
Abstract
This study examined data from the Centers for Disease Control and Prevention’s National Outbreak Reporting System between 2001 and 2021 for confirmed outbreaks of foodborne illness due to Ciguatoxin in the United States. Previous research into Ciguatoxin illness in the United States has focused on specific states or territories—namely Hawaii, Florida, Puerto Rico, and the Virgin Islands—meaning the national distribution of outbreaks remains unclear. In addition, while specific categories of seafood (e.g., reef fish) are known to carry elevated risk of illness due to Ciguatoxin poisoning, it remains unclear the extent to which specific seafood items are associated with the odds of being hospitalized in an outbreak. This study calculated descriptive statistics for the distribution of outbreaks by state, season, site of exposure, and implicated seafood item. Then, binomial regression was used to assess the relationship between the implicated seafood item in an outbreak and hospitalization. Results provided evidence that knowing the implicated seafood item in an outbreak is associated with the odds of hospitalization (χ2 5 = 33.023, p < 0.0001). Even when a seafood item was found to be associated with elevated odds of hospitalization, not all cases involved hospitalization. This finding aligns with Ciguatoxin poisoning case reports, noting that key epidemiological factors include not just the seafood item consumed but also the quantity and the part consumed (e.g., the head). In conclusion, public health officials should consider Ciguatoxin poisoning outbreaks as multidimensional and utilize information about the seafood consumed as well as the quantity and parts of the seafood consumed.
Introduction
According to the Centers for Disease Control and Prevention (CDC), foodborne pathogens cause 48 million illnesses, 128,000 hospitalizations, and 3000 deaths per year in the United States (CDC, 2018). Between 10% and 20% of all foodborne illnesses in the United States are attributed to seafood, which includes finfish, crustaceans, mollusks, marine mammals, and fish eggs (Grattan et al., 2021). Seafood poisoning is a subset of seafood-associated illnesses that results from acute consumption of naturally occurring biotoxins that affect the gastrointestinal, cardiovascular, and nervous systems, with clinical manifestations that may include diarrhea, vomiting, impaired coordination, respiratory distress, and death (Grattan et al., 2013; Visciano et al., 2016; Fleming et al., 2018; Soliño and Costa, 2020). Most of these toxins have no antidote, are not organoleptically detectible, and are not deactivated by cooking (Grattan et al., 2013).
One such toxin, Ciguatoxin, is produced by phytoplankton that accumulate in larger marine organisms via the food chain and affects between 10,000 and 50,000 people globally each year (Lewis and Vetter, 2016; Fleming et al., 2018; Navarro Quiroz et al., 2020; Chinain et al., 2021). However, given underreporting and misdiagnosis, the actual incidence may be 10 times as high (Paul et al., 2011). The diagnosis of Ciguatoxin poisoning is made clinically, often based on patient reports of neurological symptoms (e.g., cold allodynia, paresthesia) and having recently eaten fish (Bailey and Withers, 2014; Chinain et al., 2021).
The epidemiology of Ciguatoxin poisoning in the United States has previously been studied. Azziz-Baumgartner et al. (2012) investigated Ciguatoxin poisoning in Puerto Rico in 2005–2006 and found a strong association with Barracuda consumption. Radke et al. (2013) analyzed Ciguatoxin poisoning in the U.S. Virgin Islands from 1980 to 2010 and found that annual incidence had either remained stable or declined. Radke et al. (2015) compared formal reports of Ciguatoxin poisoning in Florida from 2001 to 2011 with self-reports from recreational fishers and concluded that the actual incidence is higher than what the public health system captures. Klekamp et al. (2015) reviewed syndromic surveillance of Ciguatoxin poisoning in Florida in 2014 and concluded that some cases are missed by the health care system, in part due to a lack of provider education. Lastly, Nalley (2024) examined Ciguatoxin poisoning in Hawaii in 2022 and found that certain regions have elevated risk, while only 22% of fishers and fish consumers reported their experiences with Ciguatoxin poisoning to the health care system.
This research has provided insight into the epidemiology of seafood poisoning, namely its underreporting. Yet it remains unclear what the national distribution of Ciguatoxin poisoning outbreaks looks like, given that most existing research has focused on specific states or territories. Although Ciguatoxin cases may primarily affect tropical regions, there is evidence that their geographic distribution has been expanding globally (Soliño and Costa, 2020; Chinain et al., 2021). In addition, despite its low incidence, Ciguatoxin poisoning ranks between the fifth and eighth most costly foodborne illnesses in the United States (Ralston et al., 2011; Minor et al., 2015). Lastly, while patient reports of fish consumption are useful as an indicator for Ciguatoxin illness, it remains unclear whether there is an association between specific seafood items and the odds of hospitalization. As a result, the first aim of this study was to conduct a secondary analysis of data from the CDC’s National Outbreak Reporting System (NORS) to describe the epidemiology of Ciguatoxin poisoning outbreaks in the United States between 2001 and 2021. The second aim was to test the association of seafood items with hospitalization.
Materials and Methods
Given that this study involved secondary analysis, an Institutional Review Board (IRB) exemption request was submitted to and approved by the Thomas Jefferson University IRB. In September 2023, a data request was submitted to the CDC NORS dashboard for all foodborne outbreaks of Ciguatoxin poisoning reported to NORS between 2001 and 2021. The NORS includes all enteric disease outbreaks reported to the CDC by local, state, and territorial health departments in the United States when there are two or more cases of similar illnesses that have a common exposure (CDC, 2023a). The data request was granted in September 2023 (CDC, 2023b).
Data cleaning
As described by Tao et al. (2023) in their work with NORS data, it is often necessary to transform raw surveillance data in order to analyze it. Not all items in the original NORS data file were used in this analysis; some were excluded, while others were cleaned or re-coded as follows. First, both single and multistate outbreaks were included but were categorized by the exposure state/territory. Second, only cases with a laboratory confirmed etiology of Ciguatoxin and data for hospitalizations were included. Third, missing observations for the site of exposure and the implicated food item were recoded as “Unknown.” Fourth, the variable corresponding to the month of the outbreak was recoded into “Season,” taking the value of either “Winter” (October 1 through March 31) or “Summer” (April 1 through September 30). Lastly, the variable for the name of the seafood item implicated in each outbreak was cleaned for consistency (e.g., an item originally listed as “fish, grouper” was recorded as “Grouper”; an item originally listed as “Grouper, Black” was recorded as “Black Grouper”, etc.). Because the dataset included only the common name of the seafood involved, with no definitive species identification, only the common names were used for analysis.
Data analysis
Descriptive statistical analysis was conducted using means, standard deviations, frequencies, and population-standardized rates. Inferential statistical analysis was conducted using a binomial regression model for the effect of the type of seafood consumed on the odds of being hospitalized, rather than ill, in an outbreak. The inferential analysis was restricted to known seafood items that were reported to NORS at least 10 times during the study period. A Bonferroni-corrected 0.05 alpha level was used to assess pairwise comparisons. All data analyses were performed using R (R Core Team, 2023).
Results
Epidemiology of Ciguatoxin poisoning
Between 2001 and 2021, there were 972 illnesses, 130 hospitalizations, and 0 deaths reported due to Ciguatoxin poisoning. Overall, there were 293 confirmed outbreaks, with 269 of these outbreaks having data on whether or not there was a hospitalization. For any given outbreak, the number of illnesses ranged from 2 to 29, with a median of 3. In addition, for any given outbreak, the number of hospitalizations ranged from 0 to 23, with it being most common for no hospitalizations to occur (76.9% of all outbreaks); when hospitalizations did occur, the median number was 1.5. There were outbreaks reported every year, with the overall annual rate trending downward between 2001 and 2010, rising between 2011 and 2019, and falling since then (Fig. 1). On average, there were 4.13 (standard deviation [SD] ± 2.04) outbreaks per year per 100,000,000 population. The rate of outbreaks was lowest in 2010 (1.61) and highest in 2019 (9.44). On average there were 14.96 (SD ± 6.47) illnesses and 2.01 (SD ± 1.68) hospitalizations per year per 100,000,000 population. The rate of illnesses was lowest in 2012 (5.41) and highest in 2019 (28.02), while the rate of hospitalizations was lowest in 2002 (0) and highest in 2008 (7.56) (Fig. 1).
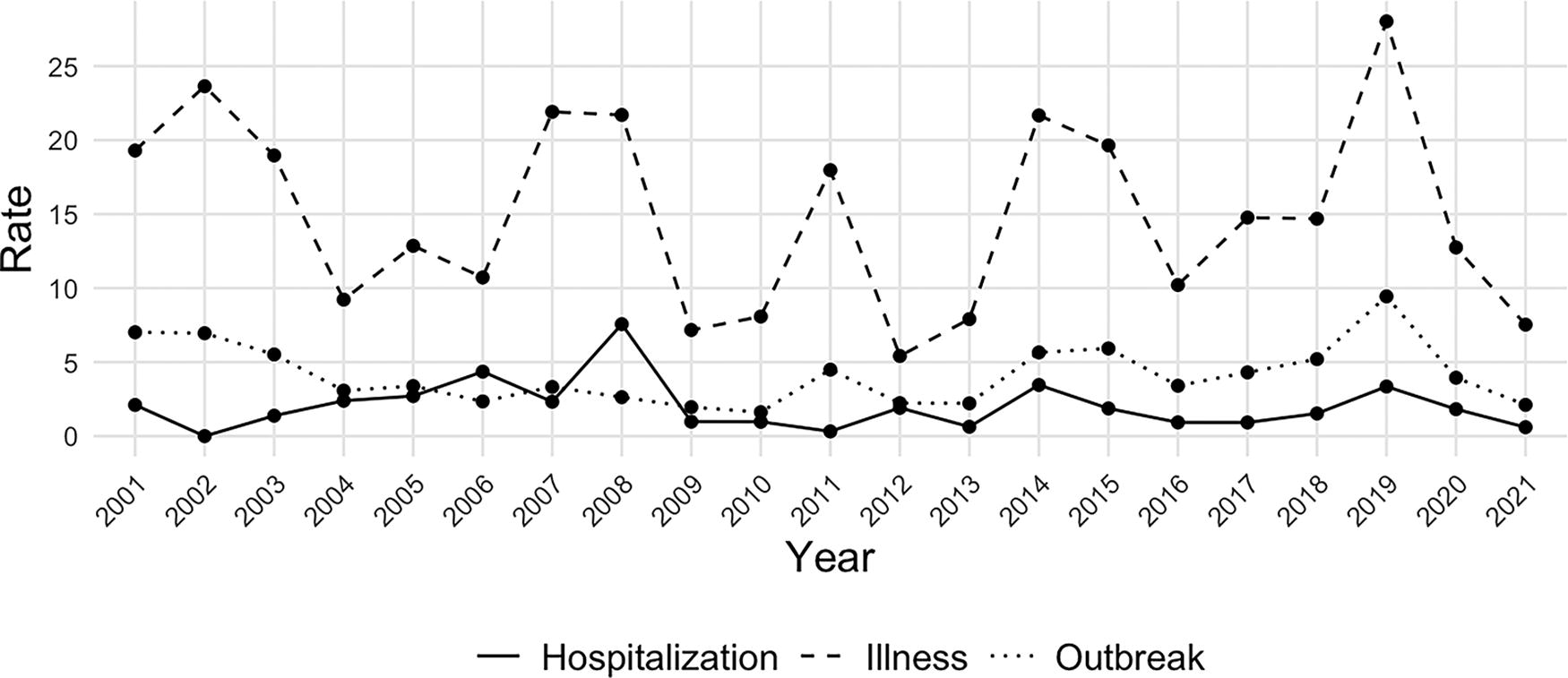
Rate of Ciguatoxin poisoning outbreaks, illnesses, and hospitalizations per 100,000,000 population. This figure includes data for outbreaks reported to the Centers for Disease Control and Prevention between 2001 and 2021.
Between 2001 and 2021, most Ciguatoxin poisoning outbreaks (71.37%), illnesses (69.13%), and hospitalizations (78.46%) were reported in the summer. Meanwhile, outbreaks were reported in 21 unique states and territories, with 82.16% of outbreaks, 76.34% of illnesses, and 78.46% of hospitalizations reported in the same three locations: Florida, Hawaii, and Puerto Rico (Table 1). Most outbreaks (79.55%) had a site of exposure listed as “private home/residence,” compared with 10.41% for “restaurant or banquet” (Table 2). Similarly, 74.9% of illnesses and 73.08% of hospitalizations had a site of exposure listed as “private home/residence,” while 12.76% of illnesses and 5.38% of hospitalizations had a site of exposure listed as “restaurant or banquet” (Table 2).
Ciguatoxin Poisoning Outbreaks, Illnesses, and Hospitalizations by State Between 2001 and 2021
Ciguatoxin Poisoning Outbreaks, Illnesses, and Hospitalizations by Site of Exposure Between 2001 and 2021
Between 2001 and 2021, there were 39 types of seafood implicated in Ciguatoxin poisoning outbreaks reported to NORS (Table 3). The 10 most common seafood items implicated in illnesses were Barracuda (26.85% of illnesses), Amberjack (13.99%), Grouper (11.21%), Unknown (9.47%), Roi (5.66%), Ulua (4.53%), Kole (3.19%), Seabass (2.37%), King Mackerel (2.06%), and Papio (1.95%). Meanwhile, 19 types of seafood were implicated in Ciguatoxin poisoning outbreaks that involved hospitalization (Table 3). The 10 most common seafood items implicated in hospitalizations were Barracuda (53.08% of hospitalizations), Roi (8.46%), Grouper (7.69%), Amberjack (6.15%), Mutton Snapper (3.08%), Unknown (3.08%), Black Grouper (2.31%), Jack (2.31%), Almaco Jack (1.54%), and Kole (1.54%).
Ciguatoxin Poisoning Outbreaks, Illnesses, and Hospitalizations by Implicated Seafood Item Between 2001 and 2021
Food items associated with hospitalization
There were 6 seafood items reported to NORS at least 10 times in relation to a Ciguatoxin poisoning outbreak during the study period: Amberjack, Barracuda, Grouper, Kole, Roi, and Ulua. Each seafood item was implicated in at least one hospitalization. Results of the binomial regression model provided evidence that knowing the type of seafood item implicated in an outbreak was associated with the odds of being hospitalized in that outbreak (χ2 5 = 33.023, p < 0.0001). Pairwise comparisons provided evidence that only consumption of Barracuda was associated with elevated odds of being hospitalized, specifically in comparison to consumption of Amberjack (p = 0.002) and Grouper (p = 0.045).
Discussion
Between 2001 and 2021, Ciguatoxin poisoning outbreaks in the United States were both rare and small, with an average of 4.13 outbreaks per year per 100,000,000 population and a median of 3 people ill and 1.5 people hospitalized per outbreak. There were no deaths from Ciguatoxin poisoning reported despite the toxin involved being capable of causing death. Overall, the rate of outbreaks in the United States appears to be trending downward in recent years. However, it remains unclear how best to interpret this finding given the conclusions of Radke et al. (2015), Klekamp et al. (2015), and Nalley (2024) regarding underreporting of Ciguatoxin poisoning. While the declining rate may be due to decreasing incidence, it might also reflect decreased reporting.
Ciguatoxin poisoning outbreaks, illnesses, and hospitalizations were more common in summer, suggesting a seasonal pattern. While outbreaks occurred across many states and territories, they were also concentrated in Florida, Hawaii, and Puerto Rico. In addition, most outbreaks, illnesses, and hospitalizations had a site of exposure listed as “private home/residence,” suggesting that Ciguatoxin poisoning and associated hospitalizations are generally not related to dining out. This finding aligns with existing research describing Ciguatoxin poisoning as an etiology of concern for recreational and subsistence fishers (Paul et al., 2011; Radke et al., 2015; Morin et al., 2016; Soliño and Costa, 2020).
While all outbreaks inherently involved illnesses, hospitalization was a variable feature of them. Similarly, not all seafood types were implicated in hospitalizations. Between 2001 and 2021, there were 39 types of seafood implicated in Ciguatoxin poisoning outbreaks and 19 implicated in outbreaks that involved hospitalization. This finding suggests that it is not seafood per se that is a risk factor for hospitalization but specific types of seafood. Consistent with the findings of Azziz-Baumgartner et al. (2012), Barracuda was the most commonly implicated seafood item during the study period: it was implicated in 26.85% of illnesses and 53.08% of all hospitalizations. Furthermore, while all the seafood items included in the regression analysis had at least one hospitalization, only consumption of Barracuda was strongly associated with the odds of being hospitalized. Nonetheless, the ratio of Barracuda-associated illnesses to hospitalizations was 3.78:1, suggesting that while consumption of Barracuda may increase the odds of hospitalization from Ciguatoxin poisoning, it does not universally result in hospitalization.
These results suggest that the risk of hospitalization from Ciguatoxin poisoning depends on both the seafood consumed and additional factors, such as the quantity or part consumed. A similar conclusion has been described in existing case reports of Ciguatoxin poisoning. For example, there is evidence of a dose-response relationship between the clinical severity of Ciguatoxin poisoning and both the quantity of fish eaten and the part of the fish eaten (Muecke et al., 2015; Edwards et al., 2019; Johnson-Arbor, 2023). To that end, recommendations for Ciguatoxin poisoning prevention include avoiding the species most at risk for it, as well as restricting the serving sizes of these fish and avoiding consumption of the head, liver, intestines, and viscera (Lewis and Vetter, 2016; Chan, 2016; Morris and Vugia, 2021). The findings from this study provide additional evidence that while certain kinds of seafood (i.e., Barracuda) carry an elevated risk of hospitalization, the risk of hospitalization in any given outbreak may also depend on the particular parts and quantities of seafood eaten.
Taken together, these findings have important implications in the United States, where per capita seafood consumption has nearly doubled since 1968 (Nguyen et al., 2023; Sun et al., 2023). Beyond North America, global seafood consumption is projected to continue increasing, with this consumption appearing to grow at a faster rate than meat consumption (Boyd et al., 2022; FAO, 2020). As Sobel and Painter (2005) have described, increased consumption of seafood carries the risk of increased exposure to marine biotoxins, and while there are many known marine biotoxins, others are newly emerging and climate change is expected to increase their burden (Mora et al., 2022; Otero, 2014). Safeguarding public health in response to these risks involves timely data and surveillance. In its 2015 report on the global burden of foodborne illnesses, the World Health Organization (WHO) noted the value of national-level epidemiolocal studies and recommended them (WHO, 2015). In its Global Strategy for Food Safety, the WHO further noted that data collection is key to addressing foodborne illness and creating evidence-based food safety systems (WHO, 2022). These factors underscore the need for continuously updated Ciguatoxin poisoning epidemiology in the United States and globally as we move further into the 21st century.
Limitations
This study contained the following limitations. First, it had access only to data for those Ciguatoxin poisoning outbreaks that were brought to the attention of the public health system, which, as Radke et al. (2015), Klekamp et al., 2015), and Nalley (2024) indicated, does not capture all cases of poisoning. Second, no individual demographic information was available for outbreaks, meaning it was not possible, for example, to examine the effect of individual-level characteristics on the odds of hospitalization from seafood poisoning. Third, because NORS contains information on outbreaks involving two or more cases of illness, the dataset did not include sporadic cases involving individuals. Fourth, because the sourcing of the contaminated seafood in each outbreak was unknown, outbreaks could not be assessed for associations with environmental factors, such as tropical storms or algal blooms. Fifth, while this study examined only laboratory confirmed Ciguatoxin outbreaks reported to the CDC, there was no information about the type of Ciguatoxin (e.g., Pacific or Caribbean) or Ciguatoxin analogues involved. Sixth, because only the common names of seafood were available, species-level analysis could not be performed. Seventh, this study considered only state-level aggregated data on Ciguatoxin poisoning outbreaks, meaning it did not examine the distribution of cases or outbreaks within states for potential clustering. Lastly, public health capacity changes during the COVID-19 pandemic may have limited outbreak surveillance capacity, which may have impacted data quality and availability for 2020 and 2021.
Footnotes
Acknowledgment
The authors express their appreciation to the CDC for making data available for this study.
Authors’ Contributions
A.H.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, validation, visualization, writing—original draft, and writing—review and editing. C.P.: Supervision, conceptualization, project administration, methodology, and writing—review and editing. H.O.: Supervision and writing—review and editing. B.G.: Writing—review and editing and methodology.
Data Availability Statement
Data analyzed in this study are available from the CDC National Outbreak Reporting System. Data can be obtained by request to
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.
Disclosure Statement
The authors declare there are no competing interests.
Funding Information
The authors declare no specific funding for this work.