
Abstract
Abstract
Objective:
The main aim of this study was to prove the efficacy of an intervention based on board games on executive functions (EFs) and clinical symptoms in children with attention-deficit/hyperactivity disorder (ADHD).
Materials and Methods:
A nonblinded randomized controlled trial was conducted with a sample of children with a diagnosis of ADHD (diagnosed by psychiatrists and clinical psychologists in a mental health center). Children were randomly allocated by matching age and sex, into two groups: experimental EF training group (n = 13; mean [M]age = 9.46, standard deviation [SD] = 1.20; boys = 53.8%) or a wait-list control group (n = 14; Mage = 9.50, SD = 1.09; boys = 71.4%). Measures assessed individually at pretest, posttest, and follow-up intervention included EFs and clinical symptoms.
Results:
Analysis of covariance repeated measures analysis showed that linguistic short-term memory, F(1,28) = 7.45, p = 0.02, and conduct problems, F(1,28) = 12.51, p = 0.00, significantly improved with larger effects in the board games training group after intervention when compared to the wait-list group. Although nonsignificant effects were reported at the follow-up, large effect sizes were actually found.
Conclusion:
Although future studies are needed, the results of this study highlight the importance of board games and its efficacy as a possible therapeutic and/or preventive intervention on ADHD.
Introduction
Attention-Deficit/Hyperactivity Disorder (ADHD) constitutes the most prevalent neurodevelopmental disorder among children and adolescents, rising to a prevalence of 5.29% in individuals younger than 18 years. 1 Alterations in the frontal lobe have constituted one of the most important explicative hypothesis for ADHD, putting particular emphasis on the impairment of executive functions (EFs) (see Refs.2,3).
There is a broad consensus to accept that there are three relatively basic EFs (shifting, updating [working memory or WM], and inhibition), which can account for the other more complex ones. 4 The impairment in these EFs in children with ADHD has consequences at different levels such as lowering academic achievement, 5 increasing difficulties in socialization, 6 or hindering of peer functioning.7,8 Dovis et al. 9 also found that, besides the WM functioning, ADHD children also showed impairments in the capacity of storage short-term information, also known as short-term memory (STM).
Nowadays, psychopharmacological treatments are the primary interventions to treat ADHD, although there is not an agreement about its efficacy in improving EFs. 10 In addition, some children do not respond to this kind of treatment, 11 and many others show secondary effects due to medication, such as insomnia or decreased appetite, which hampers treatment's acceptability by parents and children. 12
An alternative to pharmacological interventions, or even a complementary treatment to them, is the use of cognitive training procedures. Although the benefits of this kind of therapy have not been yet clarified concerning EFs, 10 most studies have found significant effects of the trainability of WM and some of its components.13,14 Also, previous evidence shows that cognitive training of specific cognitive processes could improve the execution in other tasks for which the subject has not received specialized treatment. 15 This is known as the transfer effect, which could be divided into near transfer (improvement when doing similar tasks or processes) and far transfer (a broader improvement, such as the symptoms of ADHD attributed to the enhancement of the functioning of specific brain areas). 14 In relation with these effects, there are studies in favor 16 or opposing.14,17,18
Recently, some authors suggested that computerized cognitive training procedures may improve the cognitive functioning, 19 enhancing the dopaminergic tone 20 in neural structures related to ADHD. 21 Benefits of these cognitive training procedures could be higher with the inclusion of game elements because more cerebral areas could be activated. 22 In different studies,23,24 it has been found that those children with ADHD, who were trained with computerized training with game elements, obtained better scores in WM and motivation than those who had not. In an analog way, Mohammad and El-Shamieh 25 found that playing chess improved concentration capacity in children with ADHD. Nowadays, sales 26 and research27,28 of board games are arising. Modern board games are considered cognitive games that are mainly played on a board with pieces (and or cards) on it, with predefined rules that fix the number of pieces/cards on the board, the number of positions of the elements on the board, and the number of their possible moves. 29 Some of these board games depend low on fate and are manufactured more attractive to children than chess and are easy to get. Board games are sometimes oriented and published by the editors to improve specific EFs. 30 As far as we know, there is still no scientific study that assesses the efficacy of this kind of board games to improve the cognitive functioning and the recovery of symptoms in children with ADHD specifically.
To sum up, in this study, we aimed at studying the efficacy of board games as a cognitive training for EF (near-transfer effect) and for reducing general symptomatology (far-transfer effect) in children 8–12 years of age with a diagnosis of ADHD using a randomized control trial methodology. For this reason, we hypothesized that the participants of the experimental group would get better scores on the EF's measures and that they would show more far-transfer effects after the intervention, in comparison to the control group. A follow-up of a month was also conducted in the study.
Materials and Methods
Participants
The sample was initially composed of 29 children, 8–12 years of age and recruited from one public mental health center for children and adolescents in Lleida, Spain. All children were receiving treatment for ADHD at the moment of the study (see Table 1 for demographic characteristics). About ethnicity, 97% of the sample was of Spanish origin.
Differences in Demographic Characteristics Between Children in the Executive Function Game-Training (Experimental) and the Wait-List Condition (Control)
Note: Effect sizes were interpreted according to Cohen 44 and Cárdenas et al. 45 : d < 0.20 = trivial; 0.20 < d < 0.50 = small; 50 < d < 0.80 = medium; d > 0.80 = large; w < 0.10 = trivial; 0.10 < w < 0.30 = small; 0.30 < w < 0.50 = medium; w > 0.50 = large.
ADHD, attention-deficit/hyperactivity disorder; M, mean; SD, standard deviation.
Inclusion criteria for participation were (1) being 8–12 years of age, (2) studying in a primary school grade, and (3) having a diagnosis of ADHD disorder—including Inattentive or Combination subtype because no significant differences have been previously found in EF between children with hyperactivity alone or combined with inattention diagnosis. 31 ADHD's diagnosis was established after a clinical evaluation made by clinical psychologists—including second and third authors—and/or psychiatrists of the ADHD unit in the mental health center following the suggestions of the clinical practice guidelines for ADHD. 32 Exclusion criteria included (1) having other mental disorders, (2) having an estimated full-scale IQ measured by Wechsler Intelligence Scale for Children - Fourth Edition (WISC-IV) of <80 (clinical psychologists from the center gave these data), and (3) being in a sheltered center. The assessment necessary to apply the inclusion and exclusion criteria was performed by the team of psychiatrists and clinical psychologists of the mental health center that offered the data to the research team for this research.
Measures
In this study, as it can be seen in Table 2, the primary outcome measures consisted in the assessment of linguistic and visuospatial STM, the functioning of the updating process of the linguistic and visuospatial WM, and inhibition and shifting EF skills. We also analyzed the effects of the intervention in secondary outcomes: ADHD behaviors and general psychopathological symptoms. Finally, four confounding variables were assessed based on past research3,10,33: dose per day of medication (in mg); socioeconomic index (formula's index was: [education scale score] × 3 + [occupation scale score] × 5) 34 ; fluid reasoning (RAVEN test 35 ); and sustained attention skills (CARAS test 36 ). As it can be seen in Table 3, reliability was high in most of the analyzed subscales. However, those Strengths and Difficulties Questionnaire (SDQ) subscales with reliability scores <0.50 were not considered in the analysis: hyperactivity/inattention, peer relationship problems, and prosocial behavior.
Description of Instruments to Assess Outcome Measures
CPRS-48, Conners-48 Parents Rating Scale; RT, reaction times; SDQ, Strengths and Difficulties Questionnaire; STM, short-term memory; TMT, Trail Making Test; WISC-IV, Wechsler Intelligence Scale for Children - Fourth Edition; WM, working memory.
Baseline Differences Between Children in the Executive Function Game-Training (Experimental) and the Wait-List Condition (Control)
A. Due to practical reasons, the SDQ and CPRS were only fully answered by a subset of parents at pretest and posttest (N = 24/27).
B. Due to practical reasons, Digits and Go-Nogo task were only administered to a subset of children at pretest (N = 26/27).
All the analyses were nonsignificant. Effect sizes were interpreted according to Cohen 44 : d < 20 = trivial effect size; 20 < d < 50 = small effect size; 50 < d < 80 = medium effect size; d > 80 = large effect size.
Treatment
The intervention consisted of a cognitive training based on board games. A total of five board games were used: Alles Tomate! 37 and Alles Kanone! 38 that are supposed to work the linguistic updating process of the WM; Spooky Stairs 39 that requires visuospatial information updating of WM; Out of Mine! 40 that is focused on visuospatial rotation; and Chicken Cha Cha Cha 41 that is specifically centered in visuospatial STM and WM (see Supplementary Tables S1–S5 for a detailed description adapting Baranowski's suggestions 42 ; Supplementary Data are available at https://www.liebertpub.com/suppl/doi/10.1089/g4h.2018.0051).
Sessions were organized in closed groups (6–8 participants/group). The games consisted of five training sessions of about 60 minutes each, one game for each of the 5 weeks. People who conducted the sessions were one researcher (the first author of this article) and two assistant researchers. The intervention team remained stable across the sessions. Each session was planned previously and described in a handbook for the research, and was always executed in the same way: (1) during the first 15 minutes, different social activities were executed to facilitate the interactions between the participants (most of them did not know each other previously); (2) the first board game was administered during 30 minutes; (3) the second board game was administered during 30 minutes; and (4) during the last 15 minutes, researchers thanked the participation and attended parents' questions about individual situations of their children. In the different sessions, the board games used were as follows: session 1, Alles Tomate! and Spooky Stairs; session 2, Out of Mine! and Chicken Cha Cha Cha; session 3, Spooky Stairs and Alles Tomate!; session 4, Chicken Cha Cha Cha and Out of Mine!; and session 5, Alles Kanone! and the game they liked most (this was decided democratically by all the participants in each wave). Every four participants formed a playing group. We had two playing groups in each wave. Two games were played in each intervention session. One playing group played first with a board game and the other playing group to the another during the first 30 min. During the last 30 minutes, the games were interchanged between the playing groups. Researchers and assistant researchers only controlled that the rules of each game were properly followed, but letting the participants managing different situations that naturally occurred during playing (i.e., chatting). At the end of the last session, a certificate of attendance was given to each participant. No adverse effects were found during the intervention.
Procedure
First, the Clinical Research Ethical Committee of the university accepted the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Sample size calculation was determined following the results obtained by Klingberg et al., 43 considering two points of variance. In the calculation, the fields introduced were as follows: a bilateral 95% confidence interval with a 90% statistical power and a 50% of possible dropouts. Finally, 11 subjects of each group were determined, and 21 subjects in total were considered with possible dropouts. For the recruitment, all children with an ADHD diagnosis being treated at the center were put on a list. After applying inclusion and exclusion criteria, 53 families were randomly contacted by telephone and informed by phone or in person about the research project by the first author of the article. Informed written consent was obtained from all individual participants included in the study. Those parents, who accepted the participation of their children in the investigation, answered the informant questionnaires. Also, at baseline, all the participant children were assessed in selection and outcome measures by researchers from the investigation group and research assistants trained before in a laboratory at the University. Then, participants were stratified by age and sex, randomly assigned by a code to a wait-list condition (n = 14) or to the intervention group (n = 13), with a 1:1 allocation ratio by the first author. During this study, children continued with their regular treatment in their mental health center. Attendance at the sessions in the same laboratory at the University was collected to assess treatment adherence, because all children, except one, assisted at least four sessions. After the intervention, a posttest and a follow-up (1 month) evaluation of the outcome measures were carried out by the same assessment team that performed the preintervention assessments. Between posttest and follow-up, no intervention was implemented. The first author was the person who generated the random allocation sequence, who enrolled participants and assigned participants to interventions, and also made assessments and conducted the intervention. The other researchers were not blinded, and even participants knew the group assigned. The order of the neuropsychological tests on individual sessions was counterbalanced across participants to control assessment bias. Due to technical circumstances, the assessments and the interventions were performed into two waves (see the timeline in Supplementary Fig. S1). Figure 1 shows the diagram flow of participants through each stage of the study.
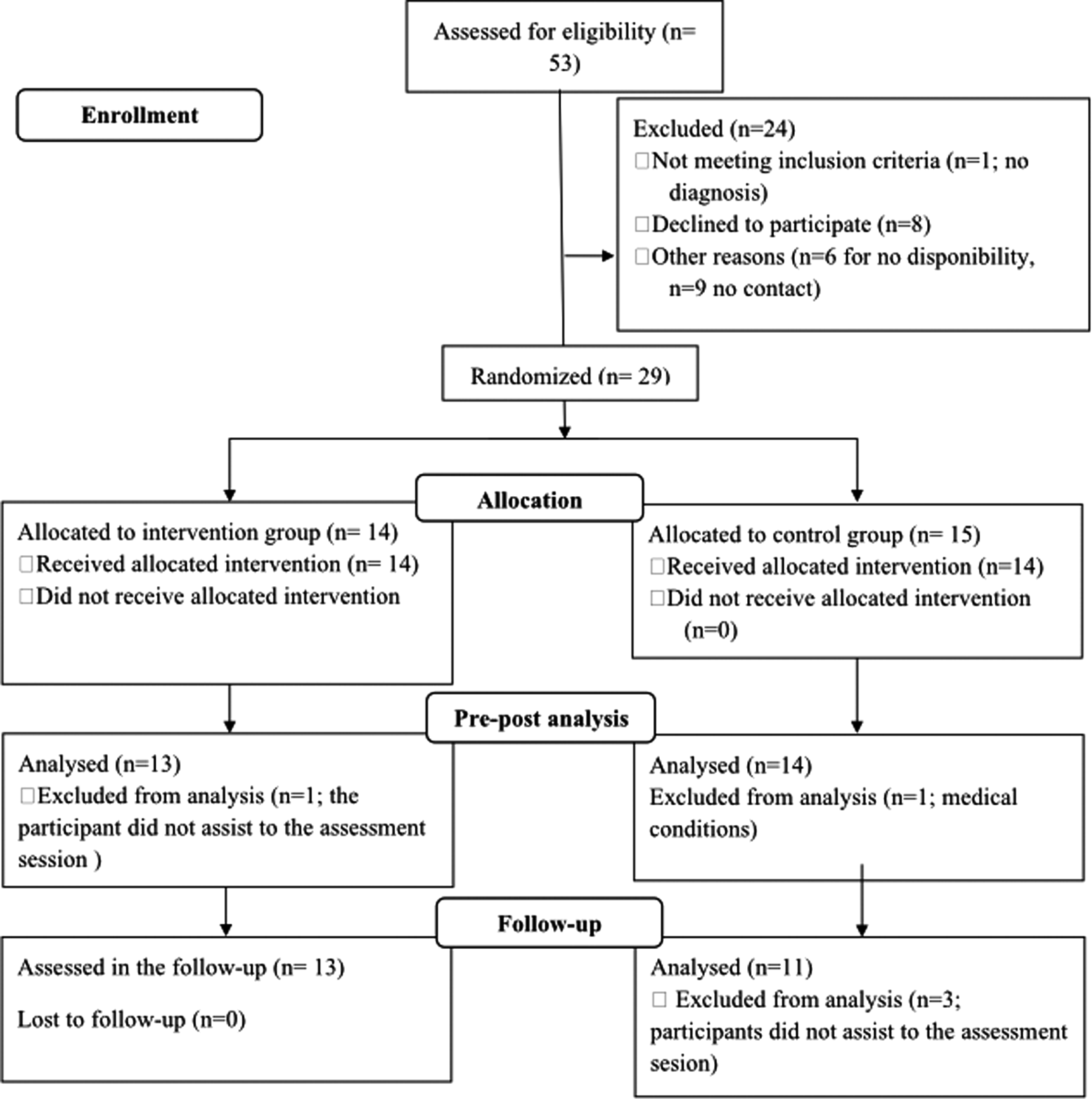
Diagram flow.
Statistical analysis
First of all, sociodemographic (age, gender, country of birth, and socioeconomic index) and clinical (diagnose subtype, type, and dose of pharmacology, fluid reasoning level, or family history of ADHD) differences between the experimental groups were analyzed using chi-square tests for categorical variables and independent t-test for continuous variables. Baseline differences in the outcome measures were also reported. Effects sizes were calculated following Cohen 44 and Cárdenas et al. 45 Regarding the SDQ and Conners-48 Parents Rating Scale, a variable was created with the average of mother and father scores for each subscale. Then, differences between experimental and control conditions were tested with analyses of covariance (ANCOVAs) for repeated measures with the time of assessment as within factor (pretest and posttest or pretest and follow-up) and treatment condition as between factor (training or wait-list) to assess short- and long-term effects. The effect of pharmacological dose per day, attentional level, socioeconomical level, and fluid reasoning was controlled in all the ANCOVAs. Multiple testing was corrected by Bonferroni correction. Following van der Oord et al.'s 46 methodology, missed items were replaced by the mean of the other items of the scale. If more than one item was missing, the subscale was not used in the analysis.
Results
Pretest comparisons
No significant differences were found in any sociodemographic or clinical characteristics comparing the experimental and control groups (Table 1).
Table 3 shows the mean, standard deviations, and the comparison between the intervention and control groups in the outcome variables of the study (in addition to the reliability of the psychometric scales). We only found a trend toward significance for the digits STM task, t(24) = −1.69, p = 0.10, and for psychosomatic, t(21) = −2.03, p = 0.06, with medium effect sizes. The rest of the analyses were not significant.
Short-term effects of the intervention
Executive function
As can be seen in Table 4, we found one significant time effect at posttest assessment. Children of both conditions showed higher scores in linguistic WM, F(1,21) = 4.82, p = 0.04, at posttest than at pretest, showing a large effect size (
Scores at Pretest and Posttest for Children in the Executive Function Game-Training (Experimental) and the Wait-List Condition (Control)
Bold indicates significant results with large effect sizes.
A. Due to technical reasons, SDQ and CPRS-48 (N = 24/27) were only administered to a subset of parents at pretest and posttest.
B. Due to technical reasons, Digits and Go-Nogo task was only administered to a subset of children at pretest (N = 26/27).
C. Due to technical reasons, Go-Nogo task was only administered to a subset of children at posttest (N = 25/27).
p < 0.05; **p < 0.01; ***p < 0.001;
We also found one significant difference between both groups comparing pretest and posttest assessments. Children in the EF Game-Training Condition showed significant increases at the linguistic STM scores, F(1,20) = 7.45, p = 0.02, with larger effects (

ADHD behaviors and general psychopathology
We found one significant effect at the Conduct Problems SDQ scale, F(1,18) = 12.51, p < 0.001, with large effects (
Long-term effects of the intervention
When analyzing the effects of the intervention in the experimental group 1 month after the intervention (see Supplementary Table S6 which shows all the long-term effects), only Linguistic Keep Track task showed a significant difference when carrying out an intragroup comparison, F(1,18) = 5.86, p = 0.03, with a large effect size (
Discussion
Previous research showed that computerized training could be efficacious in ADHD to improve WM 14 and EFs. 46 However, except for chess, 25 no other board game has been studied in depth as a training tool for individuals with ADHD.
In general, we found few significant results. One possible explanation is about the limitations of the study (i.e., the number of subjects). Another argument is that it is difficult to find far-transfer effects in cognitive training procedures. 47 Furthermore, the board games used in this research were focused in WM and STM processes and, in a weaker way, in the other EFs. It is possible that if we want to improve different cognitive processes, we must train them specifically. However, we found some significant results that are explained below.
Near-transfer effects
Results of the study showed that solely STM significantly improved after the intervention. It was estimated that those children who played board games could retain more linguistic information (up to 15.24% more information) than the control group. This fact is consistent with those studies which show that improvement can only be observed in the input capability.17,18 It is also in line with the studies which claim that, in many cases, this specific improvement is more noticeable in the linguistic STM. 14
Regarding linguistic WM, statistically significant improvements in time were found irrespective of whether the participants played the board games or not. This fact can be explained by the maturation effect produced in children of this age since it occurred in both groups (experimental and control). Previous literature has pointed at the relationship that may exist between this kind of WM and age or speed.48,49 This effect was replicated in the follow-up.
Far-transfer effects
The main short-term far-transfer effect found in this study is an important improvement regarding conduct problems. Since board games required the monitoring of standards and rules, as well as appropriate social interaction with other participants, an additive effect among the rules of the board games may have appeared. Taking into account the social impairment that many children with ADHD present 6 and that conduct problems and hyperactivity symptoms are highly associated, 50 the reduction of conduct problems has clinical relevance. Specifically, before the intervention, both groups—experimental and control—were on a normal range on Conduct Problems. Following raw scores from the SDQ, 51 children from the experimental group continued in the normal range, although with lower levels of conduct problems than before the intervention. On the contrary, the control group changed from normal range to subclinical range after the intervention. Hence, it seems that the board games intervention could prevent behavior deterioration. Moreover, group dynamics were taken into account in each one of the experimental sessions, which could have also helped in the control and maintenance of adequate behavior. Hence, future research is needed to clarify whether the improvement in conduct problems was due to playing to table-top games or to improving the STM capacity. The other results found, which were nonsignificant, were in line with past studies.17,18
Assessments at the follow-up to explore the stability of the effects of the training (long-term far-transfer effect) did not show significant results. However, we did find a large effect size in conduct problems. Although the effect was not statistically significant, the large effect size found implies that the improvement in conduct problems could remain stable for 1 month after the cognitive intervention.
Limitations and future studies
The very first pitfall of this study was the sample size. More participants are recommended in future studies. One explanation for this sample size was the strict inclusion and exclusion criteria, which included comorbidity.
The number of training sessions that participants took in this investigation should also be considered. Klingberg 20 suggests that to ensure the efficacy of memory training, there should be 8 hours of session for each subject. Future investigations should take into account the training with more sessions and with board games that train another EFs. Also, future interventions should take into account a follow-up of a more extended period. Besides, another improvement to future studies is to assess the clinical outcomes with multiple reporters (i.e., teachers).
Concerning the design of the study, another limitation is that the trial was not blinded. As other authors consider, 52 it is important to use this kind of methodology in future studies to guarantee the generalization and validity of the study. Also, it is essential to ensure an adequate control group, performing an in-group activity. In fact, probably, the best control group for this intervention should be playing board games that would not train any EF. Another consideration is the percentage of children who did not accept to participate in the study (26.42%), being interesting to assess ecological validity by playing at home or in school. Also, it would be interesting to perform an attrition analysis 53 to test if there would be differences between children who did accept to participate in the study and those who did not accept. As we could not assess any data from the nonparticipating children, we could not perform any attrition analysis in this research.
Finally, future investigations should also measure other variables related to cognitive training (e.g., previous experience with board games or motivation). Besides, the industry of board games has adapted some of them to a videogame environment. Future studies are intended to compare the efficacy of analog board games versus board videogames. Finally, other diagnoses in childhood characterized by EF's impairments, such as autism spectrum disorder, 54 could profit from this intervention, suggesting future studies on this line.
Conclusions
To summarize, our study shows evidence regarding the improvement of linguistic STM trained with board games in children with ADHD. In addition, children had the chance of interacting with other participants, which, in turn, improved their conduct problems. No other EFs or behavioral outcomes were modified. Hence, although the benefits of this game-based intervention are limited, it could be advisable to use it to help pharmacological interventions to improve the STM capacity and reduce conduct problems in ADHD children.
Footnotes
Acknowledgments
The authors thank the Comissionat per a Universitats i Recerca del DIUE, Generalitat de Catalunya (Grant Nos. 2014SGR1636 and 2017SGR1577), and the Centro de investigación Biomédica en Red en Salud Mental (CIBERSAM). The authors also thank the Department of Pedagogy and Psychology of the University of Lleida which funded the purchase of the games and to the children and their families. We also express our gratitude to the experts of Lu2 Enterprises (Xavier Moratonas) for advising us in the selection of games and to the assistant researchers (Marina Adserias and Jordi Callizo). This study was defended as a thesis of the master's degree in health general psychology at the University of Lleida.
Author Disclosure Statement
No competing financial interest exists.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.