
Abstract
Abstract
Objective:
Impaired balance is disabling for children with cerebral palsy (CPc), especially for CPc who recently underwent lower limb surgery. Positive results of using virtual reality (VR) in balance rehabilitation have been published in several outpatient populations. We investigated the feasibility of applying additional VR training focused on sitting balance in CP inpatients of a rehabilitation center after lower limb surgery. Additionally, we investigated the rate of enjoyment of VR training compared with conventional physiotherapy.
Materials and Methods:
Eleven spastic CPc (4/7 males/females) following rehabilitation after lower limb orthopedic surgery were included (5–18 years). The control group received conventional physiotherapy. The intervention group received additional VR training. Balance was measured using the Trunk Control Measurement Scale every 3 weeks of the rehabilitation period. Enjoyment was analyzed using a 10-point Visual Analog Scale.
Results:
Providing additional VR training was feasible in terms of recruitment, treatment adherence, and assessment adherence. Both groups improved sitting balance after therapy. The current games were not perceived as more enjoyable than conventional physiotherapy.
Conclusion:
Including additional VR training to conventional physiotherapy is feasible and might be promising to train sitting balance in CPc after lower limb surgery. Future research should take equal patient allocation and training duration between groups into consideration.
Introduction
C
A highly disabling factor for children with CP (CPc) is their impaired balance. 4 It influences the performance of everyday activities such as walking ability. 5 Therefore, balance training is a key element in CP rehabilitation. 6
There is growing interest in balance training for CPc using innovative/alternative tools, such as the Biodex Balance System,7,8 hippotherapy,9,10 and virtual reality (VR) games. 11 The use of VR games in rehabilitation is growing since literature has indicated that it increases the participant's motivation and improves functional outcomes and motor performance.12–15 The advantages of VR use are based on several key concepts relevant to motor learning, such as the use of feedback, motivation, and repetition. 15 Feedback motivates the participants to perform better. 16 In this regard, VR is a useful medium to enhance the number of repetitions needed to induce neuroplasticity.17,18
Consequently, VR games have been applied as a rehabilitation tool for balance in several patient populations such as stroke, acquired brain injury, and Parkinson's disease. 15 Even though the use of VR games in CP rehabilitation is increasing,11,19,20 there is only a limited amount of research concerning its use in the postoperative rehabilitation of CPc. To the best of our knowledge, the study by Sharan et al. 21 is the only study indicating that additional VR therapy in a postoperative setting could be favorable to train balance in CPc. 21 However, the authors did not specify the type of diagnosed CP and type of surgery the patients had undergone. Furthermore, the VR therapy was based on commercial off-the-shelf games not specifically designed to train balance in disabled children. The outcome measure used (pediatric balance scale [PBS]) was an overall clinical measurement scale for balance, including items during sitting as well as standing. As such, the question remains whether the reported increase in PBS score is due to actual improvements in balance or due to the ability to stand upright. Furthermore, it is unclear whether this improvement is maintained at follow-up.
To address the issues raised, we used VR games especially developed to address balance problems in CPc (after lower limb orthopedic surgery). To minimize the effect of the ability to stand, a specific measurement scale (developed for CPc) is used to assess sitting balance. Moreover, the effects of the program after a follow-up were assessed.
The aim of the current study was to examine the feasibility (in terms of recruitment, treatment adherence, and assessment process) and patient enjoyment of using additional VR training in a rehabilitation center for CPc after lower limb orthopedic surgery. The implementation of the VR intervention was deemed feasible when 80% of the potential participants agreed to participate and adhered to the training program.
Materials and Methods
Participants
For this monocentric, two-group, pretest–post-test feasibility study, CPc who stayed at the rehabilitation center at University Hospital of Pellenberg (UZ Leuven, Belgium) for rehabilitation after orthopedic surgery of the lower limbs from March 2014 until December 2014 were recruited. Participants (and parents) who met following criteria were approached and asked for participation in the study: (1) spastic CP, (2) 5–18 years, and (3) GMFCS I–IV. Patients who underwent only botulinum toxin treatment or who underwent baclofen pump implantation were excluded due to limited hospitalization period. Patients with dorsal rhizotomy were excluded as trunk rotations were contraindicated. Experiments were approved by the local ethics committee (Clinical Trial Center—University Hospital Leuven; Approval s56332) and performed with informed written consent. The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Sample size was determined by the number of participants who met the inclusion criteria during the duration of the study. Based on this pilot, a power calculation can be performed to estimate the sample size of an upcoming randomized controlled trial.
Twelve participants met the inclusion criteria. One patient did not show sufficient cooperation to take part in the study, and no informed consent was obtained (Supplementary Data S1; Supplementary Data are available online at www.liebertpub.com/g4h). Thus, eleven participants (seven females, four males) were enrolled (Table 1); 91.67% of the contacted persons participated.
A.con–G.con, participants of the control group; A.int–D.int, participants of the intervention group; Add, adductors; AL, adductor longus; AT, Achilles tendon; Bilat, bilateral; Dist, distal; DO, derotation osteotomy; DVO, derotation varization osteotomy; EDO, extension derotation osteotomy; Endo, endorotation; EVO, extension varization osteotomy; F, female; FD, flexor digitorum; G, gastrocnemius; GR, gracilis; IP, iliopsoas; L, left; M, male; Prox, proximal; R, right; RF, rectus femoris; S, soleus; SM, semimembranosus; SPLATT, split anterior tibial tendon transfer; SPOTT, split posterior tibial tendon transfer; ST, semitendinosus; TA, tibialis anterior; VO, varization osteotomy.
Participants were allocated to the intervention (n = 4) or control group (n = 7) according to their hospitalization period by a physiotherapist from University Hospital Pellenberg. Participants who received postsurgery training from March until June 2014 were allocated to the control group. Participants with rehabilitation from July until December 2014 were allocated to the intervention group. This design was chosen as the games were not yet functional at the start of the testing period. Therapists, investigators, participants, and parents were not blinded to group allocation.
Procedure
CPc received conventional rehabilitation therapy starting 6 weeks after surgery until discharge from the hospital. Every child received 2 hours of physiotherapy and 2 hours of positioning (i.e., postures to stretch the muscles) a day for 5 days a week. Conventional rehabilitation focused on improving strength, joint alignment, range of motion, postural control, motor control, endurance capacity, and mobility skills. 22
The intervention group received the same rehabilitation as the control group, with an additional training using VR games (ICT4Rehab; see intervention). The additional VR training was given three times a week for 30 minutes under supervision of one of the three raters or a pediatric physiotherapist specialized in CP. Patients trained until discharge.
Patients were discharged from the hospital when (1) they were able to walk independently with a K-walker, (2) their required orthotics and braces were available, and (3) a physiotherapist at home continued their rehabilitation.
Outcome measures
The Trunk Control Measurement Scale (TCMS) was used to assess sitting balance. The TCMS is a valid and reliable tool to assess static and dynamic sitting balance and is specifically developed for CPc. 23 The subscale, static sitting balance, consists of five items (e.g., upright sitting and holding for 10 seconds, abduction of the leg over 10 cm). The subscale, dynamic sitting balance, consists of two parts: (1) selective movement control, which evaluates seven items (e.g., rotating the upper trunk with the head fixated in the starting position and shuffling the pelvis three times in a forward and backward direction), and (2) dynamic reaching, which evaluates three items (e.g., reaching forward and sideways). Every task is graded on a two-, three-, or four-point ordinal scale. The total score of the TCMS is 58 points, whereby a high score reflects good balance (Supplementary Data S2).
Inter-rater reliability of the TCMS was investigated first. Eleven children were scored by three raters. An intraclass correlation coefficient (ICC) of 0.98 and a confidence interval of 0.94–0.99 were found (Supplementary Data S3).
A Visual Analog Scale (VAS) was used to assess the children's enjoyment during rehabilitation (conventional rehabilitation and VR games separately). The scores ranged from zero (not amusing at all) to 10 (the most amusing ever experienced).
From start of training (sixth week after surgery), TCMS and VAS scores were evaluated every 3 weeks, at discharge, and follow-up.
Intervention
The VR games were developed as part of ICT4Rehab (see Table 2 for game characteristics). 24 Participants were seated on a Wii™ Balance Board (Nintendo®, Japan) and could move a target on the screen by moving the trunk (i.e., center of pressure [CoP]) in different directions. In the first game, rocks had to be avoided while flying an airplane. Participants had to make mediolateral CoP shifts to control the airplane. In the second game, boxes needed to be thrown from a shelf by mediolaterally targeting the cursor on the boxes. In the last game, the screen was covered with (virtual) dirt and needed to be cleaned by moving the CoP mediolaterally and anteroposteriorly, which revealed an underlying picture (Supplementary Data S4).
This information is based on published articles by the group that developed the games (ICT4Rehab; www.ict4rehab.org/), which led to the spin-off FeasyMotion (www.ict4rehab.org/FeasyMotion_Flyer_ScreenResolution.pdf). The game developers have developed the game based on desires from physiotherapists who work with children with cerebral palsy. The games have been used by these physiotherapists who provided feedback to the developers.
During the VR games, participants were instructed to sit upright on the balance board (with the legs unsupported) and keep the hands (relaxed) on the legs. Compensatory movements were avoided as much as possible by providing verbal instructions.
The trial protocol is presented in Supplementary Data S5.
Statistical analyses
Descriptive statistics (mean and standard deviation [SD]) were used in this pilot study. No inferential statistical tests (providing P values) should be used in pilot studies. 25
Results
Participants
Twelve participants were included. Due to cluster allocation, five participants were allocated to the intervention group and seven participants to the control group. One participant was excluded from the intervention group due to insufficient cooperation (Supplementary Data S1).
A hundred percent of the potentially suitable patients agreed to participate in the control group (they received standard care/conventional rehabilitation therapy). One of the five patients who were eligible for the intervention training was excluded due to insufficient cooperation, hence 80% of the eligible patients were recruited for the intervention.
Treatment and assessment adherence was 100% for all participants. All participants in the control and intervention groups participated in all treatment and assessment sessions.
Trunk Control Measurement Scale
Both the intervention and control groups improved their sitting balance (Fig. 1A). A higher increase in TCMS total score seemed apparent for the intervention group compared with the control group. The intervention group seemed to score better on all three subscales of the TCMS (not shown). From individual data points, it appeared that participants with a low baseline score improved more than participants with a high score at baseline (not shown). The presented results merely indicate a description of the means and SDs from the few included participants. A randomized controlled trial should be performed to be able to investigate the effectiveness of VR training and the differences between a matched intervention and control group.
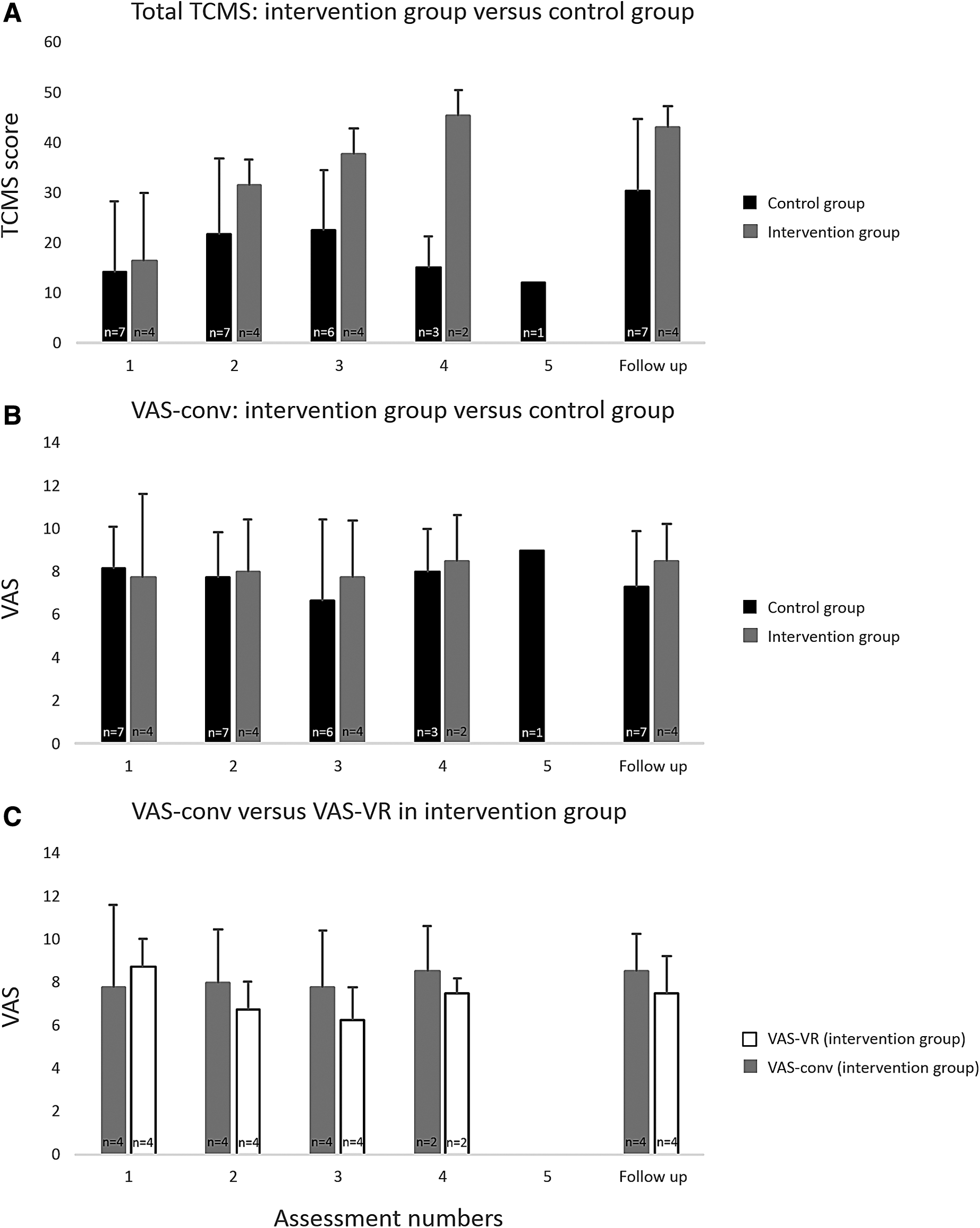
Means and standard deviations of the Total TCMS and VAS scores for the intervention and control groups. The interval period between the assessment numbers is 3 weeks. The interval period between the participant's last assessment after training and follow-up was a period of 6 weeks. Not every participant has the same number of time points since the rehabilitation period was dependent on evolution of the patient. Hence, the number of participants is provided in each bar graph.
Visual Analog Scale
VAS conventional rehabilitation (VAS-conv) intervention group versus control group
The results on VAS-conv did not seem to differ between both groups (Fig. 1B).
VAS-conv versus VAS VR games (VAS-VR) in the intervention group
The evolution in VAS-VR is negative during the time of rehabilitation (Fig. 1C). The mean of the VAS-VR games appeared lower than the mean VAS-conv in the intervention group (Fig. 1C).
Discussion
We found that applying a VR training paradigm additional to conventional physiotherapy in a rehabilitation center for CPc after lower limb surgery is feasible; 80% of the potential participants agreed to participate and 100% adhered to the training and assessments for the remainder of their rehabilitation program. The preliminary results seemed to indicate that implementing VR training in a rehabilitation center could be promising to improve balance in CPc. This should, however, be statistically examined with the upcoming RCT. Unexpectedly, the current VR training was not rated more enjoyable than conventional rehabilitation.
In the current study, we were able to demonstrate that VR games can be additionally used in a postoperative setting. No problems were reported involving patient recruitment. Only one participant who was eligible for the additional VR training was excluded. This was due to the fact that the patient had problems with listening to the therapists and, thus, did not cooperate. Most likely, this patient would have shown problems in the conventional therapy as well (given the cluster randomization, he was not in the control group of the current study). Furthermore, all patients in the intervention group showed an adherence of 100% to the additional VR training. This is quite remarkable given the already full schedule of patients in the hospital. No problems were reported in delivering the intervention, nor in implementing assessment measures.
The preliminary results for the combination of VR training with conventional physiotherapy appeared quite promising. This is consistent with the study by Sharan et al., 21 who indicated significant improvements in balance when VR gaming was added to rehabilitation after surgery, although it is unclear in their study which type of patients were included (e.g., which surgery was performed). Furthermore, it is possible that the balance improvements found in the study by Sharan et al. could have been a result of the ability to stand after the training period (and not necessarily due to improved sitting balance), as they used the PBS—a measure that includes standing balance tasks as well. Our study provides promising preliminary results to suggest that improvements in balance can also be due to a progression in sitting balance, irrespective of the ability to stand. It is of importance to further test this paradigm in a larger and homogeneous sample of CPc after lower limb surgery since there are some indications that appear to indicate that the combination of VR training and conventional physiotherapy can reduce the time of hospitalization and may increase the child's functionality (regarding trunk control) at discharge from the hospital. For instance, it appeared that at assessment number two, the intervention group achieved the same TCMS level as the control group at the follow-up measurement. An explanation could be that participants of the intervention group explored their boundaries of stability more during the rehabilitation period by playing the games. Participants of the control group only seemed to explore these boundaries when they were discharged from the hospital. Alternatively, it might be that while the VR games and the TCMS were developed completely independently, the required movements in the VR games were similar to some of the movements included in the TCMS; for example, the item of trunk shortening and lengthening (lengthening on the side of support, shortening on the other side) of the TCMS, which was also needed to reach the outer corner of the screen in the wipe out game. On the other hand, the intervention group did receive more therapy time than the control group. As such, it is possible that if the control group would have received the same amount of training in total, the results between the two groups could have been similar.
Overall, it appears that participants with a low baseline score improved more than participants with a higher baseline score (irrespective of training paradigm). However, three of these participants with a low baseline score did not improve as much as the others. These participants were diagnosed with quadriplegia, which could explain their slower improvements. The fact that three children with quadriplegia were in the control group and none in the intervention group was due to the cluster allocation method. Nevertheless, all participants showed a difference of more than six points on the TCMS between the follow-up and the first measurement. Since six points is the TCMS smallest detectable difference, 23 clinically relevant balance improvements have been made.
VR training paradigms are often applied to increase the motivation of the patient to train; therefore, we hypothesized that the children would perceive the VR games as more enjoyable than conventional rehabilitation. However, from the current results, it appears that the intervention group did not rate the games as more enjoyable than the conventional therapy. The VAS score on the games decreased somewhat over the rehabilitation time. This could be due to the fact that the games were not individually optimized as several children suggested some modifications, for instance; a dancing bear when they reached the next level and more age-specific photos in the wipe out game (e.g., boy bands, soccer players). Furthermore, some children did experience a lag between their trunk movements and the movement of the avatar on screen. As such, a future RCT should focus on optimizing the games individually to maximize each patient's motivation. This feasibility study was part of a master thesis project and, thus, its sample size is based on pragmatics such as patient flow and budgetary constraints (which is not unexpected in pilot work 25 ). Furthermore, the cluster randomization design was based on availability constraints of the VR games. At the start of the testing period, the VR games were not yet functional. Hence, we chose to allocate the patients during this period in the control group. As soon as the games were functional, patients were allocated to the intervention group. Therefore, in the future RCT, the training duration should be equal between the control and intervention groups to discern whether the increased therapy time or the specific balance-focused VR training yielded the better outcome for the current experimental group. In addition, the RCT should use individual randomization rather than cluster allocation to reduce the possibility of unbalanced control and intervention groups.
In conclusion, the current study showed the feasibility of applying a VR training paradigm in addition to conventional physiotherapy to train sitting balance in a rehabilitation center for CPc after lower limb surgery. The current results are of importance to improve the design of an upcoming RCT to examine the effectiveness of using individualized VR-based therapy additional to conventional rehabilitation in a postoperative setting to train balance in CPc after lower limb surgery.
Footnotes
Acknowledgments
This project (Clinical Trial Center s56332) was supported by a grant from the “bijzonder onderzoeksfonds” of the KU Leuven (grant nos. OT/08/034, PDMK/12/180) and the Research Foundation Flanders (FWO Vlaanderen) (grant nos. G.0901.11, “Krediet aan Navorsers” 1503915N). Pieter Meyns is a Marie Skłodowska-Curie research fellow (proposal 660458). Additionally, the authors thank the physical therapists of Department of CP at University Hospital Pellenberg for their aid during the measurements.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.