
Abstract
Abstract
Background:
Exergaming is potentially useful to promote physical activity in children; however, long-term effectiveness is unclear. MobileKids Monster Manor (MKMM) is a mobile exergame developed with the help of young advisors. The game wirelessly transmits physical activity data from an accelerometer to a mobile device. Players' steps are redeemed for in-game rewards, for example, new characters.
Objective:
First, to evaluate whether increased physical activity previously observed in a 1-week intervention is sustained over a 2-week intervention and 1-week follow-up, and second, to compare impact in schools within different socioeconomic environments.
Methods:
Thirty-seven elementary school students participated in a 4-week randomized controlled study (1-week baseline; 2-week intervention [with only the Game group receiving MKMM]; and 1-week follow-up). All participants wore a Tractivity® accelerometer throughout. Linear mixed models were applied to assess sustainability; a second 42-children-based dataset and age-/sex-adjusted linear regression models were used to compare effect across socioeconomic environments.
Results:
In the first week of intervention, the Game group compared to the Control group showed a greater increase in physical activity (of 1,758 steps/day [95% confidence interval, CI = 133–3,385] and 31 active minutes/day [95% CI = 4–59]), relative to baseline (13,986 steps/day; 231 active minutes/day). However, this was not sustained in the second intervention week or follow-up. The school within a lower socioeconomic status environment showed lower baseline activity and the 1-week intervention resulted in a greater increase relative to baseline (3,633 steps/day more [95% CI = 1,281–5,985]).
Conclusion:
MKMM could be a useful short-term physical activity promotion tool; however, effectiveness may decrease as novelty diminishes.
Background
P
Active videogames, or exergames, provide an alternative means of promoting activity by using videogame play as a motivator for exercise. 7 Exergaming has shown promise in promoting physical activity. 8 Mobile exergaming is an emerging form of exergaming using a mobile device, instead of a computer. The most popular mobile exergames are location based, detecting the player's current location and mapping it to the character in the virtual game world. The huge potential of a mobile exergame to increase physical activity was clearly demonstrated by the success of Pokémon GO.9–11 However, little research exists regarding the effectiveness of mobile exergames in increasing physical activity, 12 especially in school-based environments. Evidence to date is mixed; location-based games like Woody successfully increased outdoor physical activity, 13 but Fitquest yielded inconclusive results. 14
Mobile exergaming allows participants to be outside and can provide tailored feedback at appropriate times and places when more likely to affect behavior change. 15 Access to active play in nature and outdoors is essential for healthy child development. 4 Thus, we have developed a mobile exergame, MobileKids Monster Manor (MKMM), which allows children to play outdoors. 16 Most mobile exergames use the smartphone's in-built GPS and/or accelerometer to track physical activity, whereas MKMM is synchronized with an external activity monitor, allowing physical activity tracking without carrying the phone. MKMM leverages the wide appeal of games and technology to children, to improve their physical activity levels. To ensure the theme and graphics would be visually and conceptually attractive to children, MKMM was developed with direct involvement from KidsCan, a youth advisory group. 17 MKMM was previously validated in a community-based environment 16 and a school-based setting, 18 and in both cases, the game successfully increased short-term voluntary physical activity among children. The results of both 1-week intervention studies demonstrated the potential of this tool; however, they did not examine sustained effect. Accordingly, this study's goal was to assess the sustainability of our mobile exergame over a longer intervention period, and beyond cessation of the intervention. Although the application had no specific features designed to engender long-term behavior change, we anticipated it might nevertheless build habits that persist over time. We chose to evaluate the sustainability of MKMM in an urban elementary school because, relative to a community-based study, a controlled educational setting provides a consistent routine and facilitates monitoring of the participants. Our primary hypothesis was that MKMM would increase physical activity among children during each of 2 intervention weeks, and this increase would be maintained during a 1-week follow-up.
In addition, as a second part of the study, we also evaluated the differences in applying the MKMM intervention to two urban elementary schools within differing socioeconomic environments. For this comparison, data from a previously developed study were also used. 18 Our secondary hypothesis was that the baseline physical activity would be higher in the school with a higher socioeconomic status and thus the game might have a lessened impact.
Methods
MobileKids Monster Manor
The mobile-based exergame was developed by Ayogo Health, Inc. (Vancouver, Canada) to wirelessly connect with the Tractivity® activity monitor (Kineteks Corporation, Vancouver, Canada). Tractivity is a triaxial accelerometer-based wearable device that measures steps and active minutes in 1-minute epochs. 19 It has been previously validated in several studies20,21 and is suitable for measuring indoor and outdoor activity and, while not waterproof, can tolerate sweat and rain.
The game was developed with direct involvement of our KidsCan youth advisory group (http://bcchr.ca/kidscan), an initiative involving youth as ambassadors for research related to their demographics. Our young advisors participated from the earliest stages to improve the gaming mechanism and the accompanying visual design. Their insight ensured that the game would be attractive to children, a factor of paramount concern when designing for children. 17
The MKMM game uses a monster character theme. Physical activity is required to progress within the game. Players' steps are redeemed for rewards such as in-game items and the unlocking of new characters. MKMM leverages behavioral psychology in the form of positive peer pressure. Players are assigned to three teams and team members work together to achieve a higher total score. The game allows players within teams to encourage and congratulate their teammates' efforts using preset messages. Players completing physical activity challenges add to their teams' total score, in addition to unlocking items and characters for themselves (see Garde et al. 16 for a detailed description of the game). Physical activity is measured using the Tractivity activity monitor. The game wirelessly connects to the activity monitor periodically rather than requiring a constant connection, freeing the player from the requirement to carry the mobile device while being active.
Study population
This study was undertaken at an elementary school located in the Shaughnessy neighborhood of Vancouver, Canada. With permission from the Vancouver School Board and the school's teachers, and in accordance with a protocol approved by the University of British Columbia and Children's and Women's Health Centre of British Columbia Research Ethics Board (H15-00642), we recruited two split-grade classes of students (grades 4–5) to participate in the study. Cooperation and assistance from the teachers were instrumental to the study's successful completion.
Parents gave written informed consent for their children to participate. Each child also supplied written assent after the purpose and design of the study were explained to them using language appropriate for their age and grade level. Children with a medical history of respiratory, cardiovascular, or neurological issues were excluded from participation.
Study protocol and randomization
A randomized controlled study was performed over 1 month (May 19th to June 22nd, 2015) in three distinct phases: 1-week baseline physical activity assessment, 2-week intervention, and 1-week follow-up (Fig. 1). We randomly assigned children to one of two study arms: Game group and Control group. All participating children received the activity monitor in a convenient velcro strap that fastened securely around the ankle. Children were required to wear it continuously (except when sleeping, bathing, and swimming). During the intervention phase, only children in the Game group received MKMM, preinstalled on a Wi-Fi enabled iPod touch, and were allowed to use it at their convenience.
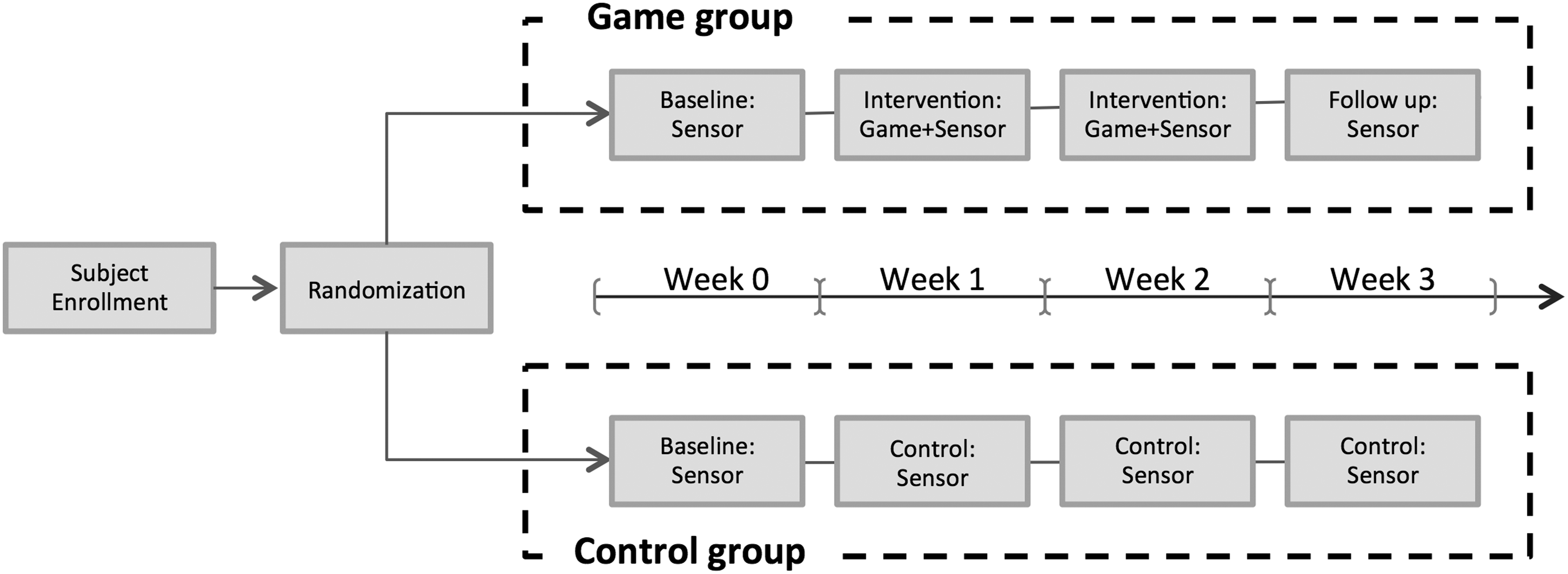
The randomized controlled testing protocol over the study period.
The activity monitors' serial identification numbers were used to randomize the participants into two study arms. Each monitor's serial identification number was assigned to either Game or Control group, matching the number of enrolled children. A research assistant, blinded to the randomization, concealed the serial identification numbers in opaque envelopes, in randomized blocks of four. The randomization was performed separately for each class.
Data collection
We recorded each participant's sex and age, and measured weight and height using a Sunbeam digital scale (Model SDR520CO-01) and a metric ruler, respectively. We calculated body mass index (BMI) from weight and height. The results were standardized using the WHO child growth standards, 22 converting to BMI z-scores that incorporate participant age and sex.
Each participant's physical activity, in steps and active minutes, was collected by the activity monitor for the study's duration. Tractivity software defines an active minute as a minute containing at least 20 steps, and within a window of 7 active minutes.
Participants in the Control group were also able to play the game once the study was completed. Thus, all participants were asked to complete the Game Response Survey 16 to assess their experience wearing the activity sensor, playing the MKMM game, and using the social aspects of gameplay. This survey consisted of eight close-ended questions 23 about players' attitudes toward the activity monitor, the game, the social encouragement within the gameplay, and if the game encouraged more physical activity overall, and one open-ended question for general comments.
Second study population for comparison
The data of a previously conducted (May 14th to June 18th, 2014) study at an elementary school located in the Kensington-Cedar Cottage neighborhood of Vancouver, BC, were also studied to assess the MKMM intervention in schools located within differing socioeconomic environments. Students from two classes (split classes of grades 4–5 and grades 6–7, ages from 9 to 13 years) were recruited according to a protocol approved by the University of British Columbia and Children's and Women's Health Centre of British Columbia Research Ethics Board (H13-03551). In this study, we applied a randomized controlled crossover study design to assess the effect of 1-week duration game intervention. 18
Data analysis
The primary hypothesis regarding the game's impact during and after the intervention was evaluated using a linear mixed models approach with group as factor, and week as covariate. Differences in physical activity relative to baseline (average steps/day and active minutes/day within each week), between both groups (Game and Control), and across weeks (intervention and follow-up), as well as group × week interaction term were studied. As recommended by adolescent physical activity guidelines, 24 a period of 60 consecutive minutes with zero steps was considered “non-wear time”. Only days with over 10 hours of “wear time” were included in analyses, and a minimum of 3 “wear days” per week were required to estimate the average number of steps and active minutes per day within each study week. For each participant, the baseline week's activity level served as a reference for all subsequent analyses.
To evaluate the secondary hypothesis, data collected as part of a similarly designed, but 1-week intervention study performed at the elementary school located in the Kensington-Cedar Cottage neighborhood of Vancouver, 18 was compared to that of this study, performed at the elementary school located in the Shaughnessy neighborhood of Vancouver. The Vancouver communities that these schools are located in and serve differ in socioeconomic status. According to the 2011 National Household Survey, the Kensington-Cedar Cottage neighborhood has an average family income of 80,386 CAD, which is equal to 60% of the average family income estimated in the Shaughnessy neighborhood (121,048 CAD). 25 It should be considered that Vancouver has an average family income (99,723 CAD), much higher than the national average (79,102 CAD). 25 A two-way t-test was applied to investigate differences in the baseline physical activity and the impact of the game during the 1-week intervention, in terms of average steps/day and active minutes/day relative to baseline. In addition, a linear regression model was applied to adjust for confounding factors such as age and sex. A probability of P < 0.05 was considered significant. All analyses were performed using IBM SPSS Statistics version 19 software.
Results
Demographics and baseline activity
We recruited 42 children (23 female and 19 male), 10.6 ± 0.51 years old, with BMI z-scores of 0.21 ± 1.0. A two-way t-test showed no significant difference between the Game and Control groups' demographic features and baseline physical activity (Table 1). According to WHO growth curves, 14% of the recruited participants were classified as overweight and 7% as obese. One participant withdrew from the study due to illness and four did not meet the minimum “wear-time” criteria across the entire study. Thus, the physical activity of 37 participants out of the 42-participant cohort was studied. Participants presented a baseline physical activity of 13,975 ± 3,187 steps/day and 230 ± 46 active minutes/day.
The BMI z-score is a measure of relative weight adjusted for age and sex. It was calculated based on WHO guidelines using the weight, height, and age values for each participant. No significant differences (through two-way t-test) were found between Game and Control demographic features and baseline physical activity values.
Three participants from the Game group and two from Control group were excluded from the analysis (one participant got sick and four did not meet the “wear time” criteria).
BMI, body mass index.
Multi-week physical activity evaluation
The effect of the game, relative to baseline activity, was assessed between groups and weeks (first and second week of intervention and follow-up), through linear mixed models, and showed statistically significant differences between groups. The group effect (Table 2) indicated that during the first week of intervention, the Game group averaged 1,758 more steps/day and 31.3 more active minutes/day relative to their baseline than the Control group. Regarding the time effect, both Game and Control groups, showed no significant temporal patterns in the variation of physical activity level across study weeks. The group × week interaction term was also not significant, showing that the Game group did not exhibit a different physical activity progression pattern compared to the Control group.
Weeks 1, 2, and 3 were recoded to 0, 1, and 2, respectively, for the linear mixed model analysis, in IBM SPSS Statistics.
CI, confidence interval; SE, standard error. Significant values are represented in bold.
These results show that MKMM successfully increased physical activity during the first intervention week, but this activity boost was not maintained during the second intervention week and follow-up (Fig. 2).
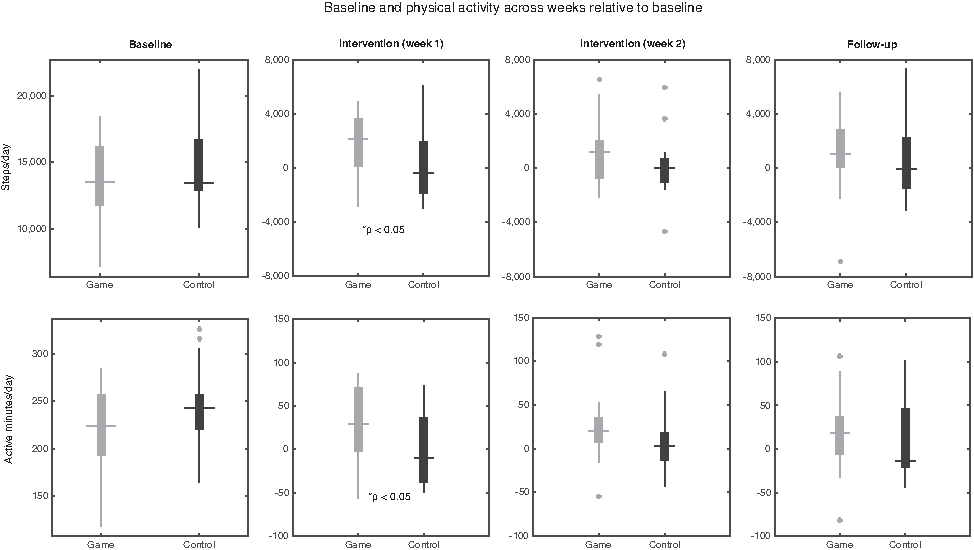
Boxplot for both groups (Game and Control) of steps/day (top row) and active minutes/day (bottom row) during (left to right) baseline week and during the first intervention, second intervention, and follow-up weeks relative to baseline. Quartile values are displayed with boxes and horizontal lines. Cross markers represent the most extreme values within 1.5 times the interquartile range from the median. As illustrated, during the first week of the intervention, the Game group showed a significantly greater increase in physical activity (in both steps/day and active minutes/day), than the Control group.
Comparison of physical activity and exergame impact in two different socioeconomic school environments
Children at the Shaughnessy neighborhood elementary school were significantly more physically active than children of the same sex and similar age at the Kensington-Cedar Cottage neighborhood school, where 42 children had been previously recruited: 20 in Game group (7 female and 13 male) and 22 in the Control group (9 female and 13 male). The children at Shaughnessy exhibited 1,557 more steps and 36 more active minutes per day (Fig. 3a, c and Table 3). Children at each school reported similar satisfaction with the game and activity sensor through the Game Response Survey (over 90% of the participants reported liking the game, the sensor, and having to be active). 16 However, the 1-week intervention resulted in a significantly greater increase in physical activity (3,633 steps/day and 64 active minutes/day more relative to their baseline) among children in the Kensington-Cedar Cottage neighborhood compared to children of the same sex and similar age in the Shaughnessy neighborhood (Fig. 3b, d and Table 3). With this 1-week intervention, students of the Shaughnessy and Kensington-Cedar Cottage neighborhoods reached, on average, activity levels of 15,693 and 14,831 steps/day, respectively (meeting the recommended daily minimum of 13,500 steps/day 26 ).

Boxplots of physical activity during the baseline week (left boxplots) and physical activity relative to baseline during the game intervention week (right boxplots), for students at the elementary schools in the neighborhoods of Shaughnessy and Kensington-Cedar Cottage in Vancouver, Canada. Physical activity is represented in terms of steps/day (top row) and active minutes/day (bottom row). Quartile values are displayed with boxes and horizontal lines. Cross markers represent the most extreme values within 1.5 times the interquartile range from the median.
The mean difference between the baseline and relative steps/day and active minutes/day, P-value, and 95% CIs evaluated through a two-way t-test are represented. Also represented are adjusted values, obtained with a linear regression model adjusted for age and sex (common confounding factors when evaluating physical activity).
Discussion
Our MKMM game intervention increased voluntary physical activity relative to baseline during the first week, as demonstrated by the significant difference in activity levels between Game and Control groups during this period. However, no difference was found between the Game and Control groups in the intervention week two and follow-up week. The majority of children reported liking the game (92%) and finding the activity monitor easy to wear (94%). However, in an open-ended response, some children reported a decrease in motivation once all game components were unlocked and no new elements were left, which may correlate with the game's decreased effect over the second intervention week. New game elements or challenges introduced into MKMM may improve the sustainability of its effectiveness.
When comparing data from our two studies at schools within different socioeconomic environments, there were differences between the cohorts in baseline physical activity and effect size of the game intervention. Children attending the Kensington-Cedar Cottage neighborhood elementary school had lower baseline activity levels than children in the Shaughnessy neighborhood. The relationship between socioeconomic status and healthy behaviors in children has been widely studied, showing a clear relationship between lower socioeconomic status and lower levels of physical activity.27,28 This relationship also appears to correlate with lower levels of participation in organized sports and fewer safe areas for outdoor play in neighborhoods with lower socioeconomic status. 27 These factors may explain, in part, why, at baseline, school children in the Kensington-Cedar Cottage neighborhood had on average 1,557 less steps and 36 less active minutes per day than school children in the Shaughnessy neighborhood.
Notably, we found that the 1-week mobile exergame intervention could reduce disparities in physical activity between varying socioeconomic environments. There was a significantly greater increase among children at the school in the neighborhood with lower socioeconomic status, where 63% of children were found to not meet the minimum physical activity recommendations. 26 The 1-week intervention brought these students to an activity level (14,831 steps/day) similar to that of students of the Shaughnessy neighborhood, during their respective intervention week (15,693 steps/day). A major limitation of this comparison is that, although both studies followed the same 1-week intervention, the study in the Kensington-Cedar Cottage neighborhood was performed from May to June 2014 and the study in the Shaughnessy neighborhood from May to June 2015. We are thus unable to remove confounders such as year-to-year variability of factors, including weather and the economy.
Exergaming is a novel and exciting strategy to increase physical activity among youth,7,29 including high-risk groups such as lower socioeconomic status. 30 However, it is difficult to compare outcomes between studies, as each applies different exergames and interventions. While some exergame interventions have increased the physical activity levels and energy expenditure of players,31,32 there are also inconclusive results on the performance and sustainability of exergames.8,33,34
With respect to the validation of MKMM, in our two previous studies, we tested the game in a community-based environment 16 and in a school-based environment. 18 MKMM was more effective in a school environment (increase of 2,934 steps/day [95% confidence interval, CI = 1,434–4,434] from baseline) than in the community environment (increase of 1,747 steps/day [95% CI = 153–3,342] from baseline). Unlike the community setting, the school setting allowed for daily interaction and healthy competition among known peers, increasing the motivating effect of the game. This effect may be associated with the demonstrated increase in compliance and game scores in the school setting. Within both environments, the increased physical activity observed with MKMM meant that more students (in total, 68% of the Kensington-Cedar Cottage neighborhood and 80% of the Shaughnessy neighborhood) met the minimum daily physical activity recommendations. In this study, focused on evaluating the effect of MKMM during and after a longer intervention period, the results confirmed that the game can promote physical activity in children, but that this effect may not be sustainable.
A major limitation of the game is that it was designed to be a short-term intervention. By exhibiting high levels of physical activity, children can unlock all monster characters and in-game rewards in only a week's time. When this happens, the player gains a level and starts the same game over again, while maintaining their accumulated score. There are no novel elements beyond completion of the first level, which correlates with the decrease in physical activity during the second week of intervention. It is likely that, to maintain motivation and the impact of the game, it must be designed to remain novel for the duration of the intervention. Another limitation of the study is the possible contamination effect of having children in the Game and Control group in the same class.
Although MKMM was not designed to act as an educational tool, exergames have this potential and may positively influence young peoples' knowledge, skills, attitudes, and behaviors in relation to health and physical exercise. 35 Less than 10% of the Canadian population is aware of the physical activity guidelines 36 ; next iterations of MKMM could provide this information or otherwise educate the user. Considering that physical activity habits that begin in childhood follow into adulthood, 37 knowledge imparted on our target population would have a valuable long-term impact.
The MKMM exergame is an innovative and exciting way of promoting physical activity in children in both school and community-based environments. However, the impact of this mobile exergame, an increase in physical activity, does not appear to be sustainable given the current iteration of the game. To sustain activity increases, we could investigate the effect of the game introducing an educational component (designed to increase comfort with physical activity or knowledge of its benefits). In addition, baseline physical activity and impact of the game may vary depending on the socioeconomic status of the families, among other factors. 15 MKMM may help promote physical activity in areas of economic disadvantage.
Footnotes
Acknowledgments
The authors would like to thank Ayogo Games, Inc. and Kineteks Corporation for their collaboration, Guohai Zhou for his advice regarding statistical analyses, and staff and students from both schools. The authors would also like to especially thank Gabrielle Chan and Sandra Yee for their vital support, the members of the Pediatric Anesthesia Research Team at the BC Children's Hospital, and KidsCan advisors. This research was funded by a grant from the Peter Wall Institute for Advanced Studies under the Peter Wall Solutions Initiative program and the Michael Smith Foundation for Health Research. The game developer, Ayogo Games, Inc., was paid as a contractor using funds from the Peter Wall Institute for Advanced Studies.
Author Disclosure Statement
No competing financial interests exist.