
Abstract
Abstract
Objective:
An acute bout of moderate-to-vigorous exercise temporarily reduces pain sensitivity in healthy adults. Recently, active gaming has been rising in popularity as a means of light-to-moderate exercise and may be particularly suitable for deconditioned individuals. Whether the physical activity elicited in active games can produce a hypoalgesic effect remains unknown. The purpose of this study was to determine whether active videogames can reduce pressure and heat pain sensitivity in healthy adults. We also evaluated the relationship between the physical activity elicited by the games and the magnitude of the hypoalgesic response.
Materials and Methods:
Twenty-one healthy adults played four different active games on separate days, including Microsoft® Kinect Xbox® One's Fighter Within and Sports Rival's Tennis, and Nintendo® Wii™ Sports' Boxing and Tennis. Heat pain thresholds on the forearm and pressure pain thresholds (PPTs) on the trapezius and forearm were assessed immediately before and after a 15-minute active gaming or control session. Minutes spent in sedentary time and moderate-to-vigorous physical activity (MVPA) during active gaming were measured with an accelerometer.
Results:
The analyses revealed that PPTs at the forearm and trapezius significantly increased from pretest to posttest following Kinect Fighter Within. PPTs at the trapezius also significantly increased from pretest to posttest following Wii Boxing. The magnitude of the hypoalgesic response was significantly correlated with MVPA and sedentary time during gameplay.
Conclusion:
These results suggest that an active gaming session played at a moderate intensity is capable of temporarily reducing pain sensitivity.
Introduction
E
In the past decade, active gaming has emerged as an alternative mode of physical activity that can elicit a light-to-moderate level of physical activity while also providing entertainment.3–5 Active games, or exergaming, are videogames that elicit movement from the user. Some games utilize motion tracking technology to track the movement of the participant and allow the participant to interact with the game with movement of his or her body. Other active games use sensors that react to motion of the remote control. This type of exercise might be particularly suitable for deconditioned individuals because gameplay can either be intensified or decreased in real-time by the participant. Games also provide built-in breaks during level or opponent transitions, creating a rest time for the participant. These breaks further ensure that the gameplay is not too strenuous for the participant. However, whether active gaming can produce a sufficient level of physical activity to reduce pain sensitivity and potentially be a pain management tool remains unknown.
The primary purpose of this study was to determine whether active videogames produce a hypoalgesic effect and reduce pressure and heat pain sensitivity in healthy adults compared with a control condition. Past research indicates that the movement elicited by active games varies widely between games.6,7 Thus, we tested four different active videogames from two different gaming systems, including the Nintendo® Wii™ (an older and more widely used gaming system) and the Microsoft® Kinect Xbox® One (a newer system with updated technology). Active videogames that cause more movement stimulate greater energy expenditure, with specifically hip movement being the best predictor of these responses.6,7 Therefore, this study also assessed the level of whole-body sedentary time, light physical activity, and moderate-to-vigorous physical activity (MVPA) with an accelerometer worn on the hip. The secondary purpose was to determine the relationship between the physical activity behavior elicited by the games and the magnitude of the hypoalgesic response.
Materials and Methods
Participants
Twenty-one healthy adults (7 males; age range 18–32 years old; average age = 22.8 ± 4.5 years) completed this study. All participants were recruited from the university campus, right-handed, and had an average body mass index of 25.7 ± 4.8 (range 19.5–35.9). During the first visit, participants were screened with the Physical Activity Readiness Questionnaire (PAR-Q) for any potential health conditions that would prohibit them from participating in physical activity. 8 Participants were also instructed to refrain from smoking, or consuming alcohol or caffeine 24 hours before testing, refrain from strenuous exercise >12 hours before testing, and fast 1 hour before each experimental session. Participants also reported no ongoing pain conditions and no medications on days of testing before the testing sessions. Participants completed one screening/control session and four experimental sessions. The data reported in this study, whereas not published elsewhere, are part of a larger study examining the energy cost of active gaming. A power analysis, using G Power 3.1.5., was used to estimate the sample size needed for detecting a significant change in pain outcome measures from the pretest (before active gaming) to the posttest (immediately after active gaming session). With a significance level of 0.05, power at 0.80, a 0.5 correlation among repeated measures, the power analysis indicated that a minimum sample size of 21 subjects was needed to detect an effect size of 0.40 (moderate effect).
Screening/control session
All participants reviewed and signed an Informed Consent Form approved by the Institutional Review Board of Indiana University. Those individuals who sign the Informed Consent Form completed the PAR-Q and height and weight measurements. Participants were then familiarized with the pain assessments and then completed the control condition pain assessments. For the familiarization of the pain tests, participants received detailed instructions for each test and then completed three practice trials for the pressure pain thresholds (PPTs) and three practice trials for the heat pain thresholds (HPTs) on the right dorsal forearm. After a 10-minute rest period, the control condition pain assessments began. Specifically, pressure and HPTs (described in Pain assessments section) were assessed before and after 15 minutes of quiet rest. Lastly, participants were familiarized with the active game systems and played each active game for 10 minutes.
Experimental sessions
All participants completed all of the experimental sessions. The order of the experimental sessions was randomized and took place on separate days. During each experimental session, participants played only one of the following games: Nintendo Wii Sports Boxing (Wii Boxing), Nintendo Wii Sports Tennis (Wii Tennis), Microsoft Xbox One Kinect's Sports Rival's Tennis (Kinect Tennis), or Microsoft Xbox One Kinect's Fighter Within (Kinect Fighter Within). A description of these games is listed in Table 1. Each game was played for two 15-minute periods with a 15-minute rest interval between each period. During period 1, participants were instructed to play at a self-selected intensity. Past research has shown that when participants play active games at a self-selected intensity, the amount of movement during games can vary widely between participants. 5 Thus, during period 2, participants were instructed to try to maximize movement during gameplay. To avoid the effects of multiple repeated pain testing, the HPTs and PPTs were only taken immediately before and after one period of gameplay during each session. Specifically, the pain assessments were taken pre- and postperiod 1 (self-selected intensity) for Wii Tennis and Kinect Tennis, and pre (i.e., immediately before period 2) and postperiod 2 (maximize movement) for Kinect Fighter Within and Wii Boxing. This strategy allowed a wide range of physical activity intensities to be assessed during active gameplay, as a goal of this study was to determine if the amount and level of physical activity elicited by the active games were associated with changes in pain sensitivity. During game play, time spent in light, MVPA, and sedentary time were measured using an accelerometer worn on the hip.
Pain assessments
The pain assessments were conducted in the following order for every participant: two trials of PPTs on the left ventral forearm, two trials of PPTs on the right trapezius muscle, and three trials of HPTs on the left ventral forearm. Assessments were conducted immediately before and after one 15-minute active gaming period during each session. The specific details for the PPTs and HPTs are described in the following two paragraphs.
Pressure pain thresholds
A handheld, clinical grade pressure algometer (Wagner Instruments, Greenwich, CT) was used for the mechanical procedures. The tip of the algometer consisted of a rubber flat 1.0 cm2 probe. The experimenter applied a constant rate of pressure at an approximate rate of 0.5 kg/s to either the left ventral forearm (∼8 cm distal to the elbow) or the upper right trapezius muscle (posterior to the clavicle). Participants were instructed to respond when the pressure sensation first became painful, at which time the algometer was removed and the amount of pressure in kg was recorded. The average PPT was calculated for each site pre and post each active game.
Heat pain thresholds
Heat stimuli were delivered with a 30 × 30 mm thermode (TSA II Neurosensory Analyzer; Medoc, Ltd., Ramat Yishai, Israel) placed and held on the participant's ventral forearm by the experimenter during testing. The thermode temperature increased from a baseline temperature of 32°C with a rise rate of 0.5°C/s. Participants were instructed to press a button when they first felt the transition from heat to the sensation of heat pain, at which time the trial stopped. Then, the temperature of the thermode was recorded. The average HPT was calculated for the three trials pre and post each active game.
Reliability of pain measures
We conducted interclass correlation coefficients (ICCs) on the pretests for each pain measure to determine the session-by-session reliability of these measures. The ICCs indicated excellent reliability for all pain measures: pretest PPT on the arm ICC = 0.905; pretest PPT on the trapezius ICC = 0.892; pretest HPT on the arm ICC = 0.969.
Accelerometer measurements
An ActiGraph GT3X+ accelerometer (The ActiGraph, Inc., Pensacola, FL) was worn on the hip during all sessions of active gameplay. The ActiGraph is a small lightweight triaxial accelerometer that is designed to detect triaxial accelerations in the range of 0.05–2 G. Output from the ActiGraph was in the form of step counts, body positions, and activity counts for a specific time period. Data were captured in 1-second epochs. The accelerometer data used for analyses were calculated from minutes 2 through 14 (12 minutes total) of each 15-minute active gaming period. Activity count cut-points to determine the amount of time a participant spent in sedentary, light, or moderate-to-vigorous activity was defined as <100 counts per minute (sedentary), 100–1951 counts per minute (light physical activity), and >1951 counts per minute (moderate-to-vigorous activity), respectively. 9 Accelerometer data are reported in minutes.
Data analyses
Descriptives were calculated for minutes spent in sedentary time, light physical activity, MVPA, and moderate and vigorous physical activity separately for each active game. Repeated measures analyses of variance (ANOVA) were conducted on sedentary minutes, light physical activity, moderate physical activity, and vigorous physical activity to determine differences in each type of physical activity across the games. Data for PPTs at the forearm and trapezius and HPTs were analyzed with 5(Condition: Kinect Fighter Within, Kinect Tennis, Wii Boxing, Wii Tennis, Control) × 2(Time: pre, post active game) repeated measures ANOVA. Post hoc comparisons were made with Tukey's HSD (Honestly Significant Difference) procedure. Bivariate correlations were also conducted to determine the relationship between light physical activity, MVPA, and sedentary time with the magnitude of exercise-induced hypoalgesic responses, regardless of active game. For each active game, the exercise-induced hypoalgesic response for each pain test was calculated by subtracting the pretest score from the posttest score. A level of P ≤ 0.05 was used for all statistical analyses.
Results
Descriptive characteristics
The accelerometer data are presented in Table 2 along with the P-values for the repeated measures ANOVA. Data indicated that whole-body movement of participants during gameplay only reached a moderate-to-vigorous intensity level during Kinect Fighter Within (moderate = 4.3 ± 3.0 minutes; vigorous = 1.6 ± 2.0 minutes) and Wii Boxing (moderate = 3.4 ± 3.4 minutes; vigorous = 2.1 ± 3.2 minutes). Accordingly, the ANOVA indicated significantly higher moderate and vigorous activity in the Fighter Within and Wii Boxing games compared with the Tennis games. Participants also experienced significantly less light physical activity while playing Wii Tennis compared with all other games. All games included whole-body sedentary time ranging from Wii Tennis (self-selected intensity period) with almost 10 minutes of sedentary time to Kinect Fighter Within (maximize movement period) with just under 3 minutes of sedentary time. Sedentary time was significantly less during the Fighter Within and Wii Boxing games compared with the Tennis games.
Total time measured was 12 minutes. P-values were calculated from repeated measures ANOVA across games.
Games played with participants instructed to maximize movement.
Games played at a self-selected intensity.
ANOVA, analysis of variance; PA, physical activity.
PPTs on the forearm
Figure 1a shows the mean and standard errors of the pretests and posttests for each condition. The repeated measures ANOVA on the PPTs on the forearm revealed a significant condition × time interaction, P = 0.03. PPTs on the forearm significantly decreased from pretest to posttest during the control condition (Cohen's d = −0.58). PPTs significantly increased from pretest to posttest following Kinect Fighter Within (Cohen's d = 0.41). Additionally, PPTs were significantly greater during the posttest following all active games compared with PPTs during the control condition. The main effects were not significant, P's > 0.05.
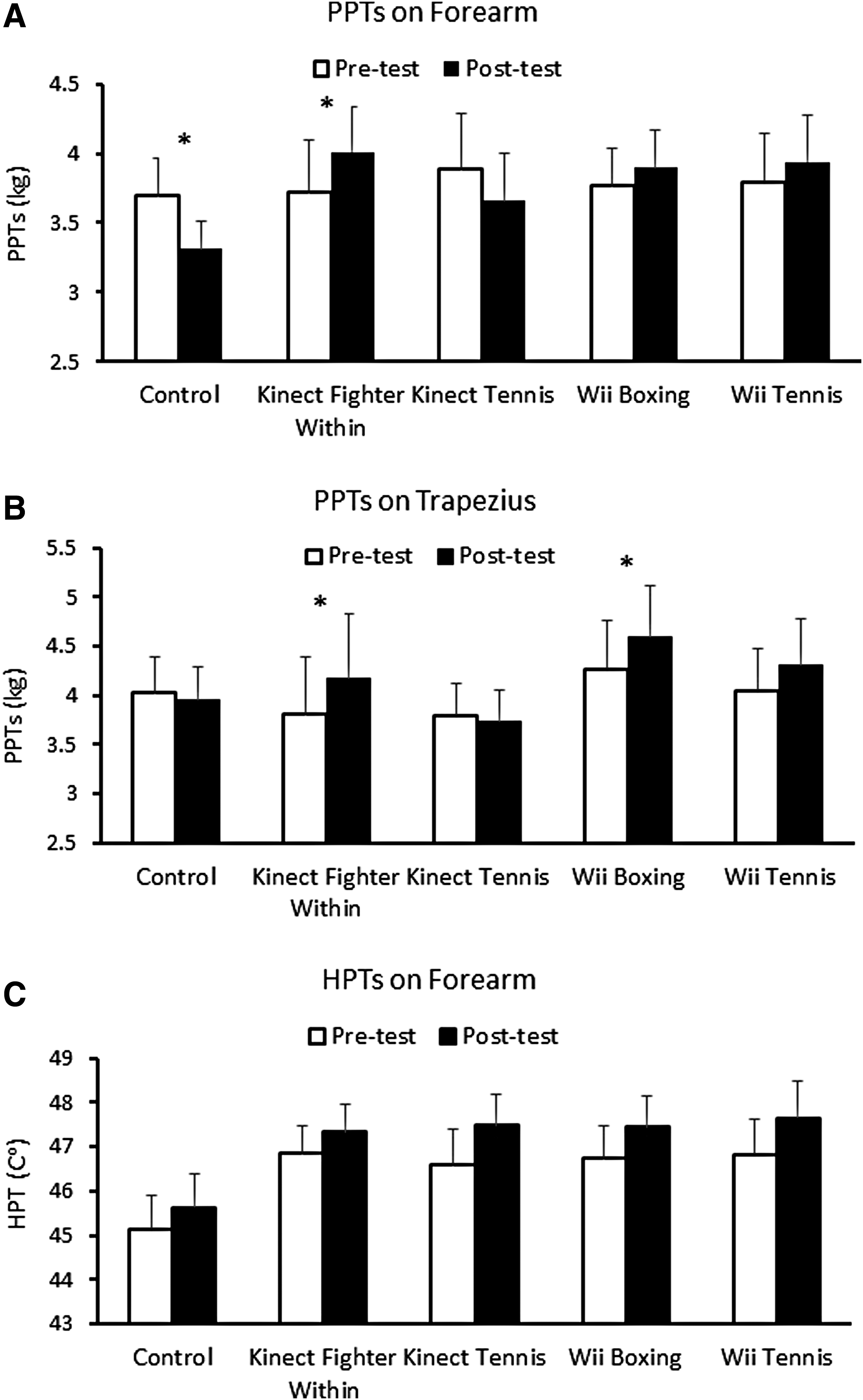
Mean and standard errors for the PPTs on the forearm
PPTs on the trapezius
Figure 1b shows the mean and standard errors of the pretests and posttests for each condition. The repeated measures ANOVA revealed a significant effect of time (P = 0.016), which was superseded by a significant condition × time interaction, P = 0.028. PPTs on the trapezius significantly increased from pretest to posttest following Kinect Fighter Within (Cohen's d = 0.44) and Wii Boxing (Cohen's d = 0.42).
HPTs on the forearm
Figure 1c shows the mean and standard errors of the pretests and posttests for each condition. The analysis revealed a significant main effect of condition, P < 0.001. HPTs were lower in the control condition compared with the active game conditions. A significant main effect of time (P < 0.001) also revealed that HPTs increased from pretest to posttest across all conditions.
Bivariate correlations between EIH and time spent in light physical activity, MVPA, or sedentary time
The bivariate correlations among EIH for each pain test and physical activity variable are presented in Table 3. EIH measured with PPTs at the forearm and trapezius was positively correlated with minutes spent in MVPA and negatively associated with sedentary time.
Table represents data from 21 participants, with each participant having four data points for each variable (i.e., one for each game).
Correlation is significant at the 0.01 level (2-tailed).
Correlation is significant at the 0.05 level (2-tailed).
EIH, exercise-induced hypoalgesia; HPTs, heat pain thresholds; MVPA, moderate-to-vigorous physical activity; PPTs, pressure pain thresholds.
Discussion
Prior research has established that an acute bout of traditional moderate-to-vigorous aerobic exercise can reduce pain sensitivity in healthy individuals. 1 However, less is known regarding whether alternative modes of physical activity that might be more appealing and plausible for deconditioned individuals can also produce a hypoalgesic effect. This study was the first to evaluate whether a single session of active gaming can reduce pain sensitivity. Active gaming provides an avenue for participants to be physically active in their home while also being entertained. We discovered that the two games eliciting the greatest MVPA reduced pressure pain sensitivity, whereas the two games eliciting minimal MVPA had no impact on pain perception.
Kinect Fighter Within increased PPTs on the forearm and trapezius, with a moderate effect size. This coincided with the fact that participants displayed the most MVPA (5.9 ± 4.1 minutes out of 12 minutes) while playing this game, which involves the upper and lower body due to the kicking and punching involved in gameplay. Importantly, the hypoalgesic effect was still present even though approximately half of gameplay was spent in either whole-body sedentary or light physical activity levels (2.9 ± 2.7 and 3.2 ± 1.6 minutes, respectively), even when the participants were instructed to maximize movement.
Wii Boxing reduced pressure pain sensitivity on the trapezius, but not the forearm. Similar to Kinect Fighter Within, participants spent just under half of game play in whole-body moderate-to-vigorous activity (5.5 ± 4.4 minutes out of 12 minutes). Prior EIH research has widely shown that short-term (∼2 to 5 minutes), high-intensity isometric exercise exerts generalized hypoalgesic effects (i.e., pain reduction on exercised and nonexercised parts of the body).10–12 In this study, a lack of sustained exercise at higher intensities may have contributed to the lack of a larger generalized hypoalgesic effect induced by active gaming. Indeed, the 15 minutes of gameplay included bouts of MVPA interspersed with bouts of light physical activity and even at times no physical activity.
The observed exercise-induced hypoalgesic effects on the trapezius, but not the forearm during Wii Boxing could have been caused by differential activation of local pain inhibitory effects at the trapezius versus forearm. Past research suggests that EIH postexercise may be produced by local and central pain inhibitory effects and effects may be stronger when local and central effects are combined.12,13 Indeed, the movement elicited during Wii Boxing is primarily arm punches which involve the trapezius muscle more than muscles of the forearm. However, it should be noted that a primary movement of Kinect Fighter Within is also arm punches. Additionally, PPT at the trapezius was measured on the dominant side, whereas PPT on the forearm was taken on the nondominant side. While only speculation, the dominant arm was likely exercised (i.e., threw more punches) more than the nondominant arm during gameplay. As such, the trapezius muscle of dominant arm could have been exposed to greater activation of localized pain inhibitory mechanisms during Wii Boxing compared with the forearm muscles of the nondominant arm.
These results also differ from those seen in previous studies conducted by Hoffman et al. 14 and Naugle et al., 2 where the participants only showed an exercise-induced hypoalgesic effect for PPTs after sustained vigorous activity (∼20 to 30 minutes), but not after sustained moderate intensity or shorter vigorous bouts (10 minutes). In this study, EIH effects were produced within a shorter time frame and at a lower intensity. The location of the pain testing and/or the type of exercise training could have contributed to the contrasting results. The pain testing in the Hoffman and Naugle studies were conducted on body sites not involved in the exercise (i.e., index finger and forearm), whereas in the current study, the pain tests were conducted on the forearm and trapezius, which were likely involved in active game play. Additionally, complete comparisons with these studies are difficult because exercise intensity was measured with different methods across studies (heart rate/VO2 max in Naugle and Hoffman studies vs. accelerometry in the current study). Future research needs to determine the importance of exercising the tested body part for changes in pain sensitivity during active gaming.
Kinect Tennis and Wii Tennis did not reduce pain sensitivity on any measure. This result is not surprising given that the tennis games produced negligible whole-body MVPA and only ∼3 minutes of whole-body light physical activity. Our exercise intensity data are in agreement with other active gaming studies showing that Wii Tennis is a light-intensity activity when played at a self-selected intensity.4,5 The lack of an EIH effect during the tennis games combined with our correlational data highlight the importance of MVPA for EIH following aerobic exercise.
Interestingly, our results indicated that heat pain sensitivity decreased across all conditions. Thus, while HPTs increased following active gaming, it also increased following 15 minutes of quiet rest. Thus, pain reduction was likely caused by repeated pain testing rather than by active gaming. Similarly, Vaegter et al. recently found comparable increases in HPTs between isometric exercise and quiet rest conditions. 15 Our results are also in line with previous studies showing no effect of aerobic exercise on HPTs, and that EIH responses are not consistent across experimental pain tests, demonstrating the importance of multimodal pain assessment when studying EIH.2,15–18
A few limitations of this study should be noted. First, only young to middle-age healthy adults were tested and these results may not generalize to older adults or individuals with chronic pain. Second, participants played each active game for two 15-minute periods (i.e., self-selected intensity period and maximize movement period) and the current study did not measure pain thresholds before and after each period. Consequently, it cannot be determined whether Fighter Within or Wii Boxing played at a self-selected intensity would produce EIH. Conversely, the Tennis games played with instructions to maximize movement may have produced analgesic effects. Likely, the primary factor as to whether an active game exerts an analgesic effect is the intensity level reached during gameplay. Third, while the order of the experimental active gaming sessions were randomized across participants, the control session was always conducted first. Thus, we cannot rule out the possibility of order effects between the control session and the experimental sessions. Fourth, we based our assessment of exercise intensity on accelerometer data captured at the hip, which would not have captured all bodily movements (i.e., upper limbs).
Clinical implications and future directions
Exercise can cause an acute hypoalgesic effect that could be beneficial for those suffering from different forms of chronic pain. However, many of these individuals are deconditioned and unable to exercise at sustained higher intensities because of their conditions. Additionally, several studies suggest that vigorous aerobic exercise fails to produce a hypoalgesic effect in individuals with central pain inhibitory deficiencies, such as fibromyalgia patients and chronic fatigue syndrome.16,19,20 We provide preliminary evidence that active gaming may have value as an exercise tool for pain management. Indeed, we showed that active gaming can produce an exercise-induced hypoalgesic effect without long bouts of strenuous activity in healthy adults. Notably, both Kinect Fighter Within and Wii Boxing reduced pain sensitivity even though on average 25% of the time assessed during gameplay was spent in whole-body sedentary time. Furthermore, in individuals with chronic pain, the act of interacting with the game could also enhance compliance with exercise therapy and serve as a pleasant distraction from pain symptoms. In support of this notion, Mortensen et al. recently revealed in an observational study that individuals with fibromyalgia reported that active games provided a manageable form of exercise and distraction from pain sensations while playing. 21 Thus, active gaming may be a viable option for deconditioned individuals and those suffering from chronic pain. Additional research should examine active gaming in chronic pain populations to test its efficacy as a cardiovascular and pain management tool. If deemed effective, active gaming could pose as an inexpensive, pragmatic tool to aid in the rehabilitation of individuals suffering from chronic pain.
Footnotes
Acknowledgment
This study was funded by the National Institute for Fitness and Sport and School of Physical Education and Tourism Management Student Research Fund.
Author Disclosure Statement
No competing financial interests exist.