
Abstract
Abstract
Objective:
To evaluate the effects of an educational board game on heart failure (HF) patients' knowledge and self-care behavior.
Methods:
In this randomized controlled study with a follow-up of 3 months, 76 patients with HF with reduced ejection fraction, who had been enrolled in our multidisciplinary HF program, were divided into two groups. During their follow-up appointment at the HF clinic usually 2 weeks after discharge, the interventional group participated in an HF educational board game conducted in Thai language, while the control group received the usual care including standard education. The primary outcome was the change of score achieved in the specialized HF knowledge and self-care behavior assessment.
Results:
In the intervention group, the knowledge and self-care behavior significantly improved (all P < 0.001), whereas both scores were unchanged in the control group (P = 0.09 and P = 0.21). Mean score change for knowledge and self-care behavior showed greater improvement in the intervention group when compared with the control group (P < 0.002 and P < 0.006).
Conclusion:
Participation in an interactive educational board game resulted in an increase in the HF patients' knowledge and self-care behavior.
Practice Implications:
An interactive educational board game may be used as an alternative educational tool in HF patients.
Introduction
H
The prevention of HF exacerbation depends on suitable self-care behavior and receiving continuous healthcare. Educating patients and their relatives on limiting high-sodium diet consumption, regular weight monitoring, assessment of excess fluid, and adjustment of diuretic dose by themselves could prevent the aggravation of HF and reduce readmission rates.4,5 Thus, an effective educational program provided by a healthcare team is crucial to improve the patients' outcome.6,7
The current pattern of enhancing knowledge for HF patients is a one-way communication technique through which nurses provide information to patients. This is a weak link as it does not stimulate the patients' interests and memories, making this way of enhancing knowledge unsuccessful. Various styles of giving knowledge need to be improved by developing interactive games, particularly learner-based games. 8 The major advantages of interactive games are patient participation and engagement of the learners. By playing and having fun at the same time, learners can meaningfully develop their learning during or after playing the games. Gaining knowledge through games is based on group process learning, resulting in the exchange and interaction between instructors and patients, and among the patients. This style of learning has been proven to be fun and interesting.9,10 Furthermore, it stimulates the patients' interest and memory and helps them to develop knowledge and skills of self-care, and thus potentially resulting in a decrease in readmission rates.
In this study, the researchers were eager to learn about the efficacy of using interactive educational board games to provide knowledge to HF patients. Hopefully, this education method may promote patients' self-care, eventually reducing the burden of HF rehospitalization, reducing costs, and improving the quality of life. Thus, the primary objective was to compare the effects of both an interactive educational program and a standard educational program used to improve the knowledge and self-care behaviors of patients with HF.
Materials and Methods
This was a prospective, randomized study with a 3-month follow-up. Written informed consent was obtained from each patient and the study protocol was approved by the Research Ethics Committee of Faculty of Medicine, Chiang Mai University.
Participants in this study were patients diagnosed with HF and discharged from Maharaj Nakorn Chiang Mai Hospital for 2 weeks. Before they enrolled in the study, all participants received the standard education session at the time of hospital discharge. At the first follow-up at the HF clinic, which provided outpatient education, patients were screened and invited to participate in the study. The inclusion criteria were (1) being able to respond to the questions and (2) being willing to participate in the study.
Subjects were assigned by simple randomization into two groups, a control group and an intervention group. The intervention group received one session of the HF interactive educational board game, organized by the researcher in Thai language, which lasted for 30 minutes per round of playing. The group playing consisted of small groups, with three to four participants and/or a few caregivers in the groups. It was necessary to play board games 12 times to include all the 38 intervention participants in the study. The control group received the onetime usual outpatient education provided by the HF nurse, which did not include the researcher. The study questionnaires in Thai language were completed to assess their knowledge and self-care behavior at baseline before the educational session and at the 3-month follow-up (Fig. 1 and Table 1).
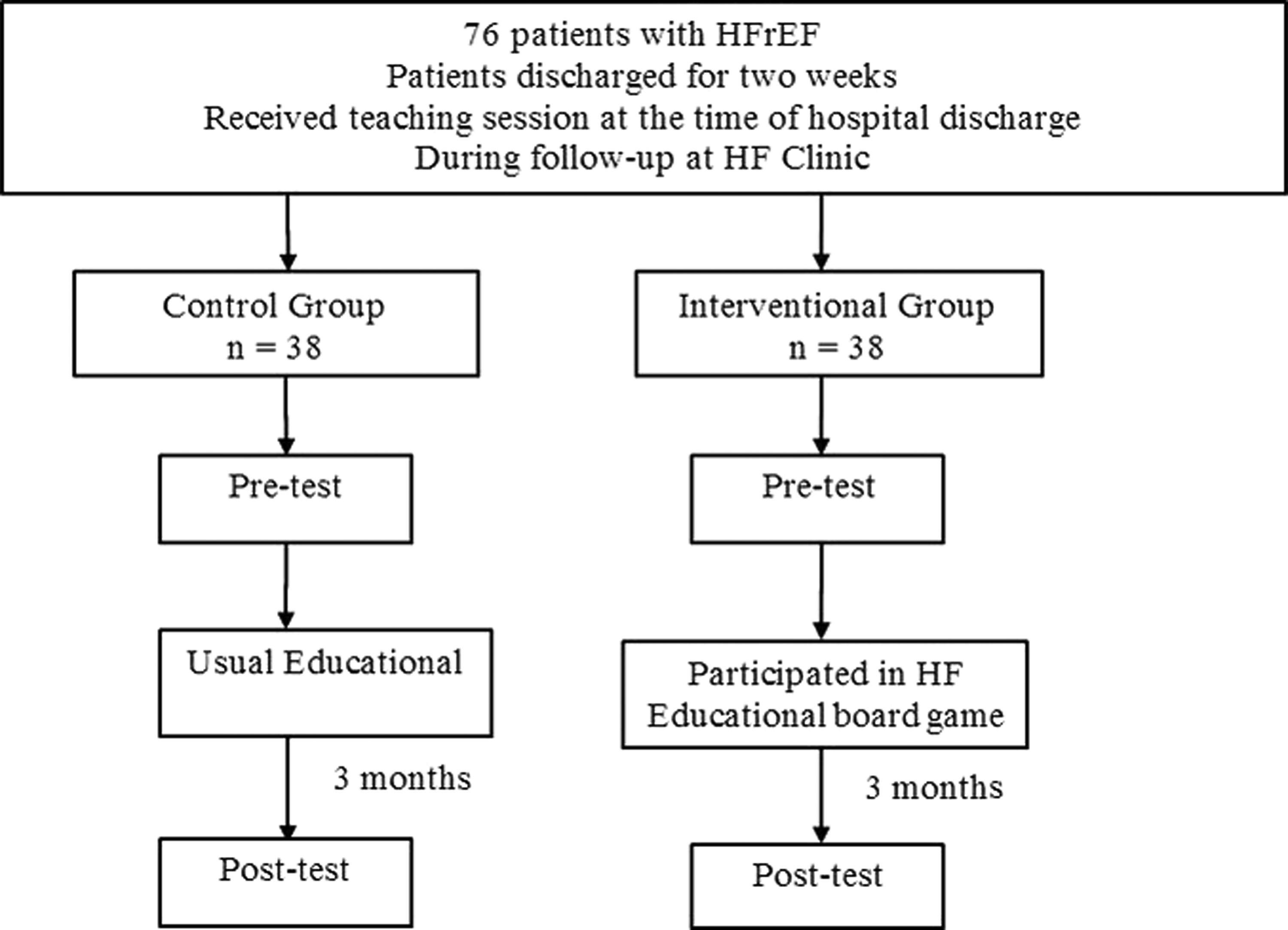
Flow diagram of the randomized controlled trial.
HF, heart failure.
Research Instruments
Interactive educational board game
The interactive educational board game used in our study was created by Patrick Jourdain, MD. The Servier (Thailand) Company Limited bought the copyright license for reproduction and distribution. The game contents were translated into Thai by Thai cardiologists and HF specialist nurses from four university hospitals. Some questions were modified to suit the lifestyle and culture of Thai people: for example, foods with added shrimp paste containing a large amount of salt should be avoided. True or false? Shrimp paste is a Thai flavoring. This HF educational tool aims to improve care for patients with an ongoing or stable medical condition. It teaches patients and/or their caregivers about the treatment of HF and gives advice regarding managing the disease in everyday life. Nurses were the ones who organized the game. A tool box contains a board, the rules of the game, specific “knowledge” cards, specific “role-play” cards relating to a situation that puts the patient at risk or that requires a particular reaction, 6 “player” counters, a 6-sided dice, and 50 colored health points. Written game instruction questionnaires and answers were provided. Game instructions were given by an HF specialist nurse with experience in HF patient's education (Appendix 1).
Standard outpatient education in HF clinic
The standard outpatient education in HF clinic was a one-on-one education session for patients and caregivers. The education topics included clinical presentation of HF, treatment, lifestyle modification, self-monitoring, and management of early symptoms.
Questionnaires
Self-response questionnaires were used to assess knowledge and self-care behaviors. All questionnaires were developed in Thai language through the review of relevant literature by researchers who did not participate in the game translation. The questionnaires were further validated by two consultant cardiologists, a nurse instructor, and two HF nurse specialists.
The knowledge element of the HF questionnaires included 28 itemized questions administered verbally or in writing to the patients. The format was True/False questions. Total scores ranged from 0 to 28. A higher score indicated a higher level of knowledge. The validity and reliability using Kuder-Richardson 20 for this questionnaire were 0.8 and 0.75, respectively. The self-care behavior part of the HF questionnaires included 25 item surveys with a 5-point Likert scale to measure the frequency of self-care behaviors. A Likert format was adopted for response alternatives (0 = never, 1 = rarely, 2 = sometimes, 3 = often, and 4 = always). The total score is the sum of the scores for the 25 items with higher scores corresponding to higher self-care levels. The validity and reliability using Cronbach's alpha coefficient for this questionnaire were 0.72 and 0.71, respectively (Appendix 2).
Data analysis
Cohen's statistical power analysis was used to determine the sample size as 34, but to cover for the possible dropout of 10% (4 patients), 38 patients were recruited for each group.
Questionnaires were collected anonymously and sorted by a concealed reference number. The outcome assessors were blinded to the assigned group.
Continuous data presented as mean ± standard deviation and compared between groups using Student's t-test. Categorical data presented as number (%) and compared between groups using the chi-square test.
A paired t-test was used to compare the differences between the pre- and postknowledge and self-care behavior scores in each group.
Student's independent t-test was used to compare the changes of score between groups.
A two-tailed P-value of less than 0.05 was considered statistically significant.
Results
Thirty-eight patients participated in the intervention group and 38 in the control group. The baseline characteristics are shown in Table 2 and the overall mean age was 58 years. Most subjects (77.6%) were male, 63.2% were married, and almost half of the patients (43.4%) had no education or completed education below the high school level. There were no statistical differences between the groups. There were no dropouts because participants were in the HF management program and the well follow-up.
NYHA, New York Heart Association.
We have found that the knowledge and self-care behaviors of the intervention group significantly improved (pre- vs. postknowledge score: 23.74 ± 3.03 vs. 26.11 ± 1.67, P < 0.001; pre- vs. post-self-care behavior score: 79.61 ± 11.83 vs. 87.89 ± 9.52, P < 0.001), whereas both scores were unchanged in the control group (pre- vs. postknowledge score: 24.05 ± 2.77 vs. 24.63 ± 2.64, P = 0.09; pre- vs. post-self-care behavior score: 79.37 ± 12.63 vs. 81.32 ± 11.01, P = 0.21) (Table 3).
Data presented as mean ± SD or N (%).
SD, standard deviation.
Moreover, the mean change of knowledge and self-care behavior scores was greater in the intervention group when compared with the control group (Table 4).
Discussion
In this study, an HF patient educational technique, using an interactive board game, resulted in better knowledge and self-care behavior improvement after assessing by questionnaires and comparing the results with the standard education. The card game contained questions regarding general knowledge of HF, food and water consumption, medicines, exercise, and self-monitoring for signs and symptoms of HF. While answering these questions, players could exchange their views with their peers while getting additional information from nurses via role-play, stimulated scenarios, discussion, and immediate feedback. The interactive board game could also help the patient to develop problem solving and communication skills, such as describing the symptoms more accurately, which would eventually help the patients to respond better to disease-related events. The method could also be adapted for other disease education programs that require optimal patient self-care.
Interactive education has been studied in people having various diseases, including acute and chronic conditions. The educational board game in public schools has improved knowledge about acute diseases such as dengue fever. 9 Similarly, the meta-analysis showed that the educational games can improve the level of knowledge and self-management in young people with chronic conditions. 11 In addition, games also improved diabetes-related knowledge, self-efficacy, communication with family and friends, self-care behaviors, and clinical utilization in young adults.12,13 Also, one study in older adults with HF showed that playing interactive digital e-health games resulted in improvement in HF self-management knowledge. 14
Compared with the videogame, there are fewer published studies using board games. In general, board games are low tech and easier to use and so can be seen as a more suitable activity for older population who are usually not “digital natives.” Therefore, we believe interactive board games may be applicable to a broader population; one in which the subjects were older or perhaps with a lower education level. Also, group interactive board games such as the one used in our study, where players are physically present, promote interpersonal interaction. This would allow more opportunities for knowledge and experience sharing and supportive encouragement among the members and the nurse conducting the game.
Interactive educational board games can be adapted in content and challenges related to the special diseases, local environment, as well as characteristics of patients and caregivers. In combination with an active learning processes, enhancing patients' engagement, and providing immediate feedback, educational board games can be a great tool for patient health education programs. An educational program increases patients' knowledge and understanding, treatment, and daily self-care and self-management in HF patients. The benefits of this educational game on outcomes should be further studied.
Limitation
The limitation of this study is the lack of reliability of self-reported self-care behavior measures. Patients may know the correct behavior, but one cannot assume that these behaviors were practiced unless directly measured. Also, retention of knowledge was not reevaluated. The benefit seen here may be weaned off after a certain period. To further the knowledge in this area, the next studies should explore the impact of board games on hard clinical outcomes, such as rehospitalization and mortality.
Conclusion
In a randomized controlled trial, we provided evidence that an interactive educational board game as a comprehensive educational program resulted in enhancing patients' knowledge and the self-care behaviors of HF patients compared with a traditional education approach.
Practice Implications
An interactive educational board game is an effective educational tool and may be used as an alternative educational method in HF patients. Being adaptable to any disease, patient characteristics, and local culture, educational games enhance patients' engagement in an active learning process. This educational method promotes patients' knowledge, self-care behavior, and hopefully improves outcomes in HF patients.
Footnotes
Acknowledgment
We thank all the staff in the Northern Cardiac Center and Division of Cardiology, Department of Internal Medicine, Faculty of Medicine, Chiang Mai University, for research and data cooperation.
Ethics Approval and Consent to Participate
The study protocol was approved by the Medical Ethics Committee of Faculty of Medicine, Chiang Mai University. Patients' informed consent was waived due to the nature of prospective study.
Author Disclosure Statement
No competing financial interests exist.
Appendix 1
An Interactive Educational Board Game for Heart Failure (HF). A board game using in our study was invented by Patrick Jourdain, MD * , and Servier (Thailand) Company Limited bought the copyright license for reproduction and distribution. The game contents were translated into Thai language and some questions were modified to suit lifestyle and culture of Thai people (by Thai cardiologists and HF specialist nurses).
Appendix 2
*
Heart Failure Department, CHR René Dubos, Pontoise and TPE Department, Paris Descartes University, Paris, France. E-mail: patrick.jourdain-mantel@wanadoo.fr