
Abstract
Abstract
Objective:
Develop and test feasibility of a mobile videogame intervention to decrease high-risk sexual behavior in black and Hispanic adolescents.
Materials and Methods:
Iterative design to develop intervention in partnership with target audience. Feasibility and preliminary impact data collected at baseline, following 2–3 hours of gameplay and at 8-week follow-up.
Results:
Twenty-six 15–17-year-olds completed pilot testing: 16 (62%) were male, 20 (77%) black or Hispanic. Pilot testing demonstrated feasibility, including producing a usable videogame prototype, incorporating videogame testing within a high school, and participants' acceptability of the videogame. Participants' gameplay experience reflected that most would play the videogame again (77%), stated that they felt responsible for the choices they made in the videogame (73%), and would tell their friends to play the videogame (58%). Most suggested adding more videogame content to further engage participants. From baseline to follow-up, participants demonstrated improvements in condom and contraception self-efficacy (P = 0.003), risk perceptions (P = 0.009), and high-risk sexual behavior knowledge (P < 0.0001). Among black or Hispanic adolescents, we found improvements in summary measures of intentions (P = 0.04), self-efficacy (P = 0.003), risk perceptions (P = 0.002), and sexual knowledge (P = 0.0002). Adolescents with previous sexual experience showed similar improvements.
Conclusion:
Pilot testing of an innovative videogame, developed in partnership with the target audience, demonstrated feasibility and preliminary impact with this cohort of black or Hispanic adolescents. We developed a usable videogame prototype and gained important data about how to enhance the next videogame iteration. Future plans include targeting an older age group to maximize our ability to measure potential impact among sexually experienced adolescents.
Introduction
B
Some evidence supports behavioral interventions that target knowledge, intentions, risk perception, and self-efficacy as critical antecedents to decreasing high-risk sexual behavior in adolescents.1,5 These targets are consistent with three theories of behavioral change that are incorporated into the videogame. The Theory of Planned Behavior holds that an individual's intention to engage in a specific behavior predicts that behavior. The Health Belief Model emphasizes the importance of individuals' self-efficacy to accomplish a given behavior, their perceptions of susceptibility to a given health problem, and their knowledge of and beliefs in the effectiveness of an intervention. The Social Cognitive Theory posits that observational learning, seeing the modeling of a behavior and the consequences of that behavior, may increase the likelihood of behavioral change.
Therefore, our framework (Fig. 1) for the videogame incorporates these theories as the basis for intervention targets proved to be effective at decreasing overall sexual risk-taking behavior in adolescents, such as improving intentions regarding sexual decision-making (number of partners, intercourse under the influence of alcohol or marijuana), self-efficacy regarding discussion and use of condoms, risk perception, and sexual knowledge. Addressing these targets has been shown to empower adolescents to increase condom use, increase use of contraception, decrease the number of concurrent sexual partners, and increase STI testing and treatment. 6 However, existing evidence-based interventions predominantly rely on being integrated into overloaded school curriculums and are limited by abstinence-only education mandates, 7 overextended educators, and nonexistent national standards. Therefore, innovative approaches to decrease high-risk behavior that have the potential to address current limitations for delivering evidence-based interventions and are tailored to address racial and ethnic disparities are needed. 8
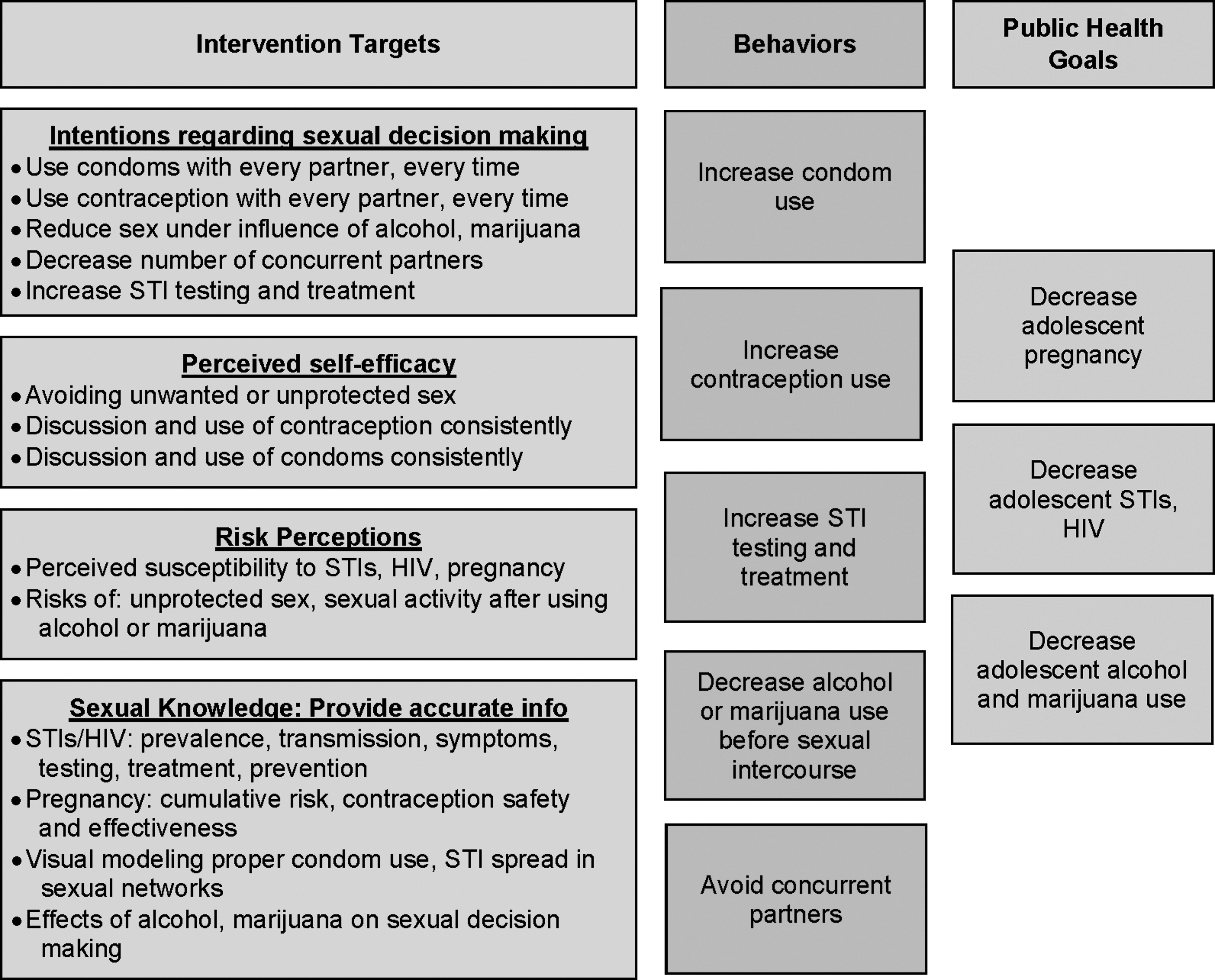
Focused logic model. Modified from “Sexual Risk & Protective Factors. Factors affecting teen sexual behavior, pregnancy, childbearing, and sexually transmitted disease: Which are important? Which can you change?” 1
Videogames can be developed as interventions for improving health behaviors and are a novel and effective way to reach at-risk populations, including adolescents.9,10 Videogames offer opportunities for visually modeling risk and risk prevention, including simulating consequences of high-risk sexual behavior, and practicing self-efficacy skills in a risk free, virtual world.9–11 The purpose of this study was to develop and evaluate a videogame to deliver a behavioral intervention to decrease high-risk sexual behavior among black and Hispanic adolescents, especially as it relates to unintended pregnancy.
Materials and Methods
We used an iterative design methodology to develop and test a videogame intervention (Table 1) with black and Hispanic adolescents. The study consisted of two stages, intervention development and pilot testing, and was approved by the Yale University Human Research Protection Program.
Characteristics of a Videogame for Health
Baranowski. 15
HIV, human immunodeficiency virus; STI, sexually transmitted infection.
Formative work: intervention development
We performed formative work in two phases. In Phase 1, we conducted four focus groups (total participants n = 16) to explore high-risk sexual behavior in adolescents and to understand specific risk behaviors, including contraception use/nonuse and drug use/nonuse, which could be integrated into the design and development of a tailored mobile videogame intervention. We recruited adolescents from a local high school and an afterschool program. Eligibility criteria included the following: adolescent females and males, aged 15–17 years, English-speaking, and who have their own mobile phone. There were no eligibility criteria for prior sexual experience. Parental notification and adolescent verbal assent was provided. Only nonidentifying demographic information was collected.
Focus group participants in Phase 1 had a mean age of 16 years, participants primarily identified as black (44%) and Hispanic (62%), and 63% of participants were female. Four prominent themes emerged in these focus groups: (1) videogames and social media permeate adolescents' lives, (2) alcohol and marijuana use is common among peers and escalates high-risk sexual behavior, (3) misperceptions related to sexual behavior are prevalent among peers and impact adolescents' decisions, and (4) adolescents perceive a lack of control (self-efficacy) over their sexual health.
These themes confirmed and supported our key intervention targets (Fig. 1). In general, adolescents agreed that a mobile videogame that teaches and demonstrates the consequences of sexual risk taking could be useful and made detailed and creative suggestions for how to improve the videogame. For example, participants suggested specific dialog to be used when avatars in the videogame were discussing sexual decision-making. They recommended using avatars with diverse skin tones, blurring any background images in the videogame to represent the effect that choosing to use alcohol or drugs in the videogame had on the player, and endorsed a house party as the basic foundation for the videogame.
Information from the focus groups in Phase 1 was used to create an initial prototype of the videogame, which was then play tested on individual iPads by three focus groups (total participants n = 10). We recruited adolescents from a local high school and two afterschool programs in New Haven County. Eligibility criteria for Phase 2 were the same as for Phase 1. In addition, adolescents could not have previously participated in the study. Parental notification and participant verbal assent were provided.
Focus group participants in Phase 2 had a mean age of 16 years, and primarily identified as black (70%) and Hispanic (10%), and 70% were female. Ideas and feedback from one focus group discussion were incorporated into the next videogame prototype and focus group until thematic saturation was reached and a final prototype was produced.9–11 Participants spent 20–30 minutes playing the initial prototype of the videogame and then participated in focus group discussions to provide feedback and suggestions for improving the videogame. For example, participants recommended awarding points for unlocking information in the videogame and recommended that avatars be prevented from exiting sexual encounters if they had chosen to use alcohol or drugs in the videogame, to simulate the flawed decision-making that accompanies alcohol or drug use.
Pilot testing
We pilot tested the videogame prototype (Fig. 2) with adolescents to determine feasibility and preliminary impact. Eligibility criteria included the following: ages 15–17 years, English-speaking, who had not participated in the study previously. To protect participants' privacy (from parents, other participants), there were no eligibility criteria for previous sexual experience. For pilot testing, written parental consent and written adolescent assent were provided. We assessed gameplay experience, including acceptability, engagement, game completion, and satisfaction using Likert-type scales. We conducted focus groups at 8-weeks follow-up, directly after participants completed quantitative surveys.
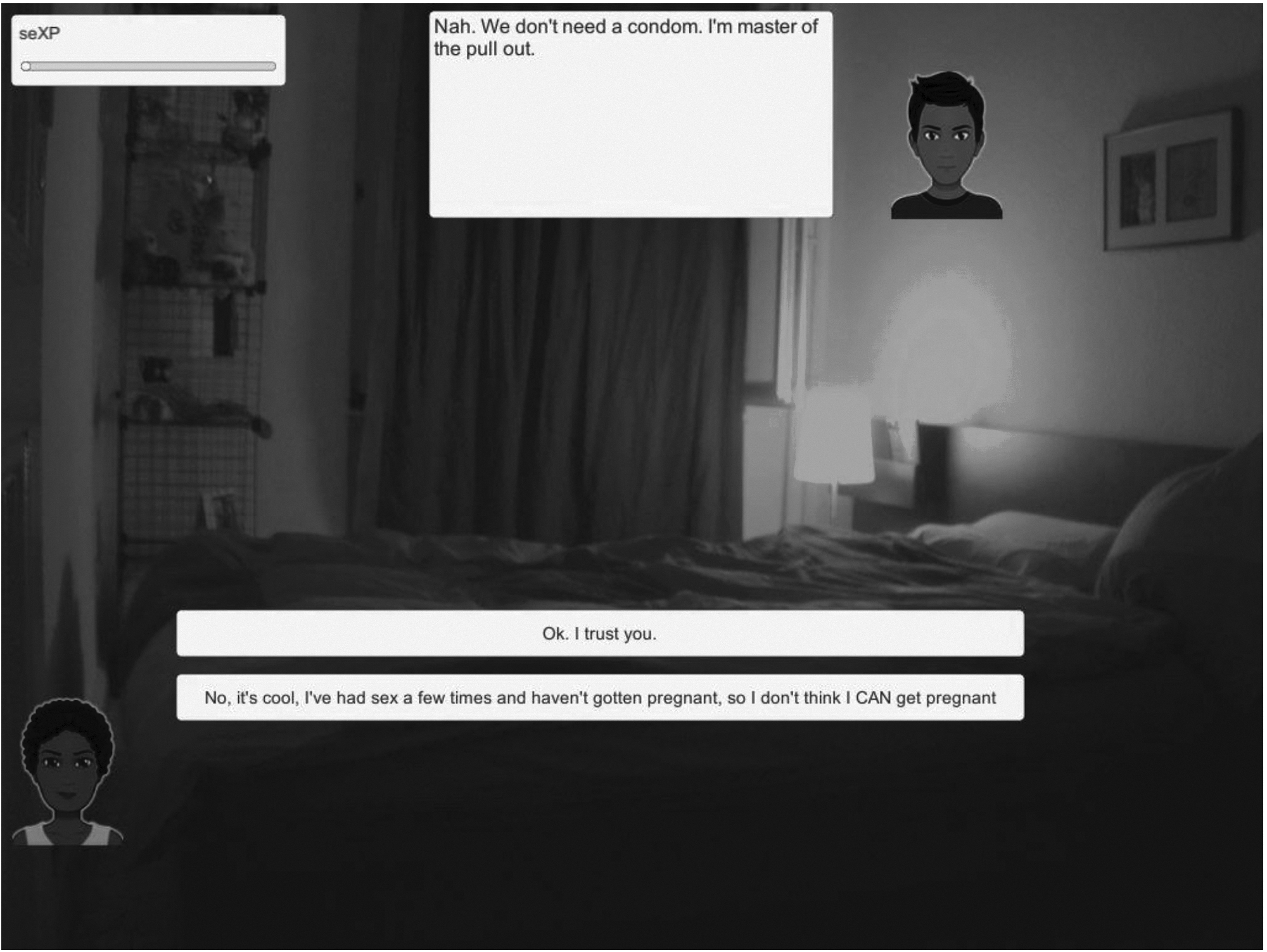
Screenshot from videogame depicting bedroom scene, dialog tree, and seXP (sexpert points meter) in upper left-hand corner.
We collected demographic data, including sexual behavior at baseline via self-administered paper survey, after 2–3 hours of gameplay, and 8-weeks after completion. We measured intentions regarding sexual decision-making (number of partners, intercourse under the influence of drugs, condom use), risk perceptions, self-efficacy, and sexual knowledge using validated instruments and questions.1,12–14
For all focus groups, we used a standard interview guide and asked open-ended questions to gain insights into overall sexual risk-taking behavior in adolescents,1,5 and videogame content, mechanics, and storylines. Focus groups were audio recorded, transcribed, and analyzed using framework analysis to identify key concepts. Salient concepts and suggestions were then incorporated into iterative videogame refinement. Baseline participant demographics and quantitative survey items were analyzed using descriptive statistics. We used paired signed-rank tests to compare data at baseline and follow-up and Pearson's correlations to describe associations between feasibility and outcome measures.
Results
Twenty-six adolescents (aged 15–17) participated in videogame pilot testing (Table 2): mean age of 16 years, 16 (62%) were male, 20 (77%) self-identified as black or Hispanic. At baseline, 12 (46%) of participants had ever been sexually active with mean age of sexual debut of 14 years old, 50% of sexually experienced participants reported two or more lifetime sexual partners and two or more sexual partners in the last 3 months. Participants played the videogame for 2–3 hours on average.
Participant Characteristics
Pilot testing demonstrated feasibility, including producing a usable videogame prototype, incorporating videogame testing within a high school, and participants' acceptability of the videogame. Participants' gameplay experience reflected that most would play the videogame again (77%), stated that they felt responsible for the choices they made in the videogame (73%), and would tell their friends to play the videogame (58%). Some (39%) stated that they would make decisions in life as they made in the videogame, which likely reflects the discrepancy between the videogame's focus on sexual encounters compared with the proportion (46%) of our participants who were not sexually experienced.
Stronger agreement with making decisions in life, as they made in the videogame, was associated with greater improvements in summary self-efficacy (r = 0.41, P = 0.04) and summary risk perception scores (r = 0.52, P = 0.008) from baseline to immediate postgameplay testing. Adolescents reporting that they would play the videogame again had greater improvements in summary risk perception scores from baseline to 8-week follow-up testing (r = 0.40, P = 0.045). Adolescents reporting that they enjoyed playing the game had greater improvements in summary risk perception scores from baseline to 8-week follow-up testing (r = 0.51, P = 0.009), and from postgameplay to 8-week follow-up (r = 0.42, P = 0.04). Comparing baseline to 8-week follow-up testing for adolescents who said that they were frustrated with this game, there was a moderate inverse correlation (r = −0.41, P = 0.04) with summary risk perception scores.
There were no significant correlations between gameplay variables and summary intention scores or summary knowledge percent scores. During focus group discussion, most adolescents suggested adding more videogame content to further engage participants, including more characters, adding levels of difficulty, extending the story to simulate conversations with parents and partners about an unintended pregnancy.
Pilot testing demonstrated improvements in summary scores (Cronbach's α 0.74–0.88) for self-efficacy regarding condom and contraception negotiation (P = 0.003), risk perceptions (P = 0.009), and sexual knowledge (P < 0.0001) from baseline to 8-week follow-up (Table 3). Although there was no measurable impact on overall summary intention scores, one individual question assessing intention to use effective contraception during future sexual encounters showed improvement (P = 0.035). No significant changes were seen in self-reported sexual behavior (Table 3).
Participant Data Before and After Videogame Intervention
Bolded text indicates statistically significant result.
P values evaluated by Signed rank.
Total scores and percentages may change due to missing observations.
Higher scores indicate improved intentions, self-efficacy, and risk perceptions as measured by five-point Likert scales where 0 = I strongly disagree, 1 = I disagree, 2 = not sure, 3 = I agree, 4 = I strongly agree. The statements are worded in the affirmative. For example, “If I have sex without contraception (something to prevent pregnancy), I would probably get pregnant (or get someone pregnant).”
SD, standard deviation.
When stratified by previous sexual experience, adolescents who reported having at least one prior experience of sexual intercourse demonstrated statistically significant improvements in summary measurements of intentions (P = 0.04) from immediate postgameplay to 8-week follow-up, and significant improvements in self-efficacy (P = 0.046), risk perceptions (P = 0.02), and knowledge (P = 0.001) from baseline to 8-week follow-up.
When stratified by race and ethnicity, black or Hispanic adolescents demonstrated statistically significant improvements in summary measurements of intentions (P = 0.04), self-efficacy (P = 0.003), risk perceptions (P = 0.02), and knowledge (P = 0.0002) from baseline to 8-week follow-up. We found no statistically significant differences in summary measurements of intentions, self-efficacy, risk perceptions, or knowledge from baseline to after gameplay, from baseline to 8-week follow-up, or from after gameplay to 8-week follow-up among three groups of participants: black non-Hispanic (n = 6), nonblack Hispanic (n = 14), and nonblack, non-Hispanic adolescents (n = 6).
Discussion
Pilot testing of an innovative videogame, developed in partnership with the target audience, demonstrated feasibility and impact with this cohort of black or Hispanic adolescents. We developed a usable videogame prototype that most participants would play again and we gained important data about how to enhance the next videogame iteration: adding more videogame content to further engage participants and targeting an older age group to maximize our ability to measure potential impact among sexually experienced adolescents.
Overall, significant improvements were noted in summary scores for self-efficacy, risk perceptions, and sexual knowledge. One individual question assessing intention to use effective contraception during future sexual encounters showed improvement. Perhaps more importantly given our target audience of black or Hispanic adolescents, we found improvements in summary measures of intentions, self-efficacy, risk perceptions, and sexual knowledge among sexually experienced adolescents, and among black or Hispanic adolescents. Our findings add to growing evidence supporting the potential for videogame interventions to deliver behavioral change. 9
Our study is limited by its small sample size, lack of control group, and short follow-up time that precluded our ability to test for changes in sexual behavior. Recruitment bias may have occurred if adolescents chose not to participate to avoid disclosing their sexual experience. However, this did not seem to be a hindrance as 56% of participants reported sexual intercourse.
Further rigorous testing of this innovative videogame to decrease high-risk sexual behavior will include a control group and target an older age group to maximize our ability to measure potential impact among sexually experienced adolescents. If successful, a videogame for adolescents that decreases high-risk sexual behavior has the potential to decrease unintended pregnancy and STIs/HIV in this vulnerable and difficult to reach population.1,4
Footnotes
Acknowledgments
We acknowledge our videogame partner developers at PreviewLabs and Timothy Nanzer who provided input and guidance in videogame programming, scripting, and debugging. We offer special thanks to the school and after-school teachers and staff and all the adolescents who participated and made a major contribution to this study. All authors were supported by a Society of Family Planning Research Fund: Interdisciplinary Innovation grant. Dr. Gariepy was also supported by NIDA 5K12DA033312.
Author Disclosure Statement
No competing financial interests exist.