemblages, including A and B (humans and a variety of mammals) and C to H (host-specific for canids, domestic mammals, cats, rodents, and pinnipeds) (Chourabi et al., 2021; Costache et al., 2020). Assemblage A have three sub-assemblages (AI, AII, and AIII), while assemblage B possesses two sub-assemblages (BIII and BIV). Notably, here is no recognized nomenclature for assemblages C to H (Asghari et al., 2022a; Asghari et al., 2022b).
Giardiasis causes self-limiting diarrhea in people with a healthy immune system. However, immunocompromised patients may experience severe clinical outcomes and even death (Mahdavi et al., 2021a). Therefore, we conducted a study to determine the clinical and molecular characteristics of G. duodenalis infection and its potential risk factors in children and adolescents with malignancies in Shiraz, southwestern Iran.
Materials and Methods
Ethical statement
The present study was approved by the Ethics Committee of the Shiraz University of Medical Sciences, Fars province, Iran and was conducted from October 2021 to May 2022.
Fecal samples collection and microscopic examination
A total of 200 fecal samples (5–10 g each) were collected from children and adolescents under 18 years old with malignancies at Amir, Nemazee, and Saadi hospitals in association with Shiraz University of Medical Sciences. Direct microscopy using saline and iodine wet mount was applied, and fecal preparations were stained with Wheatley’s Trichrome stain. Three general groups of cancers were found among examined patients: hematological, non-hematological (cranial), and non-hematological (extra-cranial).
DNA extraction
Genomic DNA was extracted from collected fecal samples using the QIAamp Fast DNA Stool Mini Kit (Qiagen, Hilden, Germany) based on the manufacturer’s instructions. Next, the quantity and quality of the purified DNA samples were determined using a nano-spectrophotometer (NanoDrop ND-1000, Biocompare, San Francisco, USA). The final DNA was eluted in 50 µL of elution buffer and kept at −20°C for further use.
Polymerase chain reaction (PCR)
All fecal samples underwent further examination using molecular techniques for G. duodenalis. First, a nested PCR protocol was used to validate the presence of the parasite through amplification of a ∼130 bp fragment of the SSU-rRNA gene. The outer primer pair RH11 and RH4, and the inner primer set GiarF and GiarR were employed in both primary and secondary reactions (Gillhuber et al., 2013). The reaction mixture had 2 μL of template DNA for both primary and secondary PCR reactions. Cycling conditions were identical for the first and second steps of PCR. The primary denaturation was at 95°C for 3 min, followed by 35 cycles of amplification (denaturation at 95°C for 30 s, annealing at 55°C for 30 s), with a final extension of 7 min at 72°C.
Subsequently, a specific fragment of the tpi gene was amplified on all samples for prevalence, sequencing, and assemblage identification. Two primer pairs described by Sulaiman and colleagues (Sulaiman et al., 2003) were used for this purpose. The first PCR was done using AL3543 and AL3546 (0.5 μM each) primer pair, which amplify a 605 bp fragment, whereas the second PCR was performed using AL3544 and AL3545 (0.5 μM each) primer pair. All PCR reactions included 2 mM MgCl2, 200 μM dNTPs, 0.5 U of GoTaq DNA polymerase (Promega), and 5 μL of the extracted DNA (for primary PCR) or 1 μL of the primary PCR product (for secondary PCR). The extracted DNA from G. duodenalis assemblage A was used as a positive control. The following cycling conditions were applied to the thermal cycler device: initial denaturation (96°C for 4 min), followed by 35 cycles of denaturation (96°C for 30 s), annealing (55°C [primary PCR] or 59°C [secondary PCR] for 30 s) and extension (72°C for 45 s), as well as an excessive step of extension at 72°C for 4 min. Finally, the secondary PCR products were visualized by electrophoresis on 1.5% agarose gel stained with Safe Stain (SinaClon, Tehran, Iran).
DNA sequencing and phylogenetic analysis
Purified PCR products of the G. duodenalis tpi gene were sequenced bi-directionally using MACROGEN, (Korea), and the chromatograms were analyzed and edited and the obtained sequences were aligned using MEGA Version X. The maximum likelihood algorithm was used for the phylogenetic analysis of the isolates from current study and reference ones. The phylogenetic tree was drawn using a neighbor-joining parameter model with the highest likelihood algorithm value. The reliability of clusters was evaluated using a bootstrap of 1000 iterations. Giardia muris (AF069565) was placed as an outgroup in the phylogenetic tree.
Statistical analysis
Collected data were analyzed by SPSS software (version 20, IBM Inc., USA). To determine the correlation between G. duodenalis infection and subject variables such as age, sex, residence, symptomatology, number of chemotherapy cycles, and type of cancers, the Chi-square test was used. p < 0.05 was considered statistically significant.
Results
Parasitological and molecular examinations
Out of 200 fecal samples examined using both parasitological and molecular methods, 4% (8/200) tested positive for G. duodenalis infection. The molecular findings were consistent with the microscopic results.
Phylogenetic analysis and genotype/assemblage identification of G. duodenalis
All eight positive samples identified by microscopy and SSU-rRNA gene were also confirmed positive for the tpi gene and accurately sequenced. The sequence identity among all eight isolates in the current study in Shiraz and the reference sequences in GenBank was 98–100%. Two assemblages were molecularly characterized: A [sub-assemblage AI (2/8, 25%) and sub-assemblage AII (3/8, 37.5%)] and B [sub-assemblage BIV (3/8, 37.5%)] (Fig. 1).
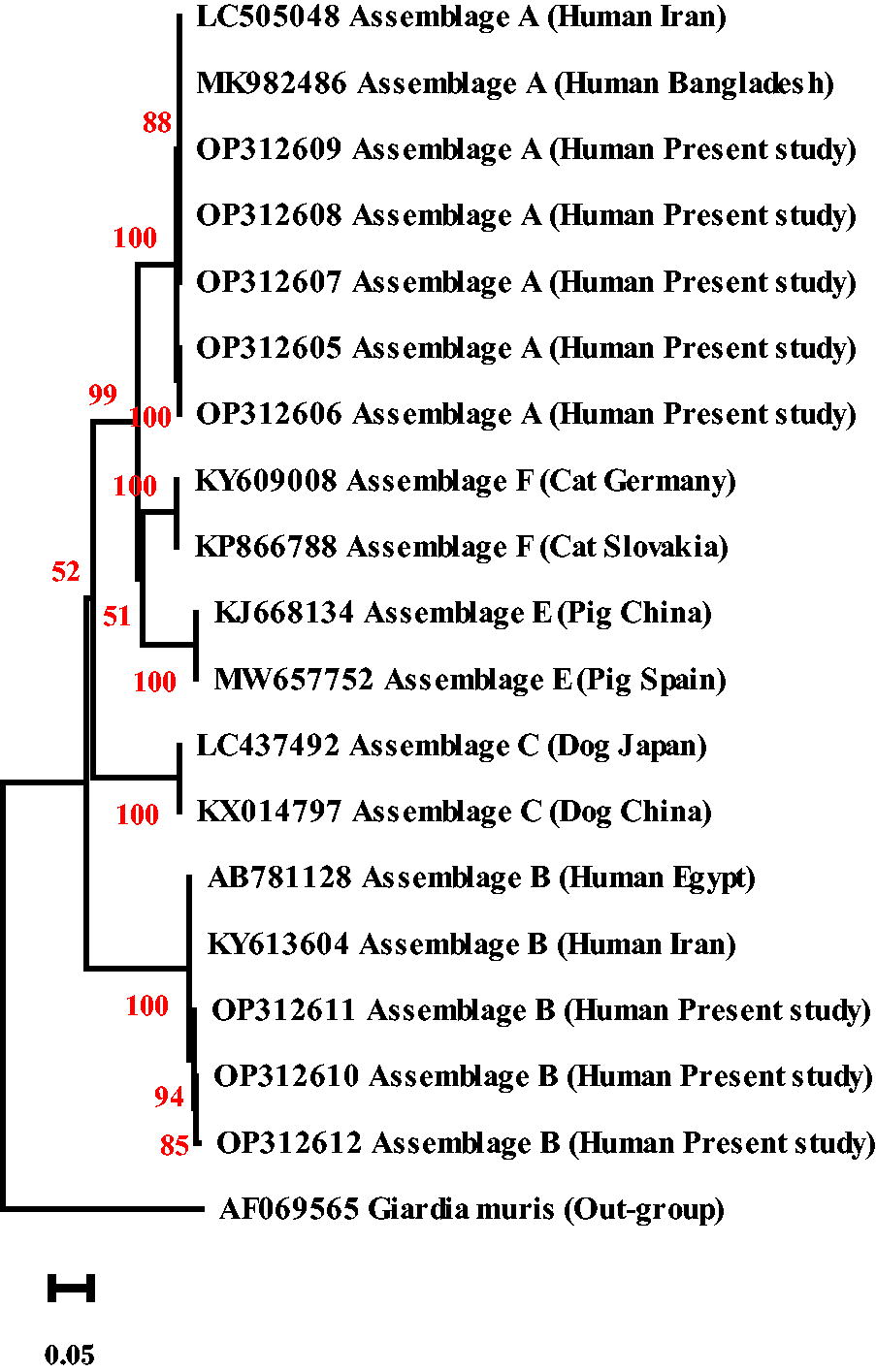
The phylogenetic tree of G. duodenalis sequences, constructed using the neighbor-joining method, indicates that the G. duodenalis isolates from cancer patients in this study belong to assemblages A and B. The percentage of replicate trees that clustered together in the bootstrap test (1000 replicates) is displayed next to the branches.
Distribution of Giardia assemblages/Sub-assemblages between various cancer types
The prevalence of G. duodenalis infection across various cancer types and the distribution of its corresponding assemblages/sub-assemblages are presented in Table 1. The highest and lowest frequencies of the G. duodenalis infection were observed in non-hematological [extra-cranial (5.5%)] and hematological (3.1%) cancer patients, respectively.
Distribution of G. duodenalis Assemblages/Sub-Assemblages between Various Cancer Types
Demographic characteristics of cancer patients for Giardia infection
Table 2 presents the demographic characteristics of cancer patients with G. duodenalis infection. In brief, there were no statistically significant differences reported between the variables examined and the infection rate of G. duodenalis in children and adolescents with cancer (p > 0.05).
Demographic Characteristics of Cancer Patients for G. duodenalis Infection
Association between chemotherapy cycles and symptomatology with prevalence of giardiasis
On the association between treatment of cancer patients and the prevalence of G. duodenalis infection, it was shown that among 8 and 192 PCR positive and negative patients, 7 (87.5%) and 148 (74%) cases had received chemotherapeutics, respectively. The frequency of therapies was directly associated with the G. duodenalis infection, so those patients receiving at least eight treatment episodes were more likely to be PCR-positive, as compared with those receiving none (χ2 = 6.7, p < 0.05) and 1–7 cycles (χ2 = 3.67, p < 0.05) (Table 3). Regarding symptoms, no substantial difference was determined among Giardia-infected and non-infected cancer patients (Table 4).
Chemotherapy (CT) and Giardiasis
A substantial difference was detected between groups A and C (χ2 = 6.7, p < 0.05); B and C (χ2 = 3.67, p < 0.05), but no notable difference was detected between groups A and B (χ2 = 1.57, p > 0.05).
Symptomatology and Giardiasis
GenBank accession numbers and associated assemblages/Sub-assemblages
The isolated partial tpi gene sequences from G. duodenalis patients suffering from cancer in Shiraz, southwestern Iran, are demonstrated in Fig. 1, under isolate/accession numbers of A11 (OP312605) and A12 (OP312606) [assemblage A (sub-assemblage AI)], A13-A15 (OP312607-OP312609) [assemblage A (sub-assemblage AII)], and B11-B13 (OP312610-OP312612) [assemblage B (sub-assemblage BIII)].
Discussion
Insufficient sanitation facilities in developing nations, such as limited access to clean drinking water and unreliable diagnostics, contribute to the underestimation and chronic nature of parasitic infections, significantly impacting the global morbidity and mortality (Asghari et al., 2021, 2020). These infections pose significant risks to immunocompromised individuals undergoing chemotherapy, potentially resulting in superinfection and hyperinfection syndromes caused by parasites and other pathogens. Notably, G. duodenalis infection is a common cause of diarrheal illness, particularly affecting children and the elderly (Azcona-Gutiérrez et al., 2017; Mahdavi et al., 2021b). This study aimed to explore the prevalence, distribution of different assemblages/sub-assemblages, and potential risk factors associated with G. duodenalis infection among children and adolescents with cancer in Shiraz, southwestern Iran.
Our findings indicate that 4% (8 out of 200) of the cancer patients examined were infected with G. duodenalis. Gender-based analysis revealed that the infection was higher among men (4.1%) than women (3.3%) (p > 0.05). The association of residence, cancer type, and age groups with G. duodenalis prevalence showed no significant differences in any of the variables studied (p > 0.05).
Our results align with a recent meta-analysis indicating a 6.9% (95% CI 0.5–9.3%) prevalence of G. duodenalis infection in cancer patients (Mahdavi et al., 2021a). A relatively similar global prevalence rate of 5% (95% CI: 4.2%–6%) was reported among HIV/AIDS patients (Mahdavi et al., 2021b). Such information may indicate that G. duodenalis infection is somehow more prevalent in cancer patients than in HIV/AIDS individuals; however, proper interpretation of this issue requires a similar number of studies and sample sizes, equivalent diagnostic methods, and examined population.
Overall, fresh smears have low sensitivity for detecting G. duodenalis in stool samples, even by experts. Currently, more sensitive diagnostic techniques, such as the indirect fluorescent antibody assay, are commonly utilized (Uehlinger et al., 2017). Additionally, most epidemiological studies accurately identify G. duodenalis infecting assemblages/sub-assemblages in different hosts using multilocus genotyping based on various genes. In the present study, all samples were initially assessed using the SSU rRNA gene, followed by confirmation with the tpi gene before sequencing. The tpi gene analysis corroborated the SSU rRNA findings, accurately identifying all infected cases without missing any positive samples. In some cases, using a single gene can result in discrepancies in the reported prevalence and classification of G. duodenalis sub-assemblages, as different genes such as tpi, gdh, and bg may detect/report various sub-assemblages (Rafiei et al., 2020; Wang et al., 2014; Wegayehu et al., 2016).
In the current study, the association between different clinical symptoms such as diarrhea, constipation, anorexia, flatulence, abdominal pain, malabsorption, and melena and the prevalence of G. duodenalis infection was evaluated; our results suggested that those subjects with gastrointestinal symptoms were more exposed to G. duodenalis than patients without symptoms (p > 0.05), being consistent with a previous study (Al-Mohammed, 2011). Frequency of therapies was, also, recognized as a likely contributing factor for G. duodenalis infection; so that, those individuals who had received eight or more treatment episodes were more infected with G. duodenalis infection than those receiving fewer or none. Although no similar study was conducted on G. duodenalis, there are previous studies on other protozoal agents, showing a direct association between treatment episodes and an increase in parasitic infections, which is consistent with our results (Yersal et al., 2016).
Among cancer patients examined in Shiraz, zoonotic assemblages A (sub-assemblages AI and AII) and B (sub-assemblage BIV) were found; such assemblages were previously isolated from different hosts such as mammals (including humans, primates, and rodents), ruminants, and birds. (Elhadad et al., 2021; Faridi et al., 2020; Heyworth, 2016; Levecke et al., 2009; Reboredo-Fernandez et al., 2015). Characterization of the zoonotic assemblages from cancer patients in the present study does not necessarily signify transmission from animal sources to individuals; however, it can be suggested that such patients should avoid close animal contact. Previously, no similar molecular study was done on G. duodenalis in cancer patients in the country, and studies on healthy people have revealed the predominance of A and B sub-assemblages (AI, AII, BIII, and BIV) (Hooshyar et al., 2017; Rafiei et al., 2013; Rayani et al., 2014), which is in line with the results of the present study.
The primary limitation of the present study was the absence of a control group alongside the cancer patients, making it challenging to accurately analyze the epidemiological results and even the pathogenicity of G. duodenalis. Furthermore, it remains unclear whether the cancer patients were previously infected with G. duodenalis assemblages in their residence or were infected during inappropriate and/or prolonged hospitalization in hospitals through human-to-human transmission. Cross-sectional studies cannot address such ambiguities, so further longitudinal studies are required to elucidate similar questions. The use of a single tpi gene locus for genotyping and sequencing is another limitation of the present study. Despite valuable efforts in the study for parasitological and molecular identification of G. duodenalis in cancer patients in southwestern Iran, the true epidemiology of the infection and the involved risk factors are still neglected and demand extensive studies.
Conclusion
The primary finding of this study was the low incidence (4%) of G. duodenalis infection in cancer patients in Shiraz, southwestern Iran. However, this rate of prevalence is not suitable for epidemiological comments/conclusions. Patients were more vulnerable to G. duodenalis infection after receiving at least eight treatment episodes (p < 0.05) and displaying gastrointestinal symptoms (p > 0.05). No significant association was found between reported variables (age, sex, residence, and type of cancer) and G. duodenalis prevalence. Three sub-assemblages AI, AII, and BIV were isolated from Shiraz cancer patients, indicating that giardiasis transmission among cancer patients in Shiraz is primarily anthroponotic, necessitating robust healthcare measures. Overall, IPIs like G. duodenalis should be screened before chemotherapeutic approaches in immunocompromised patients. Further molecular-based analyses are required to confirm and expand on these findings.
Footnotes
Acknowledgment
The authors thank the Vice Chancellor for Research of Shiraz University of Medical Sciences for the financial support of this study.
Consent to Participate
Informed consent was obtained from all individual participants included in the study (parents of patients).
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available in the online version.
Sanctioned Countries Policy
All authors are primarily involved in education or medical research and are not directly supported by the government.
Disclosure Statement
The authors declare that they have no conflict of interest.
Authors’ Contributions
F.M., A.A., and H.N. conceived and designed the study. M.H.M., M.R.M., A.A., L.S., F.M., and S.S. had a role in collecting samples and statistical analysis. A.A., K.K., and F.M. performed the molecular analysis. F.M., M.R.M., and A.A. wrote the article. H.N. and M.H.M. critically revised the article. All the authors have read and approved the final article.
Funding Information
No funding was received for this article.