
Abstract
Taenia saginata, commonly known as the beef tapeworm, is a prevalent zoonotic cestode with an estimated global prevalence of 60–70 million carriers. This parasite is frequently located in the gastrointestinal tract, and previous reports have described complications such as acute appendicitis, Meckel’s diverticulitis, pancreatitis, cholecystitis, liver abscess, intestinal obstruction, and perforation. Intestinal perforation due to parasitic diseases is a rare complication. Surgical complications associated with T. saginata are uncommon, with few reported cases of bowel perforation. Here, we present the case of a 69-year-old female who was admitted to the emergency department with acute abdominal symptoms. She had experienced abdominal pain and vomiting for 15 days. Her symptoms were accompanied by abdominal distension, reduced bowel movements, and loss of appetite. On physical examination, she had diffuse abdominal tenderness, guarding, and rebound tenderness, raising suspicion of peritonitis. Laboratory tests revealed a white blood cell count of 8,000/mm3 and an elevated C-reactive protein level of 501 mg/L, indicating an ongoing inflammatory response. Imaging revealed free intra-abdominal air and fluid, suggesting gastrointestinal perforation. During emergency surgery, a perforation in the upper rectum was identified and resected. Pathological examination confirmed the presence of T. saginata eggs in the intestinal wall. Postoperatively, the patient recovered well and was discharged on the sixth day. This case underscores the need for heightened awareness of parasitic infections as potential causes of acute abdominal conditions. Proper diagnosis and prompt surgical intervention are crucial in managing complications associated with T. saginata. Preventive measures, including thorough cooking of beef and improved sanitation, are essential to reduce the incidence of such infections.
Introduction
Taenia saginata, commonly known as the beef tapeworm, is a widespread zoonotic platyhelminth of the class Cestoda. T. saginata has an estimated global prevalence of 60–70 million carriers (Eichenberger et al., 2020). They are frequently found in the gastrointestinal tract and are transmitted to humans by consuming raw or undercooked meat. The parasite is endemic in Asia and is seen in 86% of the Middle East and North Africa region (Saratsis et al., 2019). Parasitic infestations of the gastrointestinal system remain a significant health issue in the 21st century. They are commonly observed in underdeveloped or developing countries. T. saginata (4–12 m in length) and Taenia solium (3–7 m in length) are two common cestode species. T. saginata is the most frequently encountered species in Turkey, especially in the southeastern region (Şahin et al., 2023).
In addition to its medical burden, the infection causes significant losses in the meat processing industry and threatens food safety, making T. saginata a major economic concern (Symeonidou et al., 2018). Cattle and buffalo serve as intermediate hosts, whereas humans are the definitive hosts (Saratsis et al., 2019). The parasite causes taeniasis in humans and cysticercosis in cattle (Braae et al., 2018). Humans can become infected by consuming raw or undercooked beef containing cysticerci. The prevalence of taeniasis is high in Turkish cuisine due to its rich use of raw beef (Şahin et al., 2023). In the human intestine, the parasite matures into an adult worm that can live for many years within the host’s body (Braae et al., 2018). These parasites are typically solitary. The head (scolex) of the tapeworm, equipped with attachment organs (four prominent suckers), attaches to a point in the duodenojejunal wall, whereas the body (strobila) moves freely in the intestinal lumen. The adult stage of T. saginata is one of the most common pathogenic cestodes in humans. The adult worm is generally <5 m in length but can reach up to 25 m (Braae et al., 2018). Detection of the tapeworm relies on stool examination for eggs. The perianal region can also be examined using a cellophane tape swab to detect eggs (Braae et al., 2018; Fan et al., 1992; Jongwutiwes et al., 2004; Sozutek et al., 2011; Symeonidou et al., 2018).
Taeniasis is often asymptomatic; patients typically complain of the passage of proglottids in their stool. However, it can present with pruritus ani (77%), nausea (46%), abdominal pain (43%), dizziness (42%), increased appetite (30%), and other mild gastrointestinal symptoms (Fan et al., 1992). It may also lead to complications related to the gastrointestinal system, such as obstruction, perforation, or anastomotic leakage. The migration of proglottids into the gastrointestinal lumen can lead to rare but severe acute surgical conditions. Previous case reports have described several complications associated with Taenia during surgery, including acute appendicitis, Meckel’s diverticulitis, pancreatitis, cholecystitis, liver abscess, obstruction, and perforation of the intestine, as well as anastomotic leakage (Sozutek et al., 2011). Perforations typically occur in the small intestine, particularly the jejunum. Intestinal perforation is a rare complication in parasitic diseases (Jongwutiwes et al., 2004). Abdominal surgical complications related to T. saginata are uncommon (Vallverdù Scorza et al., 2015).
A review of the literature reveals a number of cases reporting intestinal perforation as a complication of taeniasis (Akarsu et al., 2013; Atef and Emna, 2015; Bahon et al., 1997; Bordon, 1992; Crompton, 1999; Kennedy et al., 1989; Nematihonar et al., 2023; Ochoa, 1991; Patterson et al., 1993; Wu et al., 1999). To date, intestinal perforations due to various helminth infections such as ascariasis, angiostrongyliasis, enterobiasis, trichuriasis, schistosomiasis, acanthocephaliasis, taeniasis, and strongyloidiasis have been reported worldwide (Bahon et al., 1997; Kennedy et al., 1989; Ochoa, 1991; Patterson et al., 1993; Wu et al., 1999). However, rectal perforation due to T. saginata has never been observed. In this study, we present a case of rectal perforation associated with T. saginata infection. To our knowledge, this has not been previously reported in the literature.
Case Report
A 69-year-old female patient of Turkish ethnicity, born in Beykoz, Istanbul, presented to the emergency department on January 13, 2022, with acute abdominal findings. She had been experiencing abdominal pain and vomiting for 15 d. Physical examination revealed widespread distension, guarding, and rebound tenderness. Laboratory tests revealed a white blood cell count of 8,000/mm3 and an elevated C-reactive protein level of 501 mg/L, indicating an ongoing inflammatory response. Differential blood count showed neutrophilia (Neut% 96) with normal eosinophil levels (EOS: 0.1 × 103/μL, EOS%: 1.6). The absence of eosinophilia, which is typically expected in parasitic infections, may be attributed to the overwhelming inflammatory response caused by intestinal perforation. Hemoglobin was 14.2 g/dL, hematocrit 42.6%, and renal function tests were within normal limits (creatinine: 0.82 mg/dL). Liver function tests showed AST: 17.9U/L, ALT: 9.3U/L, and ALP: 71U/L, indicating no significant hepatic dysfunction. Abdominal computed tomography scan demonstrated free air density below the diaphragm (Fig. 1), free intraperitoneal air and fluid densities, heterogeneity in the omental fat tissues, and segmental wall thickening of the upper rectum (Fig. 2).

Free air density below the diaphragm.
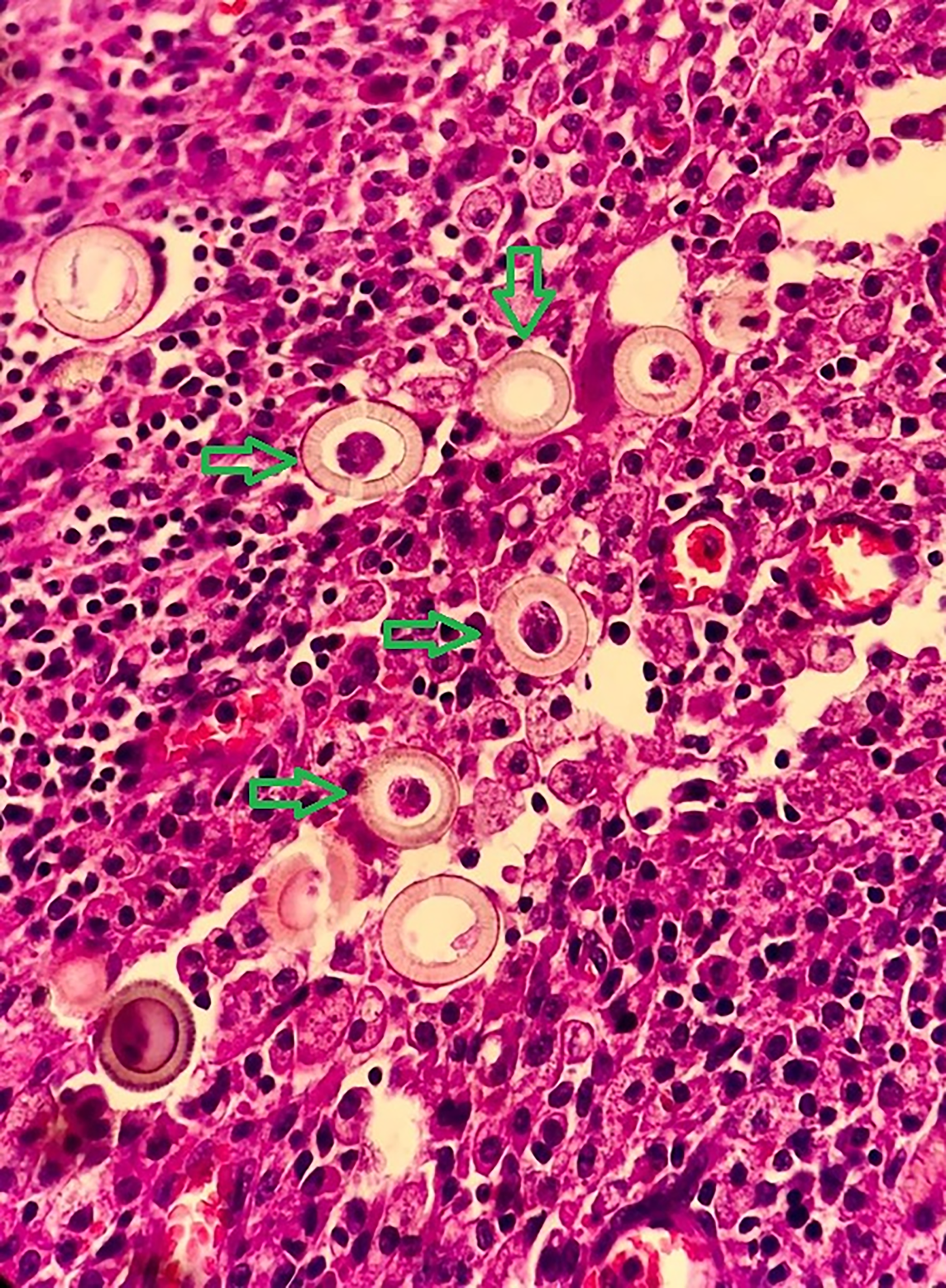
Histological section of the intestinal wall with suppurative inflammation and eggs of Taenia saginata in it, at 40× magnification. Hematoxylin and eosin-stained section obtained from the perforated rectal wall, displaying characteristic thick-walled embryonated eggs of T. saginata. The presence of these eggs within the necrotic tissue confirms parasitic involvement in the perforation etiology.
The patient was taken for emergency surgery, during which widespread fecal contamination was observed in the abdominal cavity. Exploration revealed a perforation area in the upper rectum. Macroscopic examination of the resected specimen revealed a 3.5 × 2.5 cm perforation site. The perforated segment, including 10 cm proximally and 2 cm distally, was resected according to oncological principles, considering the potential for malignancy, along with total mesorectal excision. A Hartmann’s procedure with an end colostomy was performed. The abdomen was irrigated, and drains were placed. Pathological examination showed marked ischemic necrosis in the serosa and parasite eggs (T. saginata) within the layers of the intestinal wall (Fig. 2). No other pathology was observed.
Follow-up
After the operation, the patient was followed in the service. Third-generation cephalosporin (intravenous ceftriaxone 1 g every 12 h) and metronidazole (3 × 1) were started. On the second postoperative day, the patient’s colostomy bag started to function, the nasogastric tube was withdrawn, and oral nutrition with watery food was initiated. The drain was removed on the fourth postoperative day, and she was discharged on the sixth day of her admission because her oral intake was normal, her abdominal examination was unremarkable, and her inflammatory parameters had decreased to normal levels.
After starting oral nutrition, the patient was administered a single dose of niclosamide 2 g oral tablets (four tablets). She was discharged with this treatment. The patient was called for follow-up in the third month after the operation, and no issues were observed during this checkup. No complications were noted. Subsequent colonoscopies during postoperative follow-ups revealed no additional pathology. The colostomy was closed in June 2022.
Discussion
Taenia spp. includes T. saginata, T. solium, and T. asiatica, which is very close in features to T. saginata. T. saginata is the most common tapeworm infestation in humans, which may cause gastrointestinal tract complications due to obstruction, perforation, or anastomotic leakage (Dural et al., 2015). Taeniasis is usually asymptomatic, with patients often noticing proglottids in the stool. Occasionally, mild symptoms such as nausea, weight loss, and abdominal discomfort occur. Rarely, it can cause severe conditions such as jejunal perforation and peritonitis (Dural et al., 2015; Symeonidou et al., 2018). We present a severe surgical case of T. saginata causing rectal perforation. This highlights the need to consider T. saginata in patients with gastrointestinal symptoms, especially where raw beef consumption is common. Among parasitic infections, its adult stage is one of the most common pathogenic cestodes in humans (Akarsu et al., 2013). Factors such as tourism, migration, and military operations can lead to the spread of this parasitic infection to previously unaffected communities. Therefore, it should be considered a global issue (Braae et al., 2018).
Epidemiological data from Turkey indicate that the prevalence of T. saginata varies regionally. A study conducted at Eskişehir Osmangazi University between 2003 and 2007 found T. saginata in 0.8% of 34,733 stool samples analyzed (Doğan et al., 2008). Another study from Istanbul reported a prevalence of 2.42% among 20,948 patients presenting to a university hospital (Polat et al., 2020). In addition, a historical dataset from Elazığ revealed that 2.3% of 25,077 stool samples examined between 1987 and 1993 contained T. saginata eggs (Aşçı et al., 1998). These findings highlight the ongoing public health impact of taeniasis in Turkey, particularly in regions with high consumption of raw or undercooked beef.
Most infected individuals are asymptomatic unless they notice proglottids in their stools (Nematihonar et al., 2023). The most surgical manifestation of taeniasis is abdominal pain, malnutrition, obstruction, inflammation, and perforation of the small intestine, appendix, or colon (Bhandari et al., 2022; Demiriz et al., 1997; Dural et al., 2015; Lenoble and Dumontier, 1988; Symeonidou et al., 2018). Local inflammatory reactions or obstruction due to an impacted tapeworm, bowel perforation, and consecutive peritonitis may occur (Bhandari et al., 2022). Complaints from patients such as feeling discomfort in the anal region when passing proglottids or noticing a worm in their stool or underwear should raise suspicion of taeniasis (Lenoble and Dumontier, 1988). However, our patient did not mention any issues related to the tapeworm.
Compared to small intestine perforations, colonic perforation due to T. saginata is a very rare complication (Bahon et al., 1997; Demiriz et al., 1997; Sozutek et al., 2011). The parasite may invade the small intestine before reaching the colon. Small intestine perforation mortality rates can reach 42%, depending on the primary disease (Kalaycı, 2022). A case of colonic perforation caused by taeniasis and misinterpreted as colon carcinoma on ultrasonographic examination has been reported from Turkey (Demiriz et al., 1997). A Turkish case report described a 28-year-old male with abdominal pain, nausea, and vomiting, whose appendix specimen showed acute appendicitis with T. saginata segments (Buzio et al., 1999). However, no report for rectum perforation was found in the literature.
Rare cases of tapeworm infestations requiring surgery have been reported. A 2012 case showed that a thickened gastrointestinal wall made perforation by Taenia less likely (Hakeem et al., 2012). Typically, there is a trigger that causes or prepares the wall for perforation. Another report by Faheem (Faheem et al., 2012) described a rare case of T. solium peritonitis with multiple ileal perforations. T. saginata can particularly cause acute appendicitis and gastrointestinal perforations, as well as acute cholecystitis, pancreatitis, and gastrointestinal bleeding (Bekraki and Hanna, 2016). They have also been reported to cause anastomotic leakage in the postoperative period. Migration to the bile ducts can lead to cholangitis (Uygur-Bayramiçli et al., 2012). In line with our case report, Taenia continues to be a direct cause of intestinal perforation and should be considered in the differential diagnosis of peritonitis and acute abdomen in endemic geographic regions.
Surgery is recommended only for the treatment of complications (Nematihonar et al., 2023; Sozutek et al., 2011). Treatments applied in cases of T. saginata requiring surgical intervention and causing gastrointestinal perforation reported in the literature are presented in Table 1.
Patients with Gastrointestinal Perforation Associated with Taenia saginata and Treatments Administered

T. saginata is transmitted through raw or undercooked meat. The scolex attaches to intestinal tissue, developing into proglottids that release eggs via feces, contaminating water and soil. These eggs can be ingested by cattle or humans, leading to reinfection. Preventive measures are essential to interrupt transmission (Kalaycı, 2022). Preventive strategies include thoroughly cooking beef for more than 5 min at temperatures exceeding 60°C (Braae et al., 2018), which helps to destroy any cysticerci present. In addition, maintaining good hygiene and ensuring safe practices in meat processing are essential to prevent these infections.
Recognizing surgical pathologies linked to parasitic infections can reduce mortality and morbidity. In endemic regions, parasites may necessitate surgical intervention. Surgeons should consider Taenia species in differential diagnoses, as taeniasis, though rare, can present as acute abdomen.
Conclusions
This case report highlights the rare and severe complication of rectal perforation due to T. saginata infection. Despite being a common zoonotic cestode, T. saginata often presents with minimal or no symptoms, leading to underdiagnosis and potential for serious complications. The presented case underscores the importance of considering parasitic infections in the differential diagnosis of acute abdominal conditions, particularly in regions with prevalent raw beef consumption. Effective management of T. saginata infections requires prompt diagnosis and appropriate surgical intervention in cases of complications. Antiparasitic treatment with medications such as praziquantel or niclosamide is crucial in eradicating the infection and preventing recurrence.
Preventive measures are vital in controlling the spread of T. saginata. Ensuring thorough cooking of beef, improving meat inspection processes, and enhancing public awareness about the risks of consuming raw or undercooked meat can significantly reduce the incidence of taeniasis. In addition, improved sanitation and hygiene practices are essential to prevent contamination of food and water sources with parasite eggs. This case emphasizes the need for health care professionals to remain vigilant for parasitic infections, especially in endemic areas. Early recognition and treatment of taeniasis can prevent severe complications and improve patient outcomes. The inclusion of parasitic infections in differential diagnoses and the implementation of preventive strategies are crucial steps in managing and reducing the burden of T. saginata and other parasitic diseases.
Authors’ Contributions
N.K.: Study concept, design, data collection, data analysis, interpretation, and article drafting. A.G.Y.: Data collection, data analysis, interpretation, final approval, and accountability. G.E.: Critical revision, final approval, and accountability. All authors declare that they have contributed to the study and take full responsibility for its contents.
Footnotes
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical Approval
The authors confirm that the study was conducted in compliance with the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from the patient for the publication of this case report, including any accompanying images. This case report was exempt from institutional review board approval according to the institutional policy, as it involved a single patient case with fully anonymized data and written informed consent.
Disclosure Statement
The authors declare no financial or personal conflicts of interest related to the conduct, writing, or publication of this article.