
Abstract
Abstract
Objective:
We compare physical activity during bouts of sedentary videogaming (SVG), active videogaming (AVG), and paced walking in children with and without autism spectrum disorder (ASD) to determine the effectiveness of AVG in providing moderate-to-vigorous physical activity.
Materials and Method:
Participants included nine males (8–11 years old) with ASD and eight age-matched males who were typically developing. Both groups had anthropometric and motor proficiency (Movement Assessment Battery for Children II) measures taken before testing. Participants attended three randomly assigned acquisition sessions: 20 minutes of paced walking at 4.5 metabolic equivalents, AVG, and SVG. Videogaming occurred on an Xbox® Kinect. An Actical accelerometer provided activity counts (AC) and percentage of time in moderate-to-vigorous physical activity (%MVPA). These were compared using 3 × 2 repeated measures analysis of variance for each measure.
Results:
Main effects for conditions existed for %MVPA (P < 0.0001) and AC (P < 0.0001). Post hoc Bonferroni comparisons indicated that AVG had significantly higher AC (P < 0.001) and % MVPA (P < 0.001) than SVG, but was significantly lower than paced walking (AC P < 0.001; %MVPA P < 0.01). Overall, participants spent 76.25% of their time in MVPA during AVG compared to 99.4% during paced walking and 2.31% in SVG. No main effects for groups or group by condition interaction effects were found for either measure.
Conclusions:
AVG may provide an appealing means by which all individuals can increase their overall physical activity levels, although AVG should not be seen as a replacement for walking or other forms of PA. Although further research is necessary, the finding that both groups performed similarly in AVG suggests that games can potentially be played without modifications or adaptations to gaming units, which may provide several advantages in terms of social/cost/ease of accessing unit.
Introduction
T
Given the known health benefits of routine physical activity (e.g., reduced cardiovascular disease risk factors, improved cardiorespiratory, musculoskeletal, metabolic health, and so on) 7 combined with the risks associated with sedentary behaviors (e.g., obesity, diabetes, and so on),8,9 it seems incumbent on those who live and work with children with ASD to determine effective ways in which these daily recommendations can be met. To date, however, the effectiveness of different types of exercise and physical activity has not been well established in this population. 10
Secondary motor impairment may account for some of difficulties children with ASD have in meeting physical activity recommendations.11,12 In addition, individuals with ASD often have a narrow set of interests in recreational activities.10,13 Furthermore, impairments in social communication skills can limit their ability to participate in peer play, team sports, and other group related activities that include physical activity.13–15 In addition, overt behaviors such as stereotypy, hyperactivity, and aggression can lead to decreased tolerance and acceptance in the community, school, and home, resulting in a severe restriction in overall involvement in community activities, peer and adult interactions, and typical education and concomitant socially mediated physical activity.16,17
Within the past 10 years, there has been an explosion in growth of the active videogame industry which may offer alternatives for increasing daily physical activity. Available units such as Nintendo®, Wii™, Xbox® Kinect, and Playstation (among others) are now relatively low cost and commonly used within the homes and community, creating access to a growing percentage of the general population, as well as those with ASD. Active videogaming (AVG) and the more immersive virtual reality have successfully been used in multiple areas of intervention (socialization, emotional recognition function activities of daily living, interactive play, verbalization, and communication) in individuals with ASD.18,19 Characteristics of AVG can engage players and overcome existing barriers in children with ASD. For many children with ASD, videogaming is a favored activity.20–23
This alone does not promote physical activity: children with ASD spend a larger amount of time engaging in sedentary videogaming (SVG) than their neurotypical peers. 22 However, this interest in videogames in general has the potential to be converted from sedentary to active with the use of appropriate games such as Xbox Active River Rush, where players must control a raft with their bodies as it moves downstream. Ideally, AVG would substitute for SVG, but would not replace other types of physical activity. 24 In addition, the multiple motivational qualities of AVG offered may supersede any dislike for physical activity. Many of the characteristics of AVG are motivating, which enhance effort and persistence put forth toward physical activity.25,26 Multiple research studies found positive relationships among enjoyment and performance during AVG.27,28 Motivational characteristics that support participation in AVG, including feeling of challenge, positive mood, autonomy, competence, and empowerment, are frequently lacking in repetitive exercises such as walking, stationary biking, and treadmill. 29
While using AVG is intuitively positive for increasing physical activity in ASD, evidence indicates that AVGs provide higher levels of energy expenditure or physical activity than SVG in both general and special populations.30,31 As expected, there is tremendous variability in exercise intensity depending on the different types of games and gaming systems. Within the different types of active videogames studied, most provide between light and moderate levels of activity, such as Nintendo Wii bowling, yoga, muscle conditioning, and skiing.32,33 Several provide exercise at moderate-to-vigorous levels, including Dance Central, Reflex Ridge, and Zumba.33–35 At present, the number of studies examining AVG specific to ASD is scarce, but many studies look at active videogame in populations with disabilities or health-related dysfunction such as the elderly, Down syndrome, cystic fibrosis, and cancer among others.36–38
Overall, studies concur that acute and chronic AVG promotes increased physical activity and positive health related outcomes. Likewise, the few studies on individuals with ASD indicate that AVG positively promotes physical activity31,39 and other positive outcomes such as the reduction of repetitive behaviors and improved cognitive function.19,40
The purpose of the current study was to compare a measure of physical activity (activity counts; AC) and of energy expenditure (percentage of time spent in moderate-to-vigorous activity; %MVPA) when children with and without ASD participated in 20 minute bouts of sedentary and active videogames, as well as paced walking. We predicted that AVG would show significantly higher values than SVG and similar values of these measures in paced walking in both groups. Based on previous research, we predicted that these measures would not differ between groups.
Methods
Overview
We compared the amount of moderate-to-vigorous physical activity expended during 20 minute sessions of SVG, AVG, and paced walking at 4.5 metabolic equivalents (METS) in a sample of 17 boys aged 8–11 years old with and without ASD. This study used an off the shelf Xbox Kinect 360 gaming unit using near-infrared technology to capture full body movements and provide movement feedback through an on-screen avatar. Brisk walking was chosen to support the difficulty with motor praxis experienced by children with ASD. Physical activity levels were compared using a repeated measures analysis of variance (ANOVA) with condition as the within-subject variable and group as the between-subjects variable. Before beginning this research, approval was obtained through the University of Delaware Internal Review Board to perform the study.
Participants
Participants with ASD were recruited from several school districts within the mid-Atlantic region of the United States specializing in or with specific programs for children with ASD. All children within these programs had a previous diagnosis of ASD from a clinical psychologist and/or physician. After administrative permission was granted, informational brochures were sent to students' parents with an invitation to participate. Initially, 11 male participants with ASD between the ages of 8–11 years had parental consent to participate. At the initial screening session, a series of measures were given to determine the eligibility for inclusion in the study.
Parents of the participants filled the Social Responsiveness Scale 2 (SRS 2) 41 to confirm diagnosis of ASD, with a cut score of 60 and above used to confirm ASD status (mean score: 72 ± 8.4). Next, the principal investigator administered a four-step instructional assessment to determine if the participants could understand and follow directions and engage in conversation. The Movement Assessment Battery for Children 2 (MABC-2) 42 was then administered to screen for severe motor competency issues (≤5th percentile) that may interfere with physical activity. Participants' weight and height were measured and used to calculate body mass index. All 11 participants met the inclusion criteria.
These participants were age matched with 11 participants without ASD or other physical or cognitive disability (typically developing; TD). TD participants were recruited through word of mouth and recruitment flyers posted in public places. All potential participants attended an initial screening session and were given the same set of tests as the ASD group. Parents of the participants filled the SRS 2 to rule out a diagnosis of ASD, with a cut score of 59 and below used to indicate an absence of ASD status. Movement Assessment Battery for Children 2 scores and heights and weights were taken. All 11 participants met the inclusion criteria. During the course of the study, three participants dropped out (two ASD: medication change, inability to attend testing sessions; TD: inability to attend testing session) and data from two TD participants were removed due to equipment failure, so that n = 9 for the ASD group and n = 8 for the TD group. The Table 1 summarizes participant demographic information.
Statistical significance.
ASD, autism spectrum disorder; BMI, body mass index; MABC 2, Movement Assessment Battery for Children 2; TD, typically developing.
Procedure
All testing procedures occurred in community settings that were familiar to the participants and throughout the school day, after school, or during summer activities. This environment was chosen over the laboratory to provide a comfortable environment for participants with ASD. Participants were tested in comparable areas where distractions were minimized and privacy maximized. Throughout the study, an Xbox 360 gaming unit and Kinect games (Microsoft, Redman, WA) were used on a 32-inch flat screen color television. This webcam system using near-infrared technology on top of the television requires the player to stand in front of the television by ∼5–8 ft.
All participants attended a total of four testing sessions. The first testing session was designed to introduce the participants to the equipment, Xbox Kinect games and testing protocol. During this session, participants were fitted with the Actical accelerometer (Philips Respironics, Bend, OR) and then sat for 20 minutes to obtain baseline sedentary information. Next, participants were familiarized with the videogames to be used in the study. During this time, the principal investigator showed them how to play each game and they were given opportunities to briefly try each game and ask questions. After confirming that the participants understood how to play each game, the testing session was terminated. During subsequent three sessions, participants performed all of the three activity conditions in a randomly selected order (one condition per session). On each day, participants were fitted with the Actical Accelerometer and provided instructions on the condition to be completed when they arrived at the testing session. This was followed by the activity condition, which lasted a total of 20 minutes.
Conditions
In the SVG condition, participants sat in front of the television at a comfortable distance and used a handheld controller to play “Bang Bang Racing,” a sedentary videogame requiring no movement besides the fingers of both hands. Participants repeated the game for the entire 20-minute session. In the AVG condition, two different games were played. The first game, “Crazy Sales,” requires players to control a security guard avatar using complex leg and arm movements while chasing rabbits through a virtual mall. Successful play requires multilimb coordination that resembles running and reaching. The second game, “Save the Hotdog,” also requires multilimb coordination. Players are represented onscreen by an avatar of a person in a hotdog suit who must stop a group of rabbits from eating a pile of hot dogs by moving arms and/or legs rapidly (reaching, kicking, and running movements).
The games were selected because they required full body movements and were fast-paced and had an on-screen avatar. The first game, “Save the Hotdog,” was played twice then the second game, “Crazy Sales,” was played twice; this pattern was repeated for the 20-minute period. In the paced walking condition, a walking area was used with two-taped sections with 50 and 100 ft increments for increased pace accuracy. The researcher paced the participant at 4.5 METS using a stopwatch. Data were collected during the entire session. For all conditions, minutes 4–19 were used for analysis for a total of 15 minutes.
Equipment and measures
We used an Actical (Philips Respironics, Inc., Bend, OR), a monitor that houses an omnidirectional accelerometer that senses movement in all directional planes which has been validated for use in children43,44 and used previously in research with children with ASD31,39 to capture data related to participants' physical activity. The accelerometer detects low-frequency G-forces (0.5–3 Hz) common to human movement and generates an analog voltage signal in 15 second epochs that is filtered and amplified before being digitized by a converter at 32 Hz. We used these digitized values, which indicated that the overall number of body movements made are AC, as our measure of physical activity. Actical software also provided the percentage of time spent in moderate-to-vigorous physical activity (%MVPA) using previously defined cut scores for children. 43
Analysis
Data were analyzed using a repeated measure ANOVA with condition as the within-subject variable and group as the between-subjects variable for both AC and %MVPA. The Greenhouse–Geisser correction was used to adjust for degrees of freedom where the assumption of sphericity was violated. Partial eta squared (η2p) values were calculated for significant main effects. Bonferroni post hoc tests were used to adjust for multiple comparisons. IBM SPSS Statistics for Windows (2012; Version 21.0. Armonk, NY: IBM Corp.) was used for statistical analysis.
Results
Percent time spent in moderate-to-vigorous physical activity. For %MVPA, Mauchley's test indicated that the assumption of sphericity was violated χ2 (5) = 20.760, P < 0.001; a Greenhouse–Geisser correction was used to correct degrees of freedom e = 0.57. There was no main effect of group on %MVPA (F(1, 15) = 1.30, P = 0.273), indicating that no significant differences existed between the groups in percent time spent in MVPA. There was a significant main effect of condition (F(1.690, 25.45) = 1369.08, P < 0.00001; η2p = 0.98, indicating a large effect size). Bonferroni post hoc comparisons indicated that walking was significantly greater than AVG (P < 0.001) and SVG (P < 0.0001), and AVG was significantly greater than SVG (P < 0.0001). These results are reported in Figure 1.
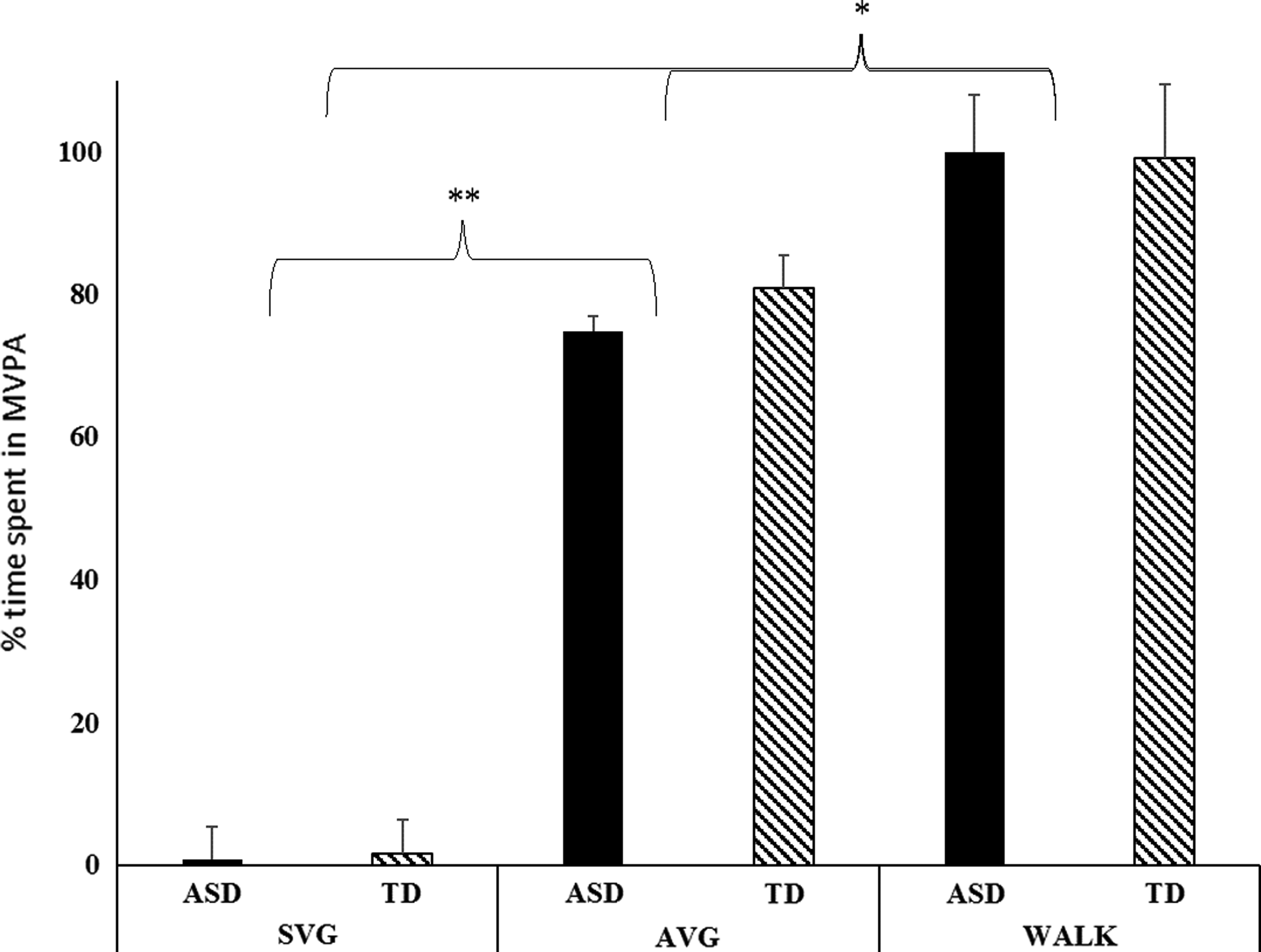
Percent time spent in moderate-to-vigorous physical activity in SVG, AVG, and paced walking during activity bouts. *Significance at P < 0.001; **Significance at P < 0.0001. AVG, active videogaming; SVG, sedentary videogaming.
Activity counts
Mauchley's test indicated that the assumption of sphericity was violated χ2(2) = 6.78, P = 0.034, and the degrees of freedom were corrected with Greenhouse–Geisser correction ɛ = 0.72. No significant main effect existed for group in AC (P = 0.107). A significant main effect existed for condition (F(1.45, 21.68) = 91.63, P < 0.001; η2p = 0.86, indicating a large effect size). Bonferroni post hoc comparisons indicated that SVG had significantly fewer AC than AVG (P < 0.001) and walking (P < 0.001). AVG had significantly fewer AC than walking (P < 0.05). The results are presented in Figure 2.

Total number of activity counts in SVG, AVG, and paced walking during activity bouts. *Significance at P < 0.005; **Significance at P < 0.001.
Discussion
We hypothesized that group differences would not exist on either measure, and this prediction was upheld. There were no significant between-subjects main effects on either measure indicating that participants with and without ASD performed the activities at similar percentages of moderate-to-vigorous physical activity and AC. This supports our previous findings that suggest that individuals with ASD can achieve MVPA intensities that are similar to individuals without ASD when using Nintendo Wii games, 31 as well as other studies, indicating children with and without ASD are similar in terms of their physical activity expenditure. 4 These results are promising as they suggest that individuals with mild-to-moderate ASD may not require adaptations to play Xbox Kinect active videogames although further research with a larger sample size should be performed to confirm this. Off the shelf game use would defray costs and minimize need for outside supports, which in turn decrease potential barriers that often deter performance of physical activity.
We also hypothesized that both physical activity and energy expenditure would be greater in AVG than SVG and this hypothesis was also upheld. Prior research has shown that participation in videogaming by individuals with ASD, in general, helps to contribute to an inactive lifestyle.21,22 The fact that the AVG condition resulted in higher activity levels than SVG, while not surprising, provides a potential alternative to the increase in sedentary behaviors resulting from too much screen time. Studies of other populations consistently find that AVG has higher physical activity levels compared to SVG.27,32–34 Given the popularity of videogaming among individuals with ASD, 10 an intervention that takes advantage of this interest will be more likely to have a higher probability of success over time than other types of repetitive activities.
At the same time, our hypothesis that AVG and paced walking would not differ in AC or %MVPA was not upheld. Paced walking provided the highest AC and percent time in moderate-to-vigorous physical activity in comparison to the two videogame conditions. This was contrary to the prediction that the three-dimensional feedback of the infrared sensor technology of the Kinect unit and rapid full-body movement promotion of the game would lead to similar intensity levels as paced walking. Given that walking can occur virtually anywhere with no special equipment and AVG necessitates the use of a gaming system hooked to a television or monitor which may or may not be dedicated to videogame use, it seems prudent to consider AVG as complementary to rather than a replacement for alternative forms of physical activity such as walking or running.
The most functionally relevant finding is that AVG provided physical activity at levels high enough to contribute to the daily recommendations of the CDC for individuals with disabilities, which states that those with disabilities should strive to adhere to short spurts of a variety of enjoyable and age appropriate activities that reach MVPA adding up to the 60 minutes per day.1,47 The data collected during AVG met these requirements as MVPA intensity levels for sustained durations in both groups. In addition, the AC per minute exceeded the 1500 cut point for moderate levels established by Puyau et al. 43 While using Kinect, time spent in moderate-to-vigorous intensity was 76% in those with ASD and 80% in those without ASD, which equals 10–11 minutes out of 15 minutes. These durations of MVPA are similar to the published periods expressed as an appropriate activity for this age group. These findings were similar to other studies on select videogames and videogame units both in adults and children.27,46–49
Limitations and future directions
The number of participants within the study may have limited our ability to detect differences between groups or group by condition interactions. Both time and geographical restrictions limited the pool of participants with ASD who fit inclusion/exclusion criteria. We also did not have a homogeneous sample of children with ASD (e.g., all classified the same), which may have led to an increase in variability in our measures. However, there is a great degree of interindividual variability within children with ASD who share a classification, so it is unclear of the impact limiting participants would be. Finally, this study was designed to examine physical activity during single activity sessions. Because participants performed each condition for one 20-minute bout only, we cannot speculate on the efficacy of using AVG for longer exercise bouts or repeated over the course of weeks, months, or years (e.g., as a regular part of a physical activity routine).
In the future, we would like to repeat this research with a greater number of participants several times a week over the course of several months to better align with the CDC recommendations. At the same time, we find the results promising in suggesting AVG are activities that could be an alternative physical activity contributor to meet recommended levels. In the natural setting, use of these AVG may meet both groups' needs and be used to facilitate group play. Group activities promote socialization and development of communication skills, and as such, the use of AVG could potentially become a mechanism to facilitate social growth and reduce social stigmatization in the ASD population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.