
Abstract
Cronobacter sakazakii is an opportunistic pathogen associated with bloodstream infections and meningitis in neonates and infants. C. sakazakii isolated from infants under 1 year of age has been reportable in Minnesota since 2003. Invasive Cronobacter infections in infants was recently made notifiable nationally in 2024. Therefore, this summary of over 20 years of reportable surveillance for C. sakazakii from Minnesota infants will inform other jurisdictions. During 2002–2024, 23 C. sakazakii cases in infants, including 8 invasive and 15 non-invasive cases, were identified and confirmed using MALDI-TOF or conventional biochemical methods. Invasive cases were younger (median, 18 days; range, 8 days to 10 months) than non-invasive cases (median, 98 days; range, 7 days to 8 months). Cronobacter isolates from infant (21), child (4), and adult (15) cases were submitted for whole genome sequencing (WGS) to obtain a contextual understanding of potential relatedness. In addition, C. sakazakii isolated from powdered infant formula (PIF) in 2003 was sequenced for comparison. Sequence type (ST) 4 was responsible for the majority of C. sakazakii cases overall (65%) and invasive infant cases (88%). Opened and unopened PIF was cultured from 10 investigations representing both invasive and non-invasive cases. Two (25%) opened PIF samples tested positive for C. sakazakii ST 4 while one (11%) unopened PIF sample tested positive for C. sakazakii ST 4. WGS demonstrated that no clinical cases were associated with a recognized outbreak. Several cases were likely due to contamination of PIF in the home during preparation, highlighting the importance of infant caregiver education to prevent infections.
Keywords
Background
The Cronobacter genus encompasses seven species: C. sakazakii, C. malonaticus, C. turicensis, C. muytjensii, C. dublinensis, C. universalis, and C. condimenti (Iversen et al., 2008; Joseph et al., 2012). C. sakazakii is an opportunistic pathogen associated with bloodstream infections and meningitis in neonates and infants, particularly those born preterm, due to their immature immune systems (Kalyantanda et al., 2015; Strysko et al., 2020; Jaradat et al., 2014; Forsythe, 2018; Joseph and Forsythe, 2012; Feeney et al., 2014). Infections in infants have been associated with contaminated powdered infant formula (PIF) (Centers for Disease Control and Prevention, 2002; Caubilla-Barron et al., 2007) and pumped breast milk (Bowen et al., 2017). Notably, C. sakazakii has been found in a wide variety of food and environmental sources (Feeney et al., 2014; Samadpour et al., 2024). Contamination of PIF can occur during production or during reconstitution and preparation (Kalyantanda et al., 2015). The fact that contamination can occur at multiple points highlights the challenges associated with investigating cases to determine if a common source can be implicated, as demonstrated during multistate case investigations in the United States in 2011 and 2021 (Centers for Disease Control and Prevention, 2012; Haston et al., 2023).
C. sakazakii isolated from infants under 1 year of age was made reportable in Minnesota in 2003. Mandatory reporting was implemented because severe cases in infants associated with consumption of contaminated PIF had been reported in the literature, and several cases were reported to the Minnesota Department of Health (MDH), including a fatal case of meningitis in 2002 (Centers for Disease Control and Prevention, 2002). The Centers for Disease Control and Prevention (CDC) receives 2–4 reports of Cronobacter infections in infants per year (Centers for Disease Control and Prevention, 2024). However, prior to 2022, Minnesota was the only state in which Cronobacter was reportable and required isolate submission, making it difficult to understand the true burden of invasive infant Cronobacter infections in the United States. Over 20 years of surveillance data for Cronobacter infections in Minnesota infants are summarized.
Methods
Inclusion criteria
C. sakazakii isolated from infants under 1 year of age, regardless of specimen source, are required to be reported to MDH. Cases were considered to have had an invasive infection if Cronobacter was isolated from a normally sterile site such as blood, cerebrospinal fluid (CSF), or abdominal fluid. The study was determined to be exempt from IRB approval.
Case investigation
Cronobacter case investigations included reviewing the patient’s clinical illness and medical history and obtaining detailed information on the case’s feeding practices, including handling and/or preparation of PIF, powdered fortifiers, breast milk, and liquid infant formula. MDH foodborne disease and health care-associated infection epidemiologists collaborated on investigations. For cases with potential health care exposure (e.g., hospitalized infant), MDH Infection Control Assessment and Response Program staff were included to consult with hospital infection prevention, nutrition, and clinical care team staff.
Testing of available opened and unopened containers of PIF was conducted for invasive Cronobacter cases in infants by the CDC and the United States Food and Drug Administration (FDA). The CDC was notified of all invasive infant Cronobacter cases and provided consultation and tested opened PIF containers. The FDA was also notified of invasive infant cases with exposure to PIF and collected and tested unopened PIF of the same lot as the case consumed.
Cronobacter isolation and identification
The isolate or clinical material from a sample positive for Cronobacter is required to be submitted to the MDH Public Health Laboratory (PHL) (Minnesota Department of Health, 2024). Isolates received prior to 2015 were identified using conventional biochemicals. Since 2015, isolates are identified using the Bruker Biotyper matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry instrument and clinical application (CA) system software database. The CA database does not differentiate between several Cronobacter species (C. sakazakii, C. dublinensis, C. muytjensii, and C. turicensis) and instead provides an identification of Cronobacter sakazakii group. Prior to 2021, pulsed-field gel electrophoresis (PFGE) was performed at MDH PHL or CDC. From 2021 through the fall of 2022 whole genome sequencing (WGS) of Minnesota isolates was conducted at CDC. Since fall 2022, MDH PHL has conducted WGS in-house on all Cronobacter isolates received, regardless of patient age, and provided the sequences to CDC for upload into the National Library of Medicine National Center for Biotechnology Information (NCBI) Bioproject PRJNA420465. In addition to this passive surveillance, there was a CDC Foodborne Diseases Active Surveillance Network (FoodNET) Cronobacter project in which clinical laboratories within Minnesota were asked to query records for all laboratory-confirmed Cronobacter isolates identified from January 1, 2003, through December 31, 2009 to better understand the incidence of Cronobacter infections (Patrick et al., 2014).
Whole genome sequencing and bioinformatic analysis
All Cronobacter isolates that were submitted to MDH PHL from January 1, 2002 through September 30, 2024 were sequenced regardless of patient age (infant, child, adult) or specimen source (invasive, non-invasive). Sequencing libraries were prepared using the Illumina DNA Prep Library preparation kit and sequenced using the Illumina MiSeq™ v2 (2 × 250 PE) chemistry. Genomes were run through the Spriggan 1.1.2 bioinformatics workflow (https://github.com/wslh-bio/spriggan) for genome assembly and multilocus sequence type (ST) determination. Reference-based single nucleotide polymorphism (SNP) analysis was performed on isolates with the same ST using the CFSAN pipeline as part of the Dryad 3.0.0 (https://github.com/wslh-bio/dryad/) workflow. A phylogenetic tree was generated using RAxML (Stamatakis, 2014) and visualized using MEGA7 (Kumar et al., 2016).
Results
Infant C. sakazakii cases
During 2002–2024, 21 C. sakazakii cases in infants were reported to MDH. Two additional non-invasive cases were identified during the retrospective FoodNET Cronobacter project, resulting in a total of 23 infant C. sakazakii cases included in this study. There were 8 (35%) invasive and 15 (65%) non-invasive cases (Fig. 1). Specimen sources included 7 (30%) blood, 5 (22%) CSF, 4 (17%) tracheal aspirate, 3 (13%) throat swab, 3 (13%) urine, 2 (9%) stool, 1 (4%) sputum, and 1 (4%) pharyngeal swab. Three (13%) cases had positive blood and CSF cultures, and two infants (9%) died. The median age for infant cases overall was 44 days (range, 7 days to 10 months). Invasive cases were younger (median, 18 days; range, 8 days to 10 months) than non-invasive cases (median, 98 days; range, 7 days to 8 months). Only 2 (25%) invasive cases occurred in infants over 2 months of age, compared to 9 (60%) non-invasive cases. Nine (57%) of the 21 cases with information on sex were female. Of the 8 invasive cases, 4 (50%) had no known underlying medical conditions, two were born preterm (32 and 36 weeks), 1 had prematurity (33 weeks) with respiratory and neurological complications, and 1 had malignancy and an indwelling catheter. The FoodNET Cronobacter project did not identify additional invasive cases that had not been previously reported.

Epidemiological Curve of Infant Cronobacter sakazakii Cases, Minnesota, 2002–2024. Invasive cases are shaded dark green, non-invasive cases are light green. D indicates the case died, O indicates that opened PIF consumed by the case tested positive for C. sakazakii, U indicates that unopened PIF consumed by the cases tested positive for C. sakazakii, and FN indicates cases that were identified during the FoodNet survey of clinical laboratories.
PIF was tested in 10 case investigations, representing 7 invasive and 3 non-invasive cases. Opened PIF was tested in eight investigations, representing six invasive and two non-invasive cases, and two (25%) samples tested positive for C. sakazakii ST 4. A 2011 case isolate was indistinguishable by PFGE from the C. sakazakii isolate recovered from opened PIF (Fig. 2). A 2021 case isolate was 0 SNPs from a C. sakazakii ST 4 isolate obtained from opened PIF consumed by the case. Additional C. sakazakii isolates were obtained from opened PIF and opened bottled water used to prepare formula for the 2021 case. These were 0–7 SNPs from each other and >50,000 SNPs from the clinical case isolate (Haston et al., 2023). C. sakazakii isolates from opened PIF and bottled water were cultured at another laboratory and are not included in the phylogenetic tree (Fig. 2). Unopened PIF was tested in nine investigations, representing seven invasive and two non-invasive cases, and one (11%) tested positive for C. sakazakii ST 4. That isolate (2003B_PIF) was not closely related to the clinical isolate by PFGE but resulted in a recall. No C. sakazakii cases were part of a recognized outbreak.
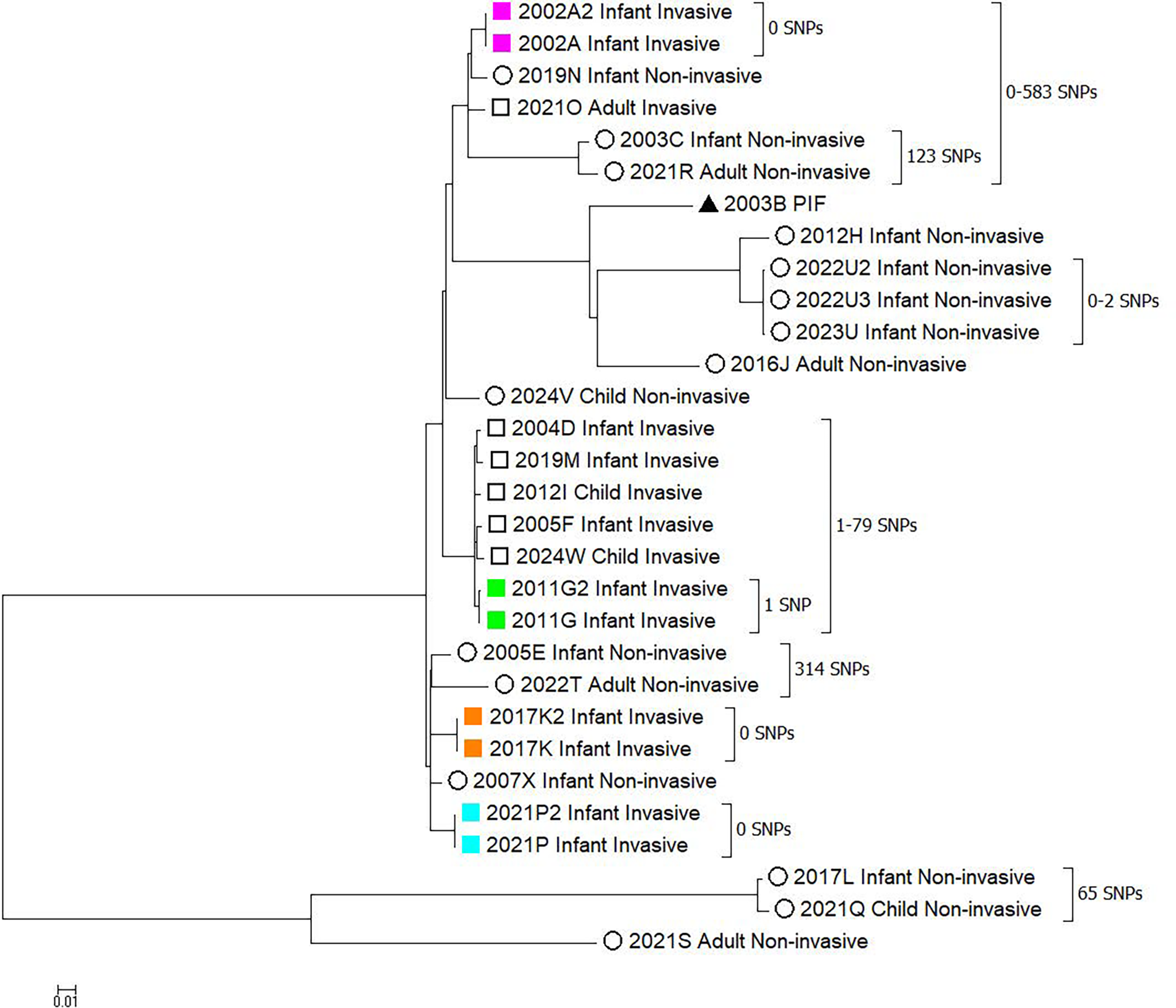
Relatedness assessment of Cronobacter sakazakii ST 4 isolates, Minnesota 2002–2024. The maximum likelihood phylogeny obtained from reference-based single nucleotide (SNP) analysis of ST 4 C. sakazakii isolates. SNP analysis was performed using the bioinformatics pipeline Dryad 3.0.0 and 2005F_Infant_Invasive as the reference genome. The core genome size for 30 genomes was 3,991,050 base pairs, which equals 89% of the mapping reference genome. Isolates are named with the year of isolation, age of the individual (infant, child, or adult), and if the infections were invasive or non-invasive. Squares represent invasive infections, circles non-invasive infections, and the triangle represents the isolate from PIF. Matching colors indicate multiple isolates from the same individual case.
Whole genome sequencing analysis
MDH PHL conducted sequencing on all Cronobacter isolates that were submitted to the PHL with specimen collection dates from February 4, 2002 through July 31, 2024, regardless of specimen source or age of the case (See the Supplementary Data for isolate metadata). In total, 43 isolates from 36 C. sakazakii cases were sequenced including 20 from infants (8 invasive and 12 non-invasive), 4 from children (2 invasive, and 2 non-invasive), and 12 from adults (1 invasive, 11 non-invasive). Isolates for 20 (87%) of the 23 reported C. sakazakii infant cases were available for sequencing. Isolates were not received at MDH PHL for a 2017 non-invasive case and the two non-invasive cases identified through the retrospective FoodNET Cronobacter project.
Three infant isolates that were initially reported as C. sakazakii were determined to be other species by sequencing. One isolate was determined to be C. dublinensis. Two isolates were determined to not be Cronobacter species and were excluded from further analyses: a urine isolate collected from a 29-day-old infant was identified as Enterobacter asburiae, and a blood isolate collected from a 5-day-old infant was identified as Enterobacter cloacae. Additionally, four isolates from adults that were initially reported as C. sakazakii were determined to be C. malonaticus.
Five cases had multiple specimens obtained with C. sakazakii isolated and sequenced from each specimen. Four cases had C. sakazakii isolated and sequenced from blood and CSF collected within 1 day of the original specimen and were 0–1 SNPs apart (2002A/A2; 2011G/G2; 2017K/K2; 2021P/P2) (Fig. 2). The remaining case included 3 C. sakazakii isolates (2022U, 2022U2, 2022U3) all from non-invasive specimen sources (tracheal aspirate, tracheostomy wound site, and sputum) and collection dates spanning 206 days. The first two isolates (2022U and 2022U2), collected 56 days apart, were 0 SNPs from each other, and the third isolate (2022U3), collected 150 days after the second specimen, was two SNPs from the first two (Fig. 2). Physicians determined that these isolations represented persistent colonization, which was further supported by the WGS results showing limited genetic change over the 206 days.
Seven different ST delineations were identified among the 43 C. sakazakii isolates sequenced. Table 1 provides a breakdown of patient demographics and average SNP differences among each ST. The majority of C. sakazakii isolates fell within ST 4, representing 23 cases, 6 duplicate case isolates, and 1 isolate from PIF. Of note, C. sakazakii ST 4 was isolated from unopened PIF (2003B PIF); however, an unrelated C. sakazakii ST (ST 283) was obtained from a clinical case that consumed PIF from the same lot, but different container.
Cronobacter Multilocus Sequence Typing by Age and Invasive Specimen Source, Minnesota 2002–2024
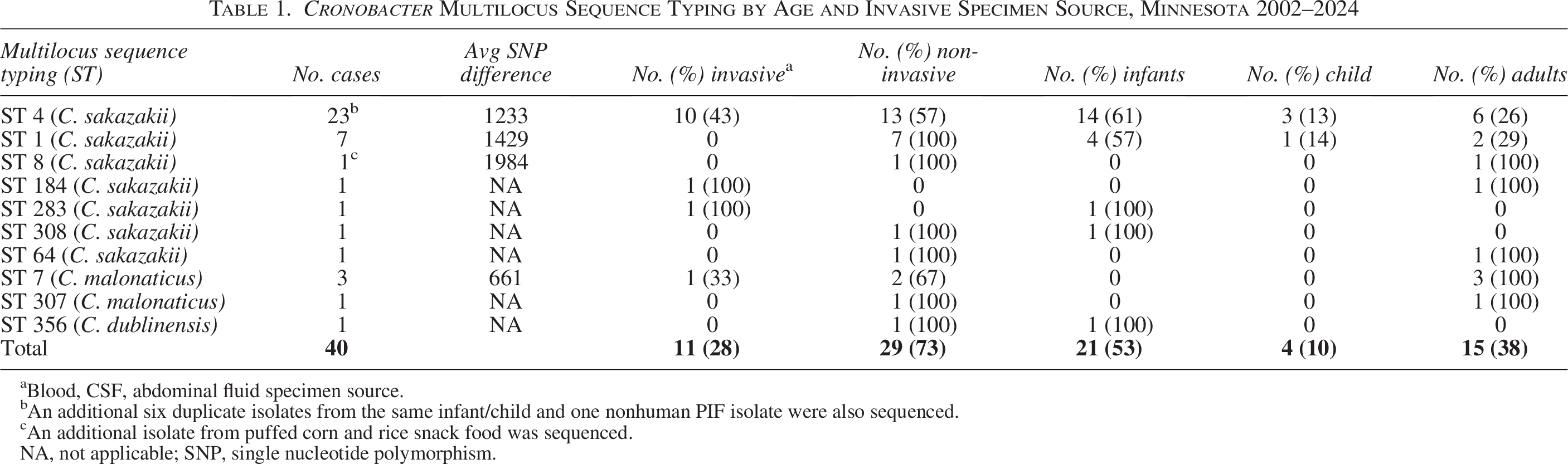
Blood, CSF, abdominal fluid specimen source.
An additional six duplicate isolates from the same infant/child and one nonhuman PIF isolate were also sequenced.
An additional isolate from puffed corn and rice snack food was sequenced.
NA, not applicable; SNP, single nucleotide polymorphism.
SNP analysis showed that invasive C. sakazakii ST 4 case isolates were more closely related to each other than non-invasive case isolates, with an average of 213 (range, 37–377) versus 1918 (range, 65–4697) SNP differences, respectively (Fig. 2; squares [invasive isolates], circles [non-invasive isolates]). There is no accepted SNP threshold to determine relatedness; therefore, generalizations were inferred from these data using epidemiological information for comparison. ST 4 cases included a grouping of isolates from six invasive cases (four infants and two children) that were 37–79 SNPs from each other and represented 50% of the invasive infant cases (Fig. 2). These cases occurred over 20 years (2004, 2005, 2011, 2012, 2019, and 2024) and had no identified geographic or epidemiological connection to each other. The 2004 case (2004D Infant Invasive) occurred in an 8-month-old infant whose infection was due to a central line infection and did not consume PIF. The 2005 case (2005F Infant Invasive) was a 44-day-old infant who had consumed PIF that tested negative for C. sakazakii. The 2011 (2011G Infant Invasive) case was a 10-day-old infant who had consumed a different brand of PIF than the aforementioned case. Opened PIF consumed by 2011G tested positive for C. sakazakii that was 13 SNPs from the clinical case isolate (data unavailable; PIF testing and sequencing performed by CDC), whereas an unopened PIF container of the same lot tested negative, suggesting that contamination of PIF during preparation in the home was the most likely source of this case’s infection. The 2012 (2012H Infant Non-invasive) case was a 2-year-old non-Minnesota resident with limited epidemiological information but who was being fed through a gastro-jejunal tube. The 2019 (2019N Infant Non-invasive) case was an 8-day-old infant who consumed PIF, of which opened and unopened container samples tested negative for C. sakazakii. The 2024 case (2024W Child Invasive) was an 18-month-old who consumed ready-to-feed formula through a gastrostomy tube.
Discussion
Invasive C. sakazakii infections in Minnesota infants are uncommon. Case investigations include assessment of feeding exposures and the potential for environmental contamination during production, preparation, and/or handling; therefore, investigations require a multidisciplinary team with expertise in foodborne disease and infection control in close collaboration with CDC and FDA. Data from the FoodNet active surveillance project suggest that invasive infant C. sakazakii cases are being reported to MDH, but non-invasive C. sakazakii cases are likely underreported. The 2023 passage of a Council for State and Territorial Epidemiologists position statement, which established a standard case definition and made invasive Cronobacter infections in infants nationally notifiable, will likely increase the number of cases that are identified nationally as additional jurisdictions make Cronobacter infections reportable (McBee et al., 2023). The 20+ years of reportable surveillance for C. sakazakii in Minnesota infants will inform these efforts and prompt investigation of these cases using established methods will help us learn more about the epidemiology of Cronobacter (Council of State and Territorial Epidemiologists, 2024).
Comparison of case-isolates with PIF or environmental samples can provide critical information to determine the source of a case’s infection. The lack of clinical isolates for some cases in national investigations has hindered the ability to determine if temporally associated cases could represent a common source outbreak (Haston et al., 2023; Centers for Disease Control and Prevention, 2012). Public health staff should promptly request clinical isolates be sent to their public health laboratory or CDC when notified of an invasive case of C. sakazakii in an infant to ensure that the isolate is not discarded by the clinical laboratory.
Sequencing revealed two non-Cronobacter species isolates and four isolates of Cronobacter species that were not C. sakazakii among cases that were initially reported as C. sakazakii. This highlights the challenges in accurately identifying this organism using classical microbiology methods. Confirmation of suspected Cronobacter species can be done at a state or jurisdictional PHL or at CDC.
Sequencing did not identify closely related isolates beyond the instances where multiple isolates were collected from the same case patient. Three closely related isolates (0–2 SNPs) from the same patient collected over 7 months suggests persistent colonization with C. sakazakii can occur. The majority of the C. sakazakii isolates were ST 4, and invasive ST 4 cases exhibited fewer SNPs than non-invasive cases (average 213 vs. 1918 SNPs). Additional research such as virulence factor analysis could help explain the increased pathogenicity and disease severity of these strains.
It is not uncommon to find multiple strains of C. sakazakii in clinical, PIF, or environmental samples (Samadpour et al., 2024; Haston et al., 2023; Masood et al., 2015); this occurred in two Minnesota case investigations. Multiple strains of C. sakazakii were isolated from opened PIF and opened bottled water during a 2021 case investigation (Haston et al., 2023), and during a 2003 case investigation, unopened PIF tested positive for a different C. sakazakii ST than the isolate from the clinical case who had consumed that lot of PIF (data not shown). Additionally, in an analysis of an outbreak investigation in France, multiple C. sakazakii strains were isolated from the same clinical cases (Masood et al., 2015). These data suggest that contamination of PIF with multiple C. sakazakii strains and polyclonal infections occur, which could make it more difficult to detect common source PIF outbreaks using traditional methods of enteric disease outbreak identification by linking cases using WGS. Ensuring that multiple C. sakazakii isolates from environmental, PIF, and clinical samples are sequenced could help overcome this limitation.
The two invasive infections that occurred in children over 1 year of age were in children that were both being fed through feeding tubes (gastrostomy and gastrojejunostomy tubes), suggesting this feeding method could be a risk factor for older children with underlying medical conditions.
The investigation of non-invasive C. sakazakii detections in infants can be challenging, as it is often difficult to determine if these detections represent an infection versus colonization. MDH does not routinely conduct a full case investigation, e.g., testing of opened and unopened PIF, for all non-invasive cases but evaluates each on a case-by-case basis to determine if testing is warranted.
No cases were associated with a recognized outbreak. Several cases were likely due to contamination of PIF in the home during preparation, highlighting the importance of infant caregiver education to prevent infections. Health care providers should provide education to caregivers of infants at higher risk for invasive C. sakazakii infection (under 2 months of age, those who were born prematurely, or are immunosuppressed). This education should cover safe hygiene, preparation, and storage practices, discussing alternatives to PIF, and the importance of thoroughly cleaning and sanitizing breast pump equipment for infants that are fed expressed milk (Centers for Disease Control and Prevention, 2023; Centers for Disease Control and Prevention, 2022; World Health Organization, 2007).
Authors’ Contributions
J.R.: Conceptualization (supporting); Writing—original draft (lead); Formal analysis (lead); Writing—review and editing (supporting). J.L.D.: Writing—original draft (supporting); Methodology (lead); Conceptualization (supporting); Review and editing (supporting); A.G.: Investigation (supporting); Formal analysis (supporting); Writing—original draft (supporting); Methodology (supporting); Review and editing (supporting); L.E.T.: Review and editing (supporting); Investigation (supporting); P.S.V.: Review and editing (supporting); Writing—original draft (supporting); Investigation (supporting); Methodology (supporting); K.S.: Review and editing (supporting); Conceptualization (supporting); Methodology (supporting); C.M.: Review and editing (supporting); Conceptualization (Lead); Methodology (supporting); R.L.: Review and editing (lead); Conceptualization (supporting); Methodology (supporting).
Footnotes
Acknowledgment
The authors would like to thank CDC and FDA staff for their expertise and assistance in conducting Cronobacter case investigations.
Funding Information
This work was supported in part through a cooperative agreement with the Centers for Disease Control and Prevention Epidemiology and Laboratory Capacity for Infectious Diseases Program [U50/CK000371].
Disclosure Statement
No competing financial interests exist.