
Abstract
Abstract
The increase in autism spectrum disorder (ASD) population triggers a deep concern within public health. This alarming trend stresses the need for the development of effective strategies that might aid with this growing population. Exergaming has several advantages as an ASD intervention, such as flexible play, a private space for exercise, and diverse types of physical activity. The study aims to analyze the effectiveness of exergaming interventions on individuals with ASD. The systematic review was conducted in accordance with PRISMA guidelines. Studies which employed exergaming interventions on individuals with ASD were considered for inclusion. Exergaming-related changes in participants' physical and cognitive functions were the main interest of the current review. Ten articles satisfied the predetermined eligibility criteria. Thematic coding categorized the main outcomes into two higher-order themes and five subthemes. The higher-order themes were physical performance and cognitive performance. The emerged subthemes were physical fitness, motor performance, intensity of physical activity, executive function, and self-perception. Following exergame interventions, individuals with ASD indicated significant improvements in physical fitness, executive function, and self-perception. Exergaming also increased participation in moderate-to-vigorous physical activity. In contrast, exergaming indicated small impact on emotional regulation and did not provide adequate opportunities for motor skill development. It is worth noting that only one randomized controlled trial was included in the current review. Future research would require more rigorous study designs to provide reliable evidence on the effectiveness of exergaming interventions for individuals with ASD. Exergaming interventions lead to improved physical and cognitive functions in individuals with ASD. It is suggested that exergaming be used as a feasible supplement to traditional physical activity programs for individuals with ASD.
Introduction
A
Recent research has acknowledged that individuals with ASD experience decreased executive function,9–11 poorer motor skill performance,12–16 and declined physical fitness due to a relatively inactive lifestyle.17–20 Although no single best treatment has been developed, several intervention programs (e.g., speech/language therapy, occupational therapy, physical therapy, and behavioral intervention) have shown positive effects in clinical practice. One such therapeutic intervention, aerobic exercise, has been effective in helping children with ASD control aggression, stereotypical behaviors, self-injury, and repetitive behaviors. 21 For example, in one particular study it was observed that children significantly increased correct responses to teacher directives after conducting a 15-minute aerobic exercise. 22 Despite the effectiveness of aerobic activity, exercise therapy has a notable limitation. Motivating individuals with ASD to participate in physical activity is not easy due to considerable barriers in the traditional activities. 23 Individuals with ASD often avoid physical activity in a group setting as they are hesitant to exhibit motor impairments or the inability to perform complex movements in front of peers. 24 Exergaming, a form of digital gaming, which requires physical movement to play the game, 25 perhaps is a feasible option to increase physical activity in individuals with ASD as it can be performed in a nonthreatening environment. 26
As a potential supplement to traditional physical activity programs, exergaming intervention may produce positive effects on physical and cognitive functions for people with ASD. Exergames exhibit advantages in practical applications. For example, exergaming systems are engineered to allow physical activity in relatively confined spaces. This helps individuals to be physically active at home or school. 27 Exergames are also relatively inexpensive and are available to the general public. In a survey involving 215 families across the United States, 82% of families with children diagnosed with ASD own at least one exergaming system. 28 Research has shown an increased interest in applying exergaming interventions to promote physical activity for various populations. Reviews on exergaming research with children, adolescents, and older adults are readily available25,29,30; however, no such review exists for the effects of exergaming on individuals with ASD. Better understanding the role of exercise through videogame platforms will provide practitioners meaningful information as to when exergaming can be used within the ASD population. Therefore, it is our aim to provide evidence-based recommendations and identify areas for future research based on the findings within this review.
Methods
Registration
This systematic study was registered in PROSPERO for two main reasons: (1) avoid duplicated systematic reviews; (2) and demonstrate the transparent review process to minimize bias of studies. 31 The registration number is CRD42017064368.
Literature search
The systematic review was conducted in accordance with PRISMA guidelines (Supplementary Data are available online at www.liebertpub.com/g4h). Five electronic databases (Google Scholar, PubMed, Web of Science, PsycINFO, and Research Autism) were utilized to search for literature. To identify relevant articles for our primary purpose the search focused on four categories; treatment, physical behavior, cognitive behavior, and population. The following combinations of terms were used to search for articles across all databases: “exergam* OR active video gam*” AND “physical activity OR exercise” AND “cognitive function OR cognition” AND “autism spectrum disorder OR autism OR ASD.” Following article identification, a 2-step screening process was utilized to select articles that met our inclusion criteria. The initial screening removed abstracts, conference reports, duplicates of articles, and articles not relevant to our purpose. Next, a full-text evaluation was conducted to assess inclusion eligibility for the remaining articles. Two authors worked independently and selected articles that met the predetermined inclusion criterion. Any disagreement on whether an article should be included was reported to the other authors and resolved following discussion.
Studies that met the following inclusion criteria were included in the review process: (1) peer-reviewed article published in English from 2000 to 2018; (2) subjects diagnosed with ASD by a physician; (3) study utilized some form of exergaming as an intervention; (4) measurements were obtained on cognitive performance, social–emotional behaviors, or physical ability tests.
Data items and synthesis
Data extracted from each study were considered essential to investigating the effects of exergaming on individuals with ASD. Basic details were derived from information on author(s), year of publication, study design, sample size and attrition rate, participant age, and exergaming platform. We also made sure to note the frequency in which the exergaming intervention was applied and the duration of each meeting. Exergaming-associated outcomes were summarized as key findings which provided evidence-based suggestions or implications for researchers and health professionals. See Table 1 for a detailed list of each study.
RCT, randomized controlled trial; TD, typically developing; ASD, autism spectrum disorder; DDR, dance dance revolution; MVPA, moderate-to-vigorous physical activity; MET, metabolic equivalents.
Thematic coding is a commonly-used analysis in qualitative research. It involves identifying common themes and establishing a framework of thematic ideas. 32 The coding process includes three stages: identifying key words or phrases from the text; generalizing the key words into descriptive themes; and developing analytical themes by thorough and interpretative coding.33,34 Thematic coding enables researchers to integrate primary findings and data of the studies in a transparent way and facilitates the process of producing new concepts and hypotheses. 33
In the first step of extracting key words and phrases from the included studies, raw codes were derived from the investigated functions (e.g., object control skill and working memory) in each trial. Next, the outlined codes were categorized into descriptive themes, such as motor skills and executive function. Further analysis and interpretation generalized the descriptive themes into higher-order themes related to physical and cognitive effects associated with exergaming interventions. See Table 2 for the hierarchical structure of the themes.
Numbers in parentheses represent the number of articles that referred to subthemes or higher-order themes.
BMI, body mass index; %MVPA, percentage of time in moderate-to-vigorous physical activity; PMSC, pictorial scale of perceived movement skill competence.
Quality assessment
The Physiotherapy Evidence Database (PEDro) scale, which was developed upon the Delphi list,35,36 was used for quality assessment. The PEDro scale has been found to be a reliable and valid instrument for assessing the methodological quality of clinical trials. 37 The scale consists of 11 criteria concerning the internal validity of a clinical trial and the statistical information reported.38,39 According to the Physiotherapy Evidence Database, the median PEDro score is 5 on a scale of 0–10. Previous research has pointed out that it is difficult to use a double-blind procedure in exercise interventions, thus limiting the maximum possible score on the PEDro scale. 40 Due to this limitation, any trial scoring 6 or above is considered high quality. 41 A score of 4 or 5 is defined as moderate quality and a 3 or below suggested low quality. Two authors independently conducted quality assessments using the PEDro scale and provided an overall rating based on the total score of each study. A third author helped resolve disagreements when necessary. Table 3 summarizes quality assessments for the included studies.
EC, eligibility criteria; RA, random allocation; CA, concealed allocation; SAB, similar at baseline; SB, subject blinded; TB, therapist blinded; AB, assessor blinded; DR, dropout rate; ITA, intention-to-treat analysis; BC, between-group comparison; PM, points measures; OSQ, overall study quality.
Results
Study selection
The initial database search resulted in a total of 1024 journal articles. A screening of titles and abstracts excluded 973 items because of duplicates (N = 390) and irrelevant topic (N = 583). In the full-text analysis, 41 of the remaining articles were removed due to the following reasons: abstracts (N = 10), book chapter (N = 1), no behavioral or cognitive outcome (N = 21), not related to the population with autism (N = 2), not peer reviewed (N = 1), and/or no exergaming intervention (N = 6). The screening process retained 10 articles eligible for further qualitative analysis. Figure 1 presents the screening process for eligible studies.
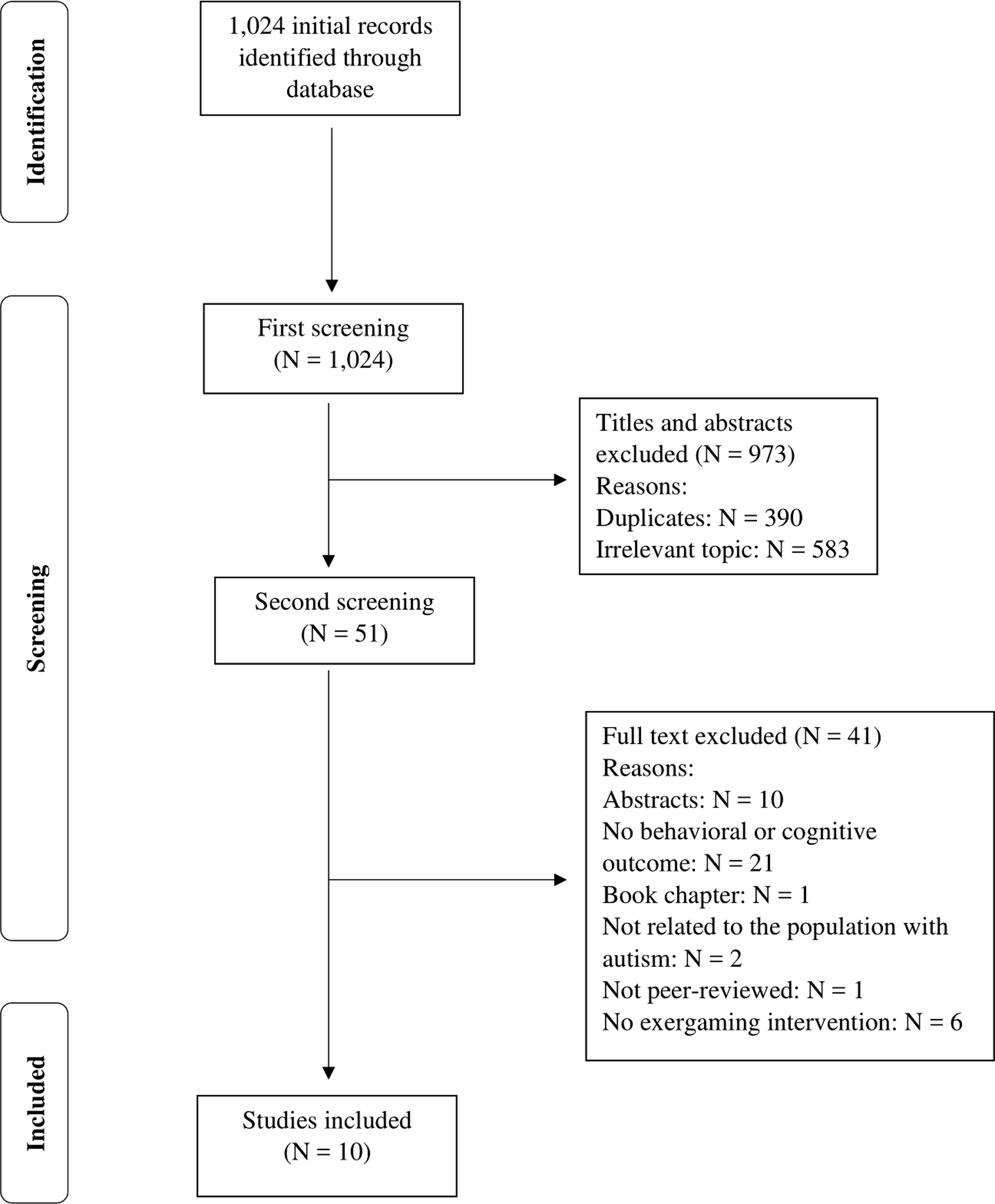
Flowchart of the inclusion process.
Study characteristics
Our review of the literature indicated an increasing interest in exergaming interventions for individuals with ASD. 42 The United States produced the most research studies (N = 7) in this field, whereas Australia (N = 1), Mexico (N = 1), and the UK (N = 1) each had one publication. Three types of research designs were used in the included studies. Interventions using pre- and posttests to measure the effectiveness of the applied intervention were utilized the most (N = 5).43–47 Case–control studies (N = 3) involved the observation of typically developing (TD) and ASD group.42,48–50 By examining exergaming-associated effects on each group, researchers may better understand if individuals with ASD benefited from an exergaming intervention as much as their typically developing counterparts. Only one study was randomized controlled trial (RCT). 26 In this study participants with ASD were randomly assigned to either control group or an intervention group. It was assumed that any group differences observed during the posttest were due to the intervention employed.
Sample sizes ranged from 5 to 100 individuals and the attrition rate varied between 0% and 15.5%. Participants were mainly recruited from local autism programs so that researchers could identify eligibility based on formal diagnoses from physicians. Participants' age ranged from 5 to 21 years, suggesting that the current body of literature focused more on children and young adults than adults and older adults. Most interventions ranged from 3 to 10 weeks in duration with the exception being the RCT, which lasted approximately 1 year. 26 The exergame platforms utilized in the interventions, included Xbox Kinect, Nintendo Wii, DDR, Makoto Arena, FroggyBobby, and Cybercycling.
Quality assessment for eligible studies
Three of the reviewed studies were considered by the PEDro scale to be high in methodological quality since the protocols met six or more defined criteria. All studies within this review included their eligibility criteria for recruitment and kept high retention throughout the intervention program. The criterion of PEDro for intention-to-treat was satisfied for all studies as they provided adequate evidence that subjects received the treatment as prescribed. 39 Common limitations which decreased methodological quality included the lack of random placement in most interventions and the lack of necessary procedures of blinding practitioners and researchers to the groups. The limitations may increase the risk of bias in participant selection and assessment. In addition, the effect sizes were only reported in five of the articles which made it difficult to conduct a statistical analysis on the magnitude of the intervention effects. Table 3 highlights the PEDro scores for each study included in this review.
Synthesis of results
According to the primary outcomes measured in the reviewed literature, we identified 16 raw codes and five subthemes. Further analysis generalized the subthemes into 2 higher-order themes, cognitive and physical outcomes. Physical outcomes addressed changes in physical fitness, motor skill performance, and intensity of physical activity during game play. Cognitive abilities were assessed through executive function testing and self-perception. Eight of the included studies measured physical outcomes, whereas six investigated cognitive performance following intervention.
Summary of Evidence
Physical outcomes
Three studies examined effects of exergaming interventions on physical fitness, which was measured by six tests on body composition, speed, endurance, strength, and flexibility. Dickinson and Place 26 examined the effects of a Nintendo Wii intervention that was performed three times per week during three academic semesters. They reported a series of statistically significant improvements in those that participated in the exergaming intervention over a control group. These improvements included a decreased body mass index (BMI), enhanced performance in speed and agility, increased broad jump distance, strengthened aerobic capacity, and increases in sit-up performance. Specifically, BMI (a measure of body fat based on an individual's height and weight) was reduced from an average of 20.1%–19.8% (P < 0.001). Participants were able to complete a 10 × 5 m shuttle run within an average of 68 seconds in the posttest as opposed to 92 seconds in the pretest (P < 0.001). Broad jump score increased from 80 to 92.5 (P < 0.001), suggesting an improvement in explosive strength. A multistage progressive shuttle run, also known as bleep test, is a measurement for aerobic capacity. Participants' performance improved from an average score of 3 in the pretest to 4.5 in the posttest (P < 0.001). Sit-up performance also improved from an average of 10 during a 15-second period to 13 (P < 0.001). The flexibility score increased following intervention but the change was not significant. The control group showed improved flexibility (P < 0.05) but increased BMI (initial score = 20.2; postintervention = 21.5, P < 0.001) and performed slower (increased time) on the shuttle run (initial score = 84.5; postintervention = 90, P < 0.001).
Two studies utilized Makoto arena, a speed-based exergame, as an intervention for individuals with ASD.43,44 A Makoto court consists of three metal beams arranged in an equilateral triangle on the floor. Participants need to identify a target light, which randomly appears on one of the beams and then touch the target as fast as possible. Hilton et al. 44 used the Makoto arena three times a week for 10 weeks, whereas Hilton (2015) 43 allowed participants to choose the frequency of the 30 intervention sessions. The 30 sessions were completed between 6 and 10 weeks. Positive effects of exergaming were observed on participants' strength and agility in a series of tests such as one- and two-legged side hop, shuttle run, and stepping over a balance beam. The improvements were significant in the posttests and suggested moderate-to-large effect sizes.43,44 Along with Dickinson and Place's research, 26 such results substantiated exergaming as an effective approach to improving physical fitness for people with ASD.
Motor skills were assessed by fine manual control 43 and object control skills. 50 Tests for fine manual control included transferring pennies into a box, sorting cards, a pegboard task, and stringing blocks. The number of correct performances during a 15-second trial was reported as the test score. 43 Participants indicated slightly poorer performance in fine manual control following the intervention; however, the results were not significant (initial score = 39, postintervention = 38, P > 0.05). Edwards et al. 50 examined exergaming-related impacts on individuals' object control skills. A set of tests on ball skills, such as dribbling, catching, throwing, kicking, striking, and golf skills were conducted to assess an individual's object control performance. Participants received 1 point if a predetermined criterion was performed or 0 if a criterion was not successfully performed. Total points provided an overall evaluation of one's actual skills. Children with autism (N = 11) and their typically developing (TD) peers (N = 19) participated in a total of 6 intervention sessions. The actual skill scores in the posttest did not improve in either group. The result suggested that playing exergames might not facilitate acquisition of actual motor skills. 50
To investigate whether exergaming could provide adequate physical activity for people with ASD, researchers utilized energy expenditure and percentage of time in moderate-to-vigorous physical activity (%MVPA) to measure physical activity intensity.47–49 Getchell et al. 48 examined energy expenditure of 15 participants with ASD as well as 15 individuals without ASD performing 20-munite bouts of running, walking, DDR, and various Nintendo Wii Games, including Wii Fit and Wii Sport. Energy expenditure of the ASD group was highest in running (136 kcals), followed by walking (98 kcals), DDR (65 kcals), Wii Fit (53 kcals), and Wii Sport (27 kcals). A comparison between the ASD group and the control found no significant difference in the amount of energy expenditure during the gameplay, except for Wii Fit, in which the ASD group indicated significantly higher level of energy expenditure (P < 0.05). Likewise, Jozkowski et al. examined 5 participants playing Xbox for 30 minutes in each session. 47 The researchers found an average energy expenditure during gameplay from 5.77 kcals/min to 7.11 kcals/min (median = 6.07 kcals/min). The energy expenditure rate reported in the study suggested that the 30-minute exergaming session at the current level of physical activity intensity would contribute significantly to the 150–400 kcal daily energy expenditure recommendations. 51
Percentage of time in MVPA is another critical assessment of physical activity intensity. During 20-minute bouts of exergaming activities, participants with ASD spent 76% MVPA in DDR, 33% in Wii Fit, and 26% in Wii Sport. The percentages accounted for approximately 15, 6.5, and 5 minutes, respectively. 48 Another two studies employing Xbox Kinect reported higher percentage of time spent in MVPA.47,49 Jozkowski et al. examined 5 ASD participants and found that the percentage of MVPA ranged between 82% and 94% (median = 89%). This was approximately 24–28 minutes in MVPA during a 30-minute session. 47 Golden and Getchell also compared the percentage of time spent in MVPA between ASD group and TD group while using the Xbox Kinect. Time spent in MVPA was 76% in the ASD group and 80% in the TD group, which roughly equated to 11–12 minutes out of a 15-minute gameplay. No significant difference was found in respect to the percentage of MPVA between the two groups (P = 0.27), suggesting that individuals with and without ASD engaged in a similar level of physical activity intensity during the gameplay. 49
Cognitive outcomes
Cognitive outcomes after exergaming interventions contained two subthemes–executive function and self-perception–which were further divided into five items. Two studies assessed executive function with the Behavior Rating Inventory of Executive Function (BRIEF). BRIEF is a standardized rating scale developed to measure executive functions, including working memory, initiation, organization, planning, and task monitoring. 52 Hilton et al.43,44 observed significant improvements in metacognition among ASD participants following 10 weeks of interventions through Makoto Arena. Both studies reported moderate-to-large treatment effects. Anderson–Hanley 42 examined changes in working memory by means of the Digit Span Backward test, which required participants to listen to a string of numbers and repeat them in reverse order. Participants repeating more numbers receive higher scores which suggest better working memory capacity than those with lower scores. While the Digit Span Backward score for the control group declined from an average score of 2.7 in the pretest to 2.1 in the posttest, the score after the exergaming intervention increased from 2.5 to 2.8. The reported improvement in performance for the exergaming group was significant (P = 0.03).
Task-switching refers to the ability of transferring from one task to another. 43 One study examining task switching used the Color Trials Test, in which participants were asked to connect two sets of numbers from 1 to 25, with one set highlighted in pink, whereas the other set was in yellow. Participants attempted to complete the task as fast as possible with a shorter completion time indicating better cognitive function in task switching. Participants following a DDR intervention spent less time completing the Color Trials Test during the posttest than the pretest (initial time = 152.1 ± 50.9; postintervention = 146.6 ± 65.8), but the difference was not significant. 42 Task-switching capacity was also one of the items examined in the BRIEF scale. Hilton et al. 44 identified reduced scores in the posttest (initial score = 63.86 ± 10.22; postintervention = 60.14 ± 10.27), which suggested positive effects after the intervention. The change in the task-switching capacity had a moderate-effect size (d = 0.36) but failed to reach significance (P > 0.05).
Individuals with ASD have difficulty in producing, planning, and managing behaviors. The presence of repetitive, purposeless behaviors is considered a symptom of autism. 53 One study compared repetitive behaviors in ASD individuals following an exergaming intervention and those with no intervention (control). In a 5-minte observation period, repetitive behaviors decreased significantly in those that received a 20-minute exergaming session compared with the control group that watched TV for 20 minutes. The number of repetitive behaviors observed in the control increased from 16 to 19.5, whereas repetitive behaviors after the intervention decreased from 14.9 to 10.8 (P < 0.001). 42 In another study, examining the effects of children with ASD, it was observed that aimed limb movement significantly increased while aimless limb movement decreased (P = 0.032) following twelve 30-minute exergaming sessions over 6 weeks. 45 The participants only completed 58% of aimed limb movements in the first exergaming session while completing 96% in the last session. This increase in purposeful movements suggests better behavioral regulation in children with ASD.
Emotional regulation is important in social communication and interaction. People with ASD may display deficits in developing appropriate relationships with peers and others due to the poorly modulated emotional responses. Three of the included studies investigated exergaming impacts on the emotional regulation of individuals with ASD. Hilton et al. 44 identified positive changes in emotional control as the BRIEF score decreased from pre- to posttest (pretest M = 59.57 ± 7.91; posttest M = 58.71 ± 10.92). However, the difference between the pre- and posttest was not significant (P > 0.05), and the size of the intervention effect was small (d = 0.11). Another study examined participants' emotional expression across 12 exergame sessions. 45 Although positive emotions (e.g., joy and interest) remained above 90% of emotional expressions in each session, no significant change was found over the 6-week intervention. The result suggests that exergaming may be effective in maintaining positive emotional expression throughout use. Communication and interaction during exergaming between three dyads of children with ASD and their siblings were examined to identify potential changes in emotional expression. 46 Researchers coded the participants' interactions as positive affect, conversation, or aggression. The results were inconsistent given that only one dyad exhibited increased positive affect during the exergaming sessions, whereas the other dyads displayed either unchanged or worse behaviors.
Perceived competency of performing motor skills was investigated in one research study. Researchers utilized the Pictorial Scale of Perceived Movement Skill Competence to assess participants' perceived motor skill competence at baseline and postintervention test. 50 Exergaming sports, such as baseball, football, tennis, volleyball, soccer, and bowling were available to choose based on participant preference. Results indicated a significant increase in perceived motor skill competence after the exergaming sessions (initial score M = 27.63 ± 3.85; postintervention M = 29.45 ± 3.91, P = 0.044). A follow-up interview indicated increased willingness to engaging in physical activities in accordance with the improved perception of motor skill performance.
Discussion
Previous research has identified health benefits through exercise for individuals with ASD.21,54 Unfortunately, there are numerous challenges during exercise that individuals with ASD face. For example, the inability or difficulty to perform complex movements may prevent people with ASD from continuous participation. 48 It was found that people with ASD were inclined to prioritize videogames as a recreational activity and play with high frequency.55,56 As such, a combination of exercise with videogames platforms (exergaming) may be a particularly appropriate approach to providing opportunities for physical activity in the ASD population. Some positive features of exergaming include enjoyment, interaction with others, and whole-body movements. These features could stimulate engagement in moderate-to-vigorous physical activity throughout the life course; thus reducing health risks such as obesity, cardiovascular diseases, and type 2 diabetes. 48 In accordance with the increased interest in the effects of the exergaming on individuals with ASD, this systematic review was conducted to synthesize evidence from existing literature on the physical and cognitive outcomes following exergaming interventions. It was also our aim to provide suggestions for future research.
Exergaming may be an appealing supplement for increasing daily activity levels for individuals with ASD. In the included literature, participants using Xbox Kinect spent 76%–94% of play time in moderate-to-vigorous physical activity.47,49 According to the American College of Sports Medicine (ACSM) national guidelines it is recommended that individuals take at least 150 minutes of moderate-intensity aerobic exercise per week. 57 Three to four 1-hour exergaming sessions will contribute to most, if not all, of the recommended physical activity levels each week. Also, the reviewed literature reported significant improvements in most physical and cognitive functions. The findings were consistent with previous studies which applied exercise therapy on people with ASD,54,58,59 suggesting that exergaming could be an effective addition to standard exercise interventions.
Another notable effect of exergaming was related to perceived skill performance in people with ASD. 50 The improved perception of motor skills implied enhanced motivation to engage in physical activity. Despite the positive outcomes associated with exergaming interventions, it is important to note that motor skill development and enhanced emotional regulation were not substantiated by the reviewed literature. We suggest that those whom may prescribe exergaming to autistic patients be cautious with their expectancies on the benefits to emotional regulation and/or the development of motor skills. However, participants in three different studies did show minor changes in emotional regulation as well as behavior management.44–46 This result is contrary to previous research, which identified improved social behavior as well as expressions of positive affect in videogame play.60,61 The discrepancy may be attributed to the dose-dependent effects of exergaming interventions. For example, one of the reviewed studies found no significant differences following an exergaming intervention of 323 minutes, whereas another reviewed study that used an exergaming intervention of 480 minutes found significant improvements in TD children. 62 It is possible that durations of the interventions in the reviewed studies were not sufficiently long enough to produce significant effects on emotional regulation. Additionally, exergaming might not provide adequate opportunities for participants to correctly perform the targeted skills.44–46,50 One study in which exergaming sessions were led by an experienced instructor did identify significant improvements in motor skill proficiency in typically developing children. 62 This finding highlights the necessity for future research to integrate structured skill instructions into an exergaming intervention with the ASD population. For example, research has demonstrated that instructional video modeling has been useful for motor skill development with ASD children.63,64 This future line of inquiry may lead to the implication that providing more structured instruction may benefit individuals with ASD in developing various motor skills.
The limitations of the systematic review stemmed from the limited number of RCT (N = 1). Well-designed RCTs follow specific procedures in randomization. This randomization reduces potential bias in the selection of participants and the placement in various conditions, which strengthens the reliability of the evidence. 65 The pre/posttests included in this systematic review may raise questions as to interpretation of the results. Four of the pre/posttest studies involved only a treatment group and lacked a control group. It is difficult to know if the reported improvements in the posttests are attributed to the intervention or are a part of natural development. Additionally, the included studies varied in outcome measures, study design, and quality. Increasing the number of studies on the effects of exergaming would significantly strengthen our current knowledge and lead to a better understanding of the response-dose relationship. In addition to the limitations of the systematic review, there were a few common limitations in the included studies. First, seven studies mentioned small sample sizes which limited generalizability of the results.42–44,46,47,49,50 Second, often times the research did not report effect sizes which is increasingly important when working with small sample size.26,42–44,50 Third, most interventions in the review lasted 10 weeks or less. Longitudinal assessments of the physical and cognitive effects of exergaming interventions would prove valuable.
In conclusion, exergaming may be considered an effective addition to standard physical activity treatment on individuals with ASD. The included literature indicated that exergaming interventions produced positive outcomes in physical fitness, executive function, and self-perceived motor skill performance. By playing exergames, participants received opportunities of engaging in moderate-to-vigorous physical activity during each session. However, effects on emotional control and motor skill development were not significant. Health professionals should be careful when attempting to help people with ASD to promote their emotional regulation and motor skills by means of exergaming interventions. Only examining one RCT is a significant limitation of the literature review. Rigorous studies are necessary to provide a better understanding of the effects of exergaming interventions for individuals with ASD. Given the limitations of the current studies, future research should strive to provide rigorous evidence established by RCTs, report effect sizes of treatment, and investigate longitudinal effects of the intervention.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.