
Abstract
Abstract
Nondigital board games are being used to engage players and impact outcomes in health and medicine across diverse populations and contexts. This systematic review and meta-analysis describes and summarizes their impact based on randomized and nonrandomized controlled trials. An electronic search resulted in a review of n = 21 eligible studies. Sample sizes ranged from n = 17 to n = 3110 (n = 6554 total participants). A majority of the board game interventions focused on education to increase health-related knowledge and behaviors (76%, n = 16). Outcomes evaluated included self-efficacy, attitudes/beliefs, biological health indicators, social functioning, anxiety, and executive functioning, in addition to knowledge and behaviors. Using the Cochrane Collaboration tool for assessing bias, most studies (52%, n = 11) had an unclear risk of bias (33% [n = 7] had a high risk and 14% [n = 3] had a low risk). Statistical tests of publication bias were not significant. A random-effects meta-analysis showed a large average effect of board games on health-related knowledge (d* = 0.82, 95% confidence interval; CI [0.15–1.48]), a small-to-moderate effect on behaviors (d* = 0.33, 95% CI [0.16–0.51]), and a small-to-moderate effect on biological health indicators (d* = 0.37, 95% CI [0.21–0.52]). The findings contribute to the literature on games and gamified approaches in healthcare. Future research efforts should aim for more consistent high scientific standards in their evaluation protocols and reporting methodologies to provide a stronger evidence base.
Introduction
The application of game design approaches and technologies has gained popularity in healthcare as a means of creating more engaging interventions, which can improve knowledge, change real-world behaviors, and subsequently impact therapeutic outcomes. Successful examples exist in the areas of treatment adherence, pain management, physical rehabilitation, depression, schizophrenia, and phobias.1–6 Games can support engagement in play and fantasy, which are described as important mechanisms facilitating greater attentional control, enhanced learning and providing patient insight toward impacting long-term behaviors. 7 From a theoretical perspective, it has been suggested that games stimulate or facilitate learning through immersion flow, and meeting individual's needs concerning mastery, fantasy, challenge, and connectedness.8–11
Although digital games are popular, nondigital formats have also been addressed in the research literature. 12 Board games have a history of use in therapeutic contexts.13–15 Aside from its engaging and entertaining characteristics, one of the great advantages of using a board game is its ability to facilitate face-to-face interactions with peers, tutors, family members, or even a therapist. These social interactions are assumed to enhance learning opportunities. 16 However, only a very small proportion of board games described in the literature have been evaluated to determine their impact. 16 Reviews focusing on evaluating the use of board games in medical education, conclude that it would be premature to claim that board games have an impact on knowledge or other educational outcomes in medicine given the strength of the existing evidence reviewed.17,18 More recently, evaluations of board games for health with patients and community members have demonstrated promising impacts on knowledge (e.g., knowledge of HIV and sexually transmitted diseases; STIs), 19 health behaviors (e.g., improved food habits), 20 and objective indicators of health (e.g., HbA1c improvements among patients with Type II Diabetes). 21 Results of these evaluations have not been synthesized or systematically assessed in the literature to date. Thus, there is a need to update previous reviews of board games in medical education and to expand the review, including evaluations of board games in other healthcare contexts.
The aim of this systematic review and meta-analysis is to answer the following two questions: (1) What kinds of board games targeting medical and health-related outcomes have been evaluated in the literature? and (2) What is the overall impact of these board games on health-related outcomes?
Method
This review follows the guidelines for the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA).22,23 In conformity with these guidelines, the Supplementary Data (available online at https://www.liebertpub.com/suppl/doi/g4h.2018.0017) provide readers with additional detail regarding our method and results, while keeping the body of this article a manageable length. The Supplementary Data include detailed database search terms and strategies, elaborated descriptions of data collection and analysis methods, details of within-studies risk of bias (RoB) analyses (e.g., bias matrices and interrater reliability results), effect sizes (ES) for each outcome comparison included in this study, and expanded results of publication bias analyses.
Inclusion and exclusion criteria
In this article, board games are defined as “a game of strategy […] played by moving pieces on a board,” 24 which does not include games played exclusively with cards (“card games”) or dice. Inclusion criteria were evaluations (1) of a health or medical-related nondigital board game intervention; (2) either as a standalone intervention or as part of a larger intervention program; (3) using random or other method of assignment to no treatment or active control group; (4) with participants from any sociodemographic background; (5) assessing medical and health-related outcomes; (6) of scholarly publications in a journal, thesis, research report, or conference proceeding; (7) published in English. Exclusion criteria were evaluations (1) of digital board games (i.e., played on computers or smart phones); (2) of board games not implemented as an intervention (e.g., used as an assessment tool); and (3) of a board game's impact on processes rather than outcomes (e.g., usability, acceptability, credibility). Notably, digital board games were not included because they breach into the category of digital game-based learning and often involve more complex gaming and learning mechanics, which would increase the heterogeneity of the included studies, rendering conclusions about overall efficacy more difficult to summarize. 16
Search method
An electronic search was performed on five databases: ProQuest (encompassing ERIC, IBSS, PsycINFO), Scopus, PubMed, JSTOR, and OVID (encompassing Medline, Embase). The search targeted board games specifically (term: “board game”) in the area of health (terms: “health,” “medical,” “patient,” “illness,” “disease”) (Supplementary Data for full search details). The searches were performed on February 8, 2017 and include studies available up until this date. Hand searching of the reference lists of articles that met final eligibility was also performed using the “snowball sampling” method. 25
Study selection
Database search results were imported into RefWorks, where duplicates and non-scholarly publications were removed. The remaining abstracts were screened to exclude articles if a nondigital medical or health-related board game was not mentioned. The full texts of the remaining articles were reviewed in detail to see if they met the inclusion/exclusion criteria. Reasons for excluding articles were documented. Three researchers independently evaluated the articles for eligibility for inclusion. A fourth rater performed a reliability check of a random selection of 33% of the articles for eligibility. Interrater reliability was calculated using Cohen's kappa (κ) coefficient, where a value greater than 0.7 would be deemed acceptable. The raters met to discuss and resolve any discrepancies until 100% agreement was achieved.
Data collection and data items
For each included article, information such as the study design, participant characteristics, sample size, and means and standard deviations of measured outcomes at each recorded time point (preintervention, postintervention, delayed follow-up) were extracted (all data items are listed in the Supplementary Data).
To identify what aspects of health and medicine have been impacted by board games in the literature, we performed a preliminary inductive coding of the measures and outcomes in each article. Only outcomes that were measured for the board game group and one or more comparison groups were coded. Following the preliminary coding, the primary coder and another investigator held a meeting to refine the coding scheme until 100% agreement on codes was reached.
Data analyses
Summary measures
Based on the extracted detailed data, the ES and 95% confidence intervals (CIs) were calculated using Cohen's d, based on a between-group mean difference for each continuous data outcome at each time point (preintervention, postintervention, delayed follow-up). 26 For dichotomous data, ES and standard errors were first calculated with a log odds ratio (using natural logarithm) then converted to Cohen's d by the method described in Borenstein et al. (p. 47), 27 to establish comparability. Special considerations in the ES calculation were made for studies with a cluster randomized design, for studies with multiple comparison groups, and for studies with multiple outcome measures within the same outcome category (Supplementary Data). 28
Since most outcome measurements extracted from the included studies did not report variance metrics for pre-to-postintervention change/improvement (only 7.4% of outcomes included these data), our analysis focused on ES comparing postintervention scores between experimental groups and, when reported, delayed follow-up scores. The ES of preintervention scores were taken into account when evaluating the RoB for each comparison. Where negative ES represented a preferred outcome (e.g., age- and sex-adjusted body mass index (zBMI) as related to obesity, or reduction in positive attitudes toward cigarette smoking), these results were multiplied by −1 to reflect a positive result in the meta-analysis.
Synthesis of data
It has been argued that combining heterogeneous studies may be appropriate if the purpose of the analysis is to come to higher-order generalizations about the topic in question.29,30 As such, this review combines heterogeneous studies investigating an array of board games and populations to answer our research questions. A summary of inconsistency across studies for each outcome is given by the value I2 under each table summarizing the meta-analysis.
28
For each outcome measure category (e.g., knowledge, behavior, self-efficacy, etc.)—and separately for both postintervention and delayed follow-up time points—the following random-effects meta-analyses are produced when two or more data points were available:
An overall analysis that synthesizes all comparisons, where an ES could be calculated (Summary Measures section). A sensitivity analysis using only outcome comparisons at a low RoB.
Risk of bias
RoB in individual studies
For each extracted outcome measure, its RoB was assessed using the Cochrane Collaboration tool for assessing RoB, 28 where six categories of bias (selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias) were evaluated. These categories were judged as either “low risk,” if the bias was unlikely to affect the study's results; “unclear risk,” if the information was not included or was insufficient; or “high risk,” if the bias would seriously affect confidence in the results. Two raters assessed risk in each study and interrater reliability for each category of bias was calculated using Cohen's kappa coefficient, where a value greater than 0.7 was deemed acceptable. Discrepancies between the two assessors were identified, discussed, and resolved with 100% agreement.
RoB across studies
The inverse standard error and the weighted variance for each study's combined d statistic were calculated to investigate the risk of publication bias across studies visually with a funnel plot. Egger's regression test was used to assess the (1) overall publication bias in the literature (i.e., across outcomes) at postintervention and delayed follow-up separately, and (2) for each outcome category individually, at the postintervention time point. For the analysis across all outcomes, to avoid a unit-of-analysis error, all results from each study were combined into a single ES (Supplementary Data: Summary Measures section).
Results
Study selection
Our electronic database search resulted in a total of n = 1043 articles from ProQuest (n = 578), Scopus (n = 185), PubMed (n = 55), JSTOR (n = 18), and OVID (n = 207), whereas another three (n = 3) other references were identified as potential candidates based on a “snowball” search of the reference lists of eligible articles. Figure 1 documents the study selection process. A total of 22 articles met our inclusion/exclusion criteria; however, n = 2 articles reported the same outcomes and intervention.31,32 Data from these two articles were extracted, summarized, and considered as one article, resulting in 21 total selected studies. Additionally, two of the articles evaluated the same board game reported on different outcomes in two distinctly different studies.20,33 They are thus considered separate studies of one board game in this report. Interrater reliability on the study selection process was high, with κ = 0.86 and a 97.92% agreement rate.
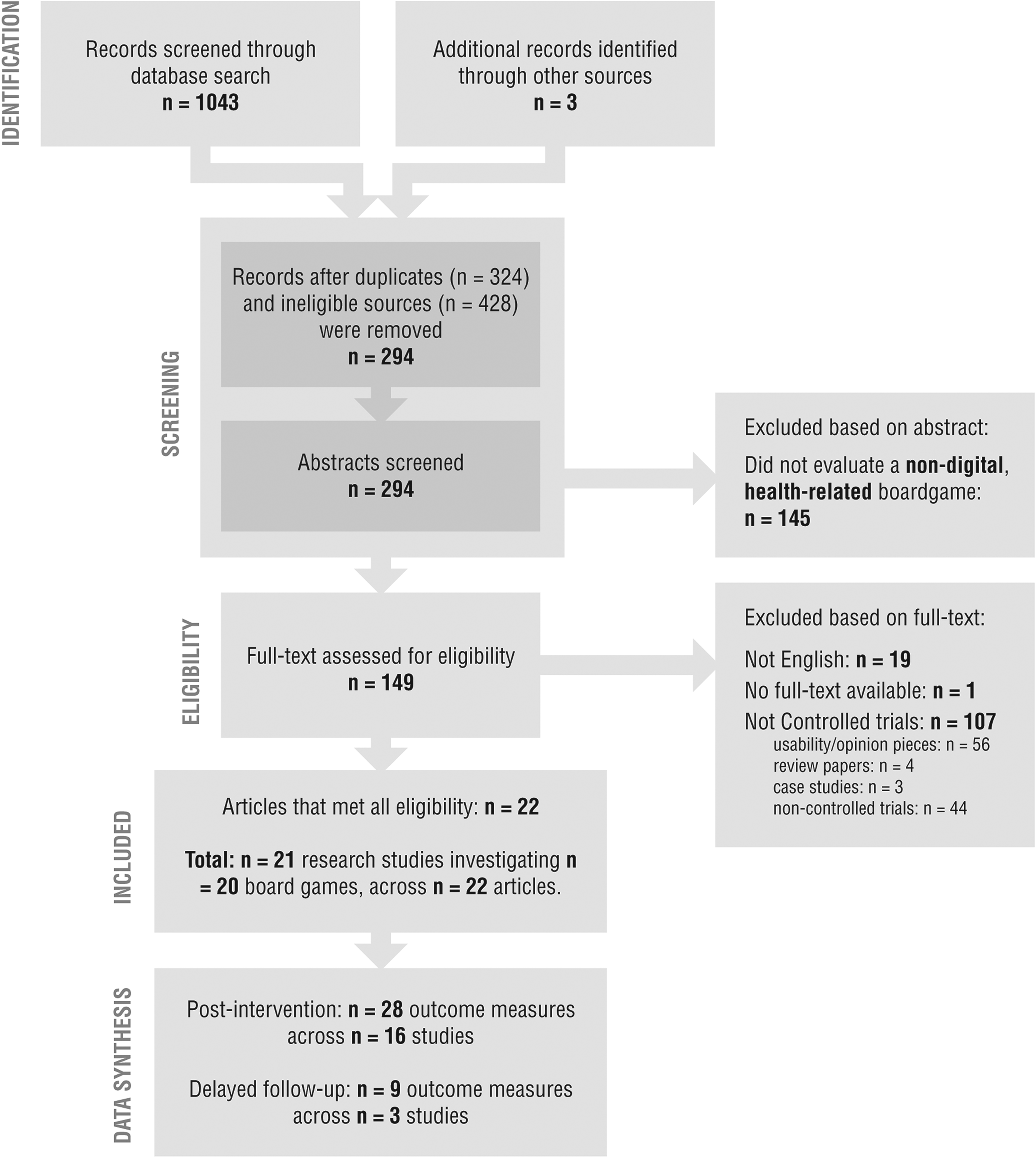
Flow diagram of study selection process.
Study characteristics
Table 1 summarizes study characteristics across the 21 research studies, including study designs, sample/cluster sizes, populations/locations, and play duration, whereas the details of each board game intervention (i.e., purpose, general intervention structure, and mechanics employed) are presented in Table 2.
Study Design Characteristics, Including Sample Size, Age Range, Location of Study, Description of Participants, Types of Comparison Group(s), and the Duration of the Intervention (i.e., How Long Did the Participants Play The Game)
cRCT, cluster-randomized controlled trial; NRS, nonrandomized study; RCT, randomized controlled trial.
Board Game Intervention Titles, Content Description, and Identifiable Learning Mechanics for Each Study
Study design
Studies consisted of n = 11 randomized controlled trials; n = 4 cluster randomized controlled trials; and n = 6 quasi-experimental or nonrandomized trials, one of which was a case–control trial. Most of the studies (n = 16) included a “no intervention” or a standard of care/learning comparison group. Two studies compared the board game with other educational media,34,35 and four compared the board game with an educational lecture.19,31,32,36,37 Finally, two studies included a specialized training intervention as control that mirrored the content/experiences targeted in the board game.38,39
Sample sizes
Studies varied in sample size, from small (n = 17) 40 to large (n = 3110 across 20 clusters), 20 with n = 6554 total participants across all 21 studies. Of these, n = 3055 received a board game-based intervention and n = 3499 were in a comparison/control group.
Populations
The samples used to evaluate the board games included a wide range of age groups, from children as young as 8 years old 35 to older adults. 40 Most (57%, n = 12) of the studies' participants were students enrolled in school. Participants in the remaining n = 9/21 studies (who were not students enrolled in schools) were patients in n = 6 studies and people recruited from specific communities in the remaining n = 3 studies.
Duration of play
Interventions varied in total play-time reported ranging from 5 minutes 38 to 30 hours, 40 and in overall duration of intervention, from a single session to 24 weeks. 33
Description of the board game interventions
Purpose/aims of the board game interventions
Most of the board game interventions focused on education to increase knowledge and/or skills (n = 17/21 studies representing 16 board games). The remaining board games evaluated in n = 4/21 studies aimed to directly impact a neurological skill (i.e., cognitive functioning for community seniors), 40 physical rehabilitation skills (i.e., hand pinch strength), 38 increase interest in Global Health issues, 41 or change in motivations among community members to increase their intentions to seek local pharmacy advice. 42
General intervention structure
Most of the included studies (n = 15 studies, representing n = 14 board games) evaluated a board game in itself as an intervention, whereas n = 6 studies investigated the effect of a board game as part of a multicomponent intervention program.
Game design and mechanics
The mechanics for only n = 15/20 board games could be interpreted (Table 2). Notably, most games (n = 12) were competitive in nature. The most popular learning mechanic implemented in the board game was a question-and-answer (self-testing) strategy, with n = 9 interventions employing this mechanic as their primary method of learning. In all cases, progressing in the game required questions to be answered correctly. In contrast, n = 4 board games implemented an action-and-consequence style of learning mechanic that involved a more reflective learning. For example, to affect diet and lifestyle behavior in children, Kalèdo employs nutrition and activity cards that the children must balance to optimize calorie-intake and energy expenditure; furthermore, the player faces consequences (e.g., loss or gain of points) throughout the game for real-life dietary/exercise decisions made during the day, thereby enhancing their understanding of healthy and unhealthy behavior and encouraging real-world transfer.20,33
Outcomes assessed
Coding of the outcome measures resulted in eight categories of health-related outcomes across the studies: (1) health-related behavior (including self-reported behavior, self-reported behavioral intentions, and measured behaviors), (2) knowledge (of a health concept or skill), (3) self-efficacy (perceived confidence in one's abilities to carry out a health-related behavior), (4) attitudes and beliefs about a health concept, (5) biological health indicators, (6) social functioning, (7) anxiety, and (8) executive functioning. The distribution of studies, measures, and between-group comparisons across outcome categories are presented in Table 3. Hereafter, we use the term “outcome” to refer to the construct that was measured; the “measure” to refer to the method or means used to quantify the outcome; and “comparison” to refer to a between-group analysis of two or more comparisons between groups for a single measure (e.g., game vs. no intervention, game vs. lecture).
The Number of Studies, Measures, and Game-Control Comparisons Extracted from the Literature in Each Outcome Category
The number of comparisons in the “Overall” column indicates the raw number of game-control comparisons reported in the studies. The “MA—all RoB” reports the total number of comparisons included in the data synthesis for each category after combining for multiple control groups or multiple measures from the same study. The “MA—low RoB” reports the total number of comparisons at a low RoB included in the sensitivity analyses.
“ Behavior” category includes the three subcategories of “self-reported behavior,” “behavioral intentions,” and “measured behavior.”
MA, meta-analysis; RoB, risk of bias.
RoB within studies
Overall, n = 3 studies were considered to have an overall low RoB19,20,43; n = 7 were considered to have an overall high RoB31,32,35,41,42,44–46; and n = 11 were considered to have an unclear RoB.21,33,34,36–40,47–49 RoB matrices for each outcome category and interrater reliability statistics are reported in the Supplementary Data. Table 3 also presents the number of low RoB and other comparisons suitable for inclusion in the data synthesis.
Results by type of outcome
Below, we present the syntheses of between-group mean difference ES (Cohen's d) for each study categorized by the type of outcome measurement at both the postintervention and delayed follow-up (if applicable) time points (visualized in Fig. 2). Overall synthetic analyses (using comparisons at all levels of RoB) and sensitivity analyses (using only comparisons at a low RoB) are presented. An ES given as “d*” denotes a synthesized effect across two or more studies, whereas “d” denotes an effect within a single study. A summary of the RoB across studies in each category is included in each subsection.

Health-related behavior
Health-related behaviors are made up of the subcategories of self-reported behavior, behavioral intentions, and measured behaviors. Taken together, health behaviors showed a small-to-moderate effect in favor of board games compared with control group(s) at immediate postintervention assessment (d* = 0.33, 95% CI [0.16–0.51], Q = 18.90, df = 7, C = 373.59, Tau = 0.03, I2 = 62.97%, Z = 3.83, P < 0.001) and a small effect in favor of board games at delayed follow-up (d* = 0.24, 95% CI [0.02–0.45], Q = 1.86, df = 1, C = 70.45, Tau = 0.01, I2 = 46.24%, Z = 2.18, P = 0.029). Each subcategory of health-related behavior is discussed individually in more detail below.
Self-reported behavior
In the subcategory of self-reported health behaviors (Table 4), we observe a significant small-to-moderate effect in favor of board games (d* = 0.38, 95% CI [0.07–0.69]) over other control conditions immediately after the intervention takes place. Additionally, we see a small effect at delayed follow-up (d* = 0.24, 95% CI [0.02–0.45]). Overall, the RoB associated with self-reported behavior outcomes was deemed to be “unclear,” with ∼56% of the weight at a low RoB, ∼31% at an unclear RoB, and 13.3% at a high RoB. However, sensitivity analyses—that include only comparisons at a low RoB—show similar effects at both the postintervention (d* = 0.38, 95% CI [0.08–0.83]) and delayed follow-up (d* = 0.24, 95% CI [0.01–0.46]).
Effect Size Details for Studies Measuring Self-Reported Health-Related Behavior
ES, (Cohen's d); “Comps” refers to the number of game-control comparisons that were combined (due to multiple outcome measures or multiple control groups) to form the ES used. “Weight (%)” refers to the total weight or contribution each study makes to the synthesized effect.
Q = 8.84, df = 3, C = 99.06, Tau = 0.06, I2 = 66.07, Z = 2.44, P = 0.015.
Q = 1.86, df = 1, C = 70.45, Tau = 0.01, I2 = 46.24, Z = 2.18, P = 0.029.
Q = 3.96, df = 1, C = 35.11, Tau = 0.08, I2 = 74.76, Z = 1.62, P = 0.104.
Q = 1.82, df = 1, C = 60.55, Tau = 0.01, I2 = 44.98, Z = 2.08, P = 0.038.
ES, effect size.
Behavioral intentions
Behavioral intentions as a subcategory are considered distinct from self-reported behaviors because they measure intent to engage in behaviors in the future, as opposed to self-reported behaviors that occurred in the past. A small effect of board games over control groups is observed for behavioral intentions postintervention (d* = 0.28, 95% CI [0.06–0.50]; Table 5). No study measured behavioral intentions at delayed follow-up. The RoB associated with comparisons measuring behavioral intentions is high overall, with 44.3% weighted as “unclear” RoB, and 55.6% as high RoB. No study provided low RoB comparisons, so sensitivity analyses were not performed.
Effect Sizes for Studies Measuring Health-Related Behavioral Intentions
ES (Cohen's d); “Comps” refers to the number of game-control comparisons that were combined (due to multiple outcome measures or multiple control groups) to form the ES used. “Weight (%)” refers to the total weight or contribution each study makes to the synthesized effect.
Q = 4.36, df = 2, C = 116.94, Tau = 0.02, I2 = 54.13, Z = 2.51, P = 0.012.
Measured behavior
Finally, Moyer and Nelson assessed the subcategory of health-related behavior directly, with hand pinch strength (pressure) and pinch repetitions in individuals attending rehabilitation sessions. 38 Combining multiple comparisons in this study, no effect of board game over the control group was observed (d = 0.33, 95% CI [−0.22 to 0.88], Z = 1.18, P = 0.239). This comparison has an overall unclear RoB.
Knowledge
A large and significant postintervention effect of health/disease-related knowledge in favor of board games was observed at immediate follow-up (d* = 0.82, 95% CI [0.15–1.48]). The effect was small and not significant at the delayed follow-up (d* = 0.25, 95% CI [−0.53 to 1.03]). Heterogeneity of the postintervention ES was very high (I2 = 94.50%) and included studies measuring very different types of knowledge. The synthesis of ES for health-related knowledge outcomes have only 28.7% of the weight associated with low RoB, 27.6% with high RoB, and 43.8% with an unclear RoB. Using only low RoB ES, the large postintervention ES remains (d* = 1.05, 95% CI [0.82–1.28]), and the one study 20 that did a delayed follow-up assessment of knowledge shows a marginally significant small-to-moderate effect (d = 0.34, 95% CI [−0.03 to 0.72], p = .063). Refer to Table 6 for details.
Effect Sizes for Studies Measuring Health-Related Knowledge
ES (Cohen's d); “Comps” refers to the number of game-control comparisons that were combined (due to multiple outcome measures or multiple control groups) to form the ES used. “Weight (%)” refers to the total weight or contribution each study makes to the synthesized effect.
Q = 127.18, df = 7, C = 153.19, Tau = 0.78, I2 = 94.50, Z = 2.39, P = 0.017.
Q = 1.08, df = 1, C = 0.63, Tau = 0.13, I2 = 7.58, Z = 0.64, P = 0.525.
Q = 0.48, df = 1, C = 37.29, Tau = 0.00, I2 = 0.00, Z = 9.08, P = 0.001.
Self-efficacy
Self-efficacy refers to an individual's self-perceived abilities to engage in behaviors despite challenges. 50 The mean ES for self-efficacy showed no evidence of an effect at immediate (d* = 0.09, 95% CI [−0.03 to 0.22]) or at delayed follow-up (d* = 0.18, 95% CI [−0.36 to 0.71]), Table 7. The comparisons for self-efficacy are at an overall low RoB, with ∼69% of weighted data at low risk and ∼31% at an unclear risk. Results are consistent with the overall synthesis (above) when analyzing only comparisons with a low RoB at the posttest (d* = 0.12, 95% CI [−0.02 to 0.25]) and delayed follow-up (d* = 0.18, 95% CI [−0.39 to 0.75]).
Effect Sizes for Studies Measuring Health-Related Self-Efficacy
ES (Cohen's d); “Comps” refers to the number of game-control comparisons that were combined (due to multiple outcome measures or multiple control groups) to form the ES used. “Weight (%)” refers to the total weight or contribution each study makes to the synthesized effect.
Q = 2.35, df = 2, C = 165.16, Tau = 0.00, I2 = 14.76, Z = 1.43, P = 0.151.
Q = 14.30, df = 1, C = 95.18, Tau = 0.14, I2 = 93.01, Z = 0.64, P = 0.523.
Q = 0.08, df = 1, C = 64.57, Tau = 0.00, I2 = 0.00, Z = 1.70, P = 0.089.
Q = 9.88, df = 1, C = 58.97, Tau = 0.15, I2 = 89.88, Z = 0.62, P = 0.534.
Attitudes and beliefs
Participants' attitudes and beliefs about a health topic showed a small but significant effect in favor of board games postintervention (d* = 0.15, 95% CI [0.05–0.25]), but not at delayed follow-up (d* = 0.06, 95% CI [−0.05 to 0.18]), Table 8. The comparisons associated with health-related attitudes and beliefs are largely at a low RoB, with ∼72% weighted at low RoB, ∼17% at an unclear RoB, and ∼11% at a high RoB. Sensitivity analyses using only low-RoB comparisons confirm a small effect of board games over other control comparators at the posttest (d* = 0.23, 95% CI [0.11–0.36]) and a very small and trending effect upon delayed follow-up (d* = 0.12, 95% CI [−0.01 to 0.24]).
Effect Size Details for Studies Measuring Attitudes and/or Beliefs
ES (Cohen's d); “Comps” refers to the number of game-control comparisons that were combined (due to multiple outcome measures or multiple control groups) to form the ES used. “Weight (%)” refers to the total weight or contribution each study makes to the synthesized effect.
Q = 2.04, df = 3, C = 226.75, Tau = 0.00, I2 = 0.00, Z = 2.81, P = 0.005.
Q = 0.04, df = 1, C = 88.98, Tau = 0.00, I2 = 0.00, Z = 1.01, P = 0.313.
Q = 0.17, df = 1, C = 111.21, Tau = 0.00, I2 = 0.00, Z = 3.68, P < 0.001.
Q = 0.06, df = 1, C = 85.49, Tau = 0.00, I2 = 0.00, Z = 1.78, P = 0.075.
Biological health indicators
There was a small-to-moderate effect of board games on biological health indicators (e.g., zBMI, diabetes indicators) measured immediately after the intervention (d* = 0.37, 95% CI [0.21–0.52], Table 9). Only Viggiano et al. 20 performed a delayed follow-up measurement, which showed a moderate effect of lower zBMI scores in favor of the game group over a no-intervention group. The comparisons in this category's synthesis showed 45.5% weight at low risk and the remaining 54.6% at an unclear risk. Only the comparisons by Viggiano et al. 20 are at a low RoB, so sensitivity analyses were not performed.
Effect Size Details for Studies Measuring Health-Related Biological Health Indicators
ES (Cohen's d); “Comps” refers to the number of game-control comparisons that were combined (due to multiple outcome measures or multiple control groups) to form the ES used. “Weight (%)” refers to the total weight or contribution each study makes to the synthesized effect.
Q = 5.56, df = 2, C = 328.12, Tau = 0.01, I2 = 64.04, Z = 4.60, P < 0.001.
Social functioning
A single study targeted social functioning in patients with schizophrenia with seven subscales. 39 Although the authors report significant outcomes on a few subscales (e.g., recreational activities), there was no significant effect of the board game on social functioning (d = 0.19, 95% CI [−0.11 to 0.48], Z = 1.22, P = 0.221). The RoB associated with the comparisons in this combined ES was unclear.
Anxiety
The effect of a board game intervention on anxiety was assessed in one study by Fernandes et al. in preoperative children and their parents. 35 The authors did not provide information about variance for the data, which prevented us from calculating ES for anxiety. These comparisons were at an overall high RoB.
Executive functioning
Finally, executive functioning was assessed by Fissler et al. among elderly retirement home patients at risk of dementia. 40 An overall large but nonsignificant effect of the game intervention program was observed at immediate follow-up (d = 0.88, 95% CI [−0.19 to 1.95], Z = 1.82, P = 0.068). This comparison was associated with an unclear RoB.
RoB across studies
The risk of publication bias across studies was assessed visually with a funnel plot (Fig. 3). Although there is a noticeable lack of studies to support other interventions over board games (dots left of zero), Egger's test was not significant for postintervention comparisons (β0 = −0.09, 90% CI [−3.84 to 3.64], dftotal = 16, t = −0.05, P = 0.964). Publication bias was also not observed in the majority of the individual outcome categories (Supplementary Data). Lastly, Egger's test was not significant for delayed follow-up comparisons (β0 = −0.91, 90% CI [−6.05 to 4.24], dftotal = 2, t = −1.11, P = 0.466).

Funnel plot of effect sizes from postintervention and delayed follow-up comparisons against the inverse of the standard error of the effect, across all outcome categories.
Discussion
This systematic review and meta-analysis is the first to provide a synthesis on and analysis of nondigital board games for health impacts for users in academic, patient/hospital, and community settings together. It extends Bochennek et al. review of board games for medical education by also including games for patients and laypeople from a community context. 16 The findings further contribute to theories about how games can facilitate learning and behavior change.8–11 The overall quality of the studies investigated was not high; RoB assessments revealed that 85.7% of the studies had a high or unclear RoB associated with their methodological designs. Keeping these biases in mind, we have been able to draw some general insights about the impact of board games on health-related outcomes and about potential future directions for research.
Main findings
The designs of board games evaluated, and the types of measures used to evaluate outcomes across studies were heterogeneous; a finding that is consistent with previous reviews of board games for medical education that also found the topics addressed and game approaches difficult to place in broad categories due to the diversity of examples in the literature.16,18 The diversity of approaches and topics addressed in board games was also found in reviews of digital game-based learning and serious games.2,51
While the majority of games in this review are applied to behavioral challenges consistent with major healthcare priorities (e.g., reduction in rates of obesity), they typically aim to affect change by conveying knowledge. For instance, Viggiano et al. 20 targeted lifestyle changes in children by conveying knowledge about healthy diet and exercise. Our meta-analysis showed that board games resulted in significantly more knowledge attainment than other nongame conditions, consistent with findings of meta-analyses in the realm of digital game-based learning.52–55 This—along with the null or very small effects measured in self-efficacy and attitudes/beliefs—suggests that the primary value of board games thus far is shown when applied to behavioral problems arising through lack of knowledge or difficulty in communicating health-related concepts, rather than those characterized by the persistence of negative behavior in the presence of knowledge. Even Khazaal et al., 43 who did not measure knowledge directly, aimed to change smoking behavior through the conveyance of facts about smoking (e.g., costs associated with addiction, biological effects of smoking). However, it should be noted that the lack of analyses of board games applied to situations, wherein negative behavior persists in the face of knowledge precludes conclusions regarding their suitability in these contexts.
Overall, and in many cases as a result of increased knowledge through gameplay,20,33,34,41–43,46 health-related behavioral outcomes (e.g., smoking cessation, diet, and lifestyle changes) showed a small-to-moderate postintervention effect in favor of board games, particularly in the self-reported behavior category. This is consistent with studies of videogames targeting health behavior change that generally show positive effects.2,56 However, self-reported measures of behavior are particularly vulnerable for bias because they can be associated with social stigmas (e.g., around diet and exercise).57,58 Unfortunately, only a single study in our review included an objective measure of behavior. 38 Ultimately, downstream biological health/patient outcomes, such as reduced zBMI scores, are the desired objectives of behavior-targeting games and indicate real-world behavior change; our synthesis of biological health outcomes demonstrated small-to-moderate effects in this category, highlighting the potential of board games to facilitate real-world change, although only three studies included such outcomes. A meta-analysis investigating the synthesized effects of active videogames on health outcomes also showed small to large effects. 59
While our analyses suggest that board games can be effective at increasing knowledge, changing behavior and, in turn, affecting biological outcomes, the evidence for improvement of self-efficacy was not significant; this is inconsistent with a meta-analysis of active videogames that showed moderate effects on self-efficacy, 59 perhaps because players of active videogames experience the behavior first-hand, instead of receiving knowledge about the behavior to apply at a later time, like in the reviewed board games. Furthermore, we can fairly confidently conclude (due to the low RoB and significant synthesized effects) that board games affect attitudes and/or beliefs very little, which contrasts stronger findings in the digital game-based learning literature. 60 Lastly, there is insufficient evidence to conclude whether board games may impact other outcomes in health and medicine, such as anxiety, social functioning, and executive functioning, with only single studies covering these themes. However, game-based studies of other “nonboard” games not included in this review (e.g., Mahjong) have shown some promise in the realm of executive functioning.61–63
Limitations
This meta-analysis is limited by heterogeneity of outcomes used to evaluate the board games, poor methodological design of many of the studies, and the small sample size/inadequate power of most of the included studies. Synthesizing highly heterogeneous studies (note the high I2 values for our various syntheses), is a clear weakness in this meta-analysis. However, heterogeneous outcomes are often examined to come to higher-order generalizations about a topic in question.29,30 In this case, we were interested in examining whether board games could be used as a tool to impact outcomes in the domain of health. Therefore, the results should be used as a general summary of the effect across the educational board game literature in different outcomes. Furthermore, because of the limited number of comparisons within each outcome category, we were unable to perform moderator analyses to investigate possible confounding effects of, for example, total play time, primary game mechanic (e.g., question-and-answer vs. action-and-consequence), or target audience (e.g., adults or children). It should finally be noted that, since studies with larger samples (and therefore less variance) tended to contribute more toward synthesized effects (e.g., Viggiano et al. 20 accounted for ∼40% of the weight in self-reported behavior; Khazaal et al. accounted for 54% of the weight in attitudes and beliefs), our reported effects may be more representative of the types of board games or play contexts found in these more robust studies.
Another limitation of the data synthesis is that, while we examined outcomes from studies with control/comparison groups, some of these included research designs that did not randomize participants to treatment and control groups. The randomized trial is considered the Gold Standard for determining causality in evaluating the impact of interventions on outcomes. 4 Until results from larger and higher quality, randomized, controlled trials of board game interventions in healthcare are available, the research results presented in this review represent the best strategy for appraising the evidence, while considering the inherent bias in the studies evaluated.
A further limitation is that the findings reported do not consider preintervention results because (1) some studies did not include baseline measurements and (2) most studies did not report variance for pre to postintervention change, thus excluding pre–post improvement information from ES calculations; this precluded our ability to evaluate whether or not differences between treatment and control groups observed at the postintervention may have been related to preexisting differences at baseline. However, it should be noted that effects with baseline imbalances (or no reported baseline measurements at all) were excluded from sensitivity analyses as they fell into the high or unclear RoB categories. Finally, the findings from this study are also limited due to missing data from studies; there was missing data from 11/88 postintervention comparisons where the authors did not include enough information for ES to be calculated (all these studies are at an unclear to high RoB).
Despite these limitations, it should be noted that an overall strength of this review is that it synthesizes data across diverse populations to estimate the impact that board games have had on various health-related outcomes, which has not previously been done in the literature.
Future directions
Our suggestions based on our critical review of the studies are consistent with previous games for health guidelines that call for the use of randomized controlled trials with adequate sample sizes to clarify the causal role of the intervention's impact on outcomes.56,64 Studies should also aim to measure behavior through direct means or consecutively logged activity to prevent biases associated with self-reports and, when possible, include more objective biological outcomes (e.g., zBMI) to corroborate behavior findings in a standard way across studies.
Furthermore, as discussed above, a main finding of this review was that the majority of board games targeting health-related behaviors did so through conveying new knowledge. Future research might investigate whether a board game might be effective in changing persistent, negative behaviors in the presence of knowledge.
Finally, a qualitative interpretation of the included studies would suggest that board games integrating a question-and-answer mechanic (i.e., trivia genre; a popular gaming pattern implemented by most of the included studies)19,31,32,36,42–45,47,49 have potential to lead to significant gains in knowledge; this is consistent with other research regarding the impact of self-testing strategies on knowledge consolidation in nongaming contexts.65,66 However, there appears to be a lack of board games that incorporate learning and gaming mechanics in more complex ways (e.g., through action-and-consequence),20,33,34,43 which limits our understanding of the different ways board games can be designed to support learning. Future games as educational tools should attempt to integrate more complex design strategies and explore whether or not existing digital game design frameworks (e.g., Learning Mechanics-Game Mechanics model, or the Activity Theory Model of Serious Games)67,68 can be applied to justify design decisions and advance our understanding in this area. Moreover, game efficacy should be examined through studies designed to clarify whether mechanisms of the board game itself (e.g., cooperative or competitive) or the context of its delivery (e.g., in a clinic, in a school setting) is responsible for the impacts observed in carefully designed studies; while such investigations are inherently more difficult to perform, the importance of asking more design-oriented questions is well recognized.53,69
Conclusion
In sum, this systematic review updates and extends previous reviews of board games for health. Although the findings of this meta-analysis are limited, given the current state of evaluations of board games for health in the literature, they do show preliminary evidence for the use of board games to improve knowledge in health outcomes. Future efforts to develop board games should focus on directly targeting behaviors related to downstream biological health outcomes, exploring alternative game design strategies to the trivia-genre, and evaluating board game interventions using rigorous scientific methods. Once knowledge about the overall efficacy of board games is better established, healthcare professionals, patients, students and community members can benefit from this engaging approach to promote health and medical outcomes.
Footnotes
Acknowledgments
The authors wish to thank Ouarda Yvray for helpful comments on the review. This work was supported by Pfizer and the Social Sciences and Humanities Research Council of Canada through a Michael Smith Foreign Study Supplement.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.