
Abstract
Abstract
Objective:
The progression of chronic kidney disease can directly affect patient's health-related quality of life (HRQoL). Exercise training is a good option to reverse the impacts caused by the disease. To escape from the monotonous routine and stimulate further practice, the therapist should consider making physical activity more playful. Using videogames during exercise training is possible to rehabilitate the patient aiming for fun beyond the organic condition. The present study aimed to evaluate the effects of exercise training combined with Virtual Reality (VR) in functionality and HRQoL of patients on hemodialysis.
Materials and Methods:
A randomized controlled study in which control group (n = 20) maintained only hemodialysis without any physical effort or intervention from the researchers and intervention group (n = 20) who performed endurance and strength physical exercises in combination with VR during hemodialysis for 12 weeks. All eligible patients underwent a familiarization of games and were evaluated by an investigator-blind for functional capacity, quality of life, and depressive symptoms. Functional capacity tests included walking speed, timed up and go (TUG), and Duke Activity Status Index (DASI). To evaluate a HRQoL, Kidney Disease and Quality-of-Life Short-Form (KDQOL-SF™, v. 1.3) was used and to investigate depressive symptoms, the Center for Epidemiological Scale-Depression. Paired sample t-tests were conducted to determine differences within each group. Repeated-measures analysis of variance (group vs. time) was used to assess group differences in our major outcomes. The level of significance was 5%.
Results:
The exercise improved functional capacity (TUG: P = 0.002, DASI: P < 0.001) and HRQoL in physical and specific domains: physical functioning (P = 0.047), role physical (P = 0.021), as well as in physical composite summary (P < 0.001) and effects of kidney disease (P = 0.013). There was no influence on depressive symptoms (P = 0.154).
Conclusion:
Physical training combined with VR improved functional capacity and some quality-of-life domains of hemodialysis patients.
Introduction
The progression of chronic kidney disease (CKD) can directly affect a patient's health-related quality of life (HRQoL). 1 The impact of chronic diseases is not only judged by its mortality but also by its social impact, disability, and patients' perception about their illness. Based on that, any health care intervention should be a patient-centric approach. 2
Besides the complexity of the multidimensional concept of quality of life, HRQoL can be seen as a useful guide for improving health care quality. There is evidence that HRQoL significantly declines over time with the maximal decrement in physical components.3,4 The disease per se accelerates the appearance of sarcopenia, dynapenia, and mobility limitation, negatively affecting the levels of vitality and social interaction of the individual.5–7
Patients with CKD are at risk of developing or worsening preexisting physical impairments due to their pathophysiological condition associated with the sedentary life style. 5 Some CKD-based research of exercise training in patients on hemodialysis showed that this intervention is seen as a nonpharmacological agent of biopsychosocial recovery.8–11 Besides, it is safe and is associated with sizeable improvements in functional capacity and HRQoL.12–14
Despite these proven benefits, physical exercise therapy is far away from being part of a routine, especially during hemodialysis. 5 The most common barrier among patients is lack of motivation.15–18 To escape from the monotonous routine and stimulate further practice, the therapist should consider making physical activity more playful. The distinguishing point of previous studies is the idea of using videogame for physical training. The use of virtual reality (VR) in rehabilitation therapy of chronic diseases facilitated adherence to exercise therapy.19,20
VR has been a successful technology in therapeutic programs20–23 and our past experiences have demonstrated that exercise training combined with VR enables playful, interactive work and good feedback, facilitating patient interest and probable adherence to treatment. 23 The focus during the VR is not the disease but the activities that games propose and thus it is possible to rehabilitate the patient aiming for fun beyond the organic condition.24–26 In addition, a study of balance exercises and computerized cognitive training in elderly supports the notion that it is beneficial to combine computerized training with clinical practice over an exclusively physical or cognitive intervention. 27
Despite the growing interest supporting the use of VR in physical rehabilitation in a number of different clinical areas, the available literature lacks clinical and scientific evidences that support recommendations for exercise combined with VR guidelines. For patients with renal diseases, more robust studies are required. The present study aimed to evaluate the effects of exercise training combined with VR in the functionality and HRQoL of patients on hemodialysis.
Materials and Methods
Subject
The sample comprised of patients at a privately owned dialysis company: Clinese-Clínica de Nefrologia de Sergipe LTDA. The company had an estimate of roughly 300 hemodialysis patients during research. Since the company prescribes hemodialysis three times per week and does not have exercise training as part of routine activities, eligibility criteria included sedentary adults (≥18 years) who were on hemodialysis by arteriovenous fistula (AVF) for at least 3 months.
Exclusion criteria were hemodynamic instability, diagnosed respiratory disorder, visual impairment, or musculoskeletal and/or neurological limitations that compromised the ability to perform the proposed exercises. Throughout the research, absence from two consecutive sessions, withdrawal, or death were excluded from the final analysis.
Participants were assigned to control group (CG) or intervention group (IG) by generating random numbers at Random site (www.randomizer.org). All participants gave written informed consent and this study was approved by the Research Ethics Committee of the Federal University of Sergipe under number 236.202. The study was also registered in the Brazilian Registries of Clinical Trials (ReBEC) under the number RBR-9nckrq.
Exercise protocol
All eligible patients underwent a familiarization of games from Wii™ Sports (2006) and Wii Fit™ Plus (2009) software previously selected by researchers for physical training (Table 1). In the pre-exercise session, patients included at the study were evaluated by an investigator-blind for functional capacity, quality of life, and depressive symptoms.
Nintendo Wii Games and Their Respective Motor Demands
At the Random site, we used a blocked design to generate random numbers. An independent researcher made random allocation envelopes using group names (CG or IG) representing computer-generated random sequence numbers. The original random allocation sequences were hidden from all other researchers. The group name was typed on a blank sheet of paper that was cut, all the same size, and folded a few times and then placed inside envelopes that were sealed and opened immediately before the initiation of the exercise training.
After randomization, CG patients maintained only hemodialysis and regular activities without any physical effort during the sessions, and without any intervention from the researchers. Meanwhile, GI subjects performed endurance and strength exercises in combination with VR games in a progressive manner for 12 weeks.
Due to the space limitation, patients from both groups remained in the same dialysis room and therefore, it was not possible to blind patients. They were advised by researchers not to offer any information to the investigator-blind about the group to which they belonged.
The exercises were based on the repetitions of movements and motor demands of each preselected game. During the activities the individual maintained the sitting position working on the coordination, balance, and resistance of the lower limbs and the upper limb without the AVF.
The exercise protocol was performed every session with a frequency of three times a week. The exercises were always performed within the first 2 hours of hemodialysis, not using the member with AVF according to the recommendations of the American College of Sports Medicine. The mean duration ranged from 30 to 60 minutes as suggested by NKF-KDOQI and Life Options Rehabilitation Advisory Council and the guidelines of the Cochrane Collaboration. The progression of therapy occurred on average every 2 weeks, with changes in the type of games and exercises (Table 2).
Exercise Training Protocol with Virtual Reality
The training started with stretches held for 30 seconds. Subsequently, physical exercises were performed associated with videogames. Finally, the cycle ergometer was used as an auxiliary tool for aerobic effects. From the 16th week onward, Thera-band and ankle weight were used to impose resistance to muscle during training. Adverse events were investigated at each session and recorded, when present, for further analysis.
The intensity of training was measured from the subjective perception of the effort classified by the Borg scale of 6–20 points. The cutoff point for heart rate training was 12–14 characterized as “somewhat hard.” Each patient received instructions to stop all activity if they felt dizzy, unusual shortness of breath, or experienced chest pain.
Compliance was measured as a minimum of 80% of the goal exercise time for that session successfully completed. Subjects in the CG group were not given access to any exercise protocol tool.
Techniques for measurement of the hemodynamic
Regarding blood pressure measurement, the indirect method was used with an auscultatory technique and calibrated aneroid sphygmomanometer (standardization). The technique of checking and evaluation of blood pressure measurements followed the protocol recommended by the Brazilian Society of Cardiology in the Brazilian Guidelines for Hypertension. The respiratory rate was measured from the inspection of the number of inspirations per minute. Pulse and oxygen saturation were measured from the oximeter (OLED-Fingertip pulse).
Clinical outcomes
The choice of evaluation tools was based on recommendations from previous publications.28,29 All measurements were conducted on a “nondialysis day” and analyzed by a blinded investigator.
Walking speed
The test followed the recommendations of Fritz et al. 30 Each individual was instructed to walk at a comfortable accelerated pace, without running, a distance of 20 meters demarcated in a flat straight path corridor. The measurement of time using a stopwatch neglected the first and the last 5 meters, which correspond to the period of acceleration and deceleration of the march. The time used to cover the 10 meters was recorded in seconds and subsequently used to calculate the walking speed (WS) (meters per second). 31
Timed up and go
The test was performed following the original protocol of Podsiadlo and Richardson. Time was measured in seconds for the ability to transition from sitting to standing, walking for 3 meters in a straight line, rotating 180° returning in the course, finishing in the seated position again, and lying back in the chair.32,33 Times greater than 10 seconds were considered to compromise functional mobility. 34 Its reliability with chronic renal patients has already been tested and approved. 35
Duke Activity Status Index
This is a simple questionnaire with rapid administration, containing 12 items that describe activities of daily life, such as personal hygiene, locomotion, domestic tasks, sexual function, and recreation. 36 The score is calculated based on the affirmative answers whose value is weighted by the metabolic equivalent of that activity. The possible scores vary from 0 (all “no” answers) to 58.2 (all “yes” answers), with higher scores reflecting a higher functional capacity. Its reliability with renal patients has already been tested. 37
Health-related quality of life
The Kidney Disease and Quality-of-Life Short-Form (KDQOL-SF™, v. 1.3) obtained from the website (www.rand.org/health/surveys_tools/kdqol.html) was used. This questionnaire contains eight generic domains formed from SF-36 questions grouped into physical composite summary (PCS) and mental composite summary (MCS) and 11 specific domains related to renal disease. Responses are transported to an Excel spreadsheet provided by the KDQOL-SF Working Group. This worksheet recodifies data from each item of the questionnaire, resulting in preanalyzed data, with a normalized scale ranging from 0 (worst quality of life) to 100 (best quality of life). 38 Higher scores indicate greater health perception and absence of problem. Dimensions are assessed and scored separately, and there is no single value resulting from the overall assessment of quality of life.
Depressive symptoms
The Center for Epidemiological Scale-Depression (CES-D) questionnaire was used. The questions emphasize the symptoms in the last 7 days before filling in. The final score ranges from 0 to 60 points, with higher scores indicating more depressive symptoms. Originally, the cutoff point of the CES-D scale for identifying depressive symptoms was ≥16 points, 39 but its use in chronic renal patients demonstrates that a cutoff point of ≥18 points would present better diagnostic accuracy, 40 presenting 69% sensitivity and 83% specificity for depressive symptoms. 41
Statistical analyses
For sample calculation a Paired t-test was used, considering a statistical power of 95%, significance of 5%, and an effect size of 1.17 for timed up and go (TUG); in a two-tailed test an estimate of 20 patients per group (CG and IG) was found. To this analysis, Cheema et al. 42 and Cho and Sohng 22 were referenced.
All statistical analyses were performed using the R Core Team 2016 software and significance was based on a two-tailed α value of 0.05. Paired sample t-tests were conducted to determine if values between time points differed significantly within each group. Repeated-measures analysis of variance (group × time) was used to assess group differences in our major outcomes. The Cohen effect size was used to evaluate the magnitude of the differences.
Results
Fifty-eight patients on hemodialysis were recruited. Thirteen were excluded because they fit within the criteria that included hemodynamic instability, respiratory compromise, visual impairment, or musculoskeletal and/or neurological limitations that interfered with the ability to perform the proposed exercises. The 45 individuals included were randomized (www.random.org) and allocated to CG with regular activities and IG that play intradialytic exercise training. During follow-up, there were two dropouts and one death in the CG and one loss of follow-up and one patient with adverse events unrelated to the intervention in the IG, then 20 patients in each group remained until the end of the study (Fig. 1).
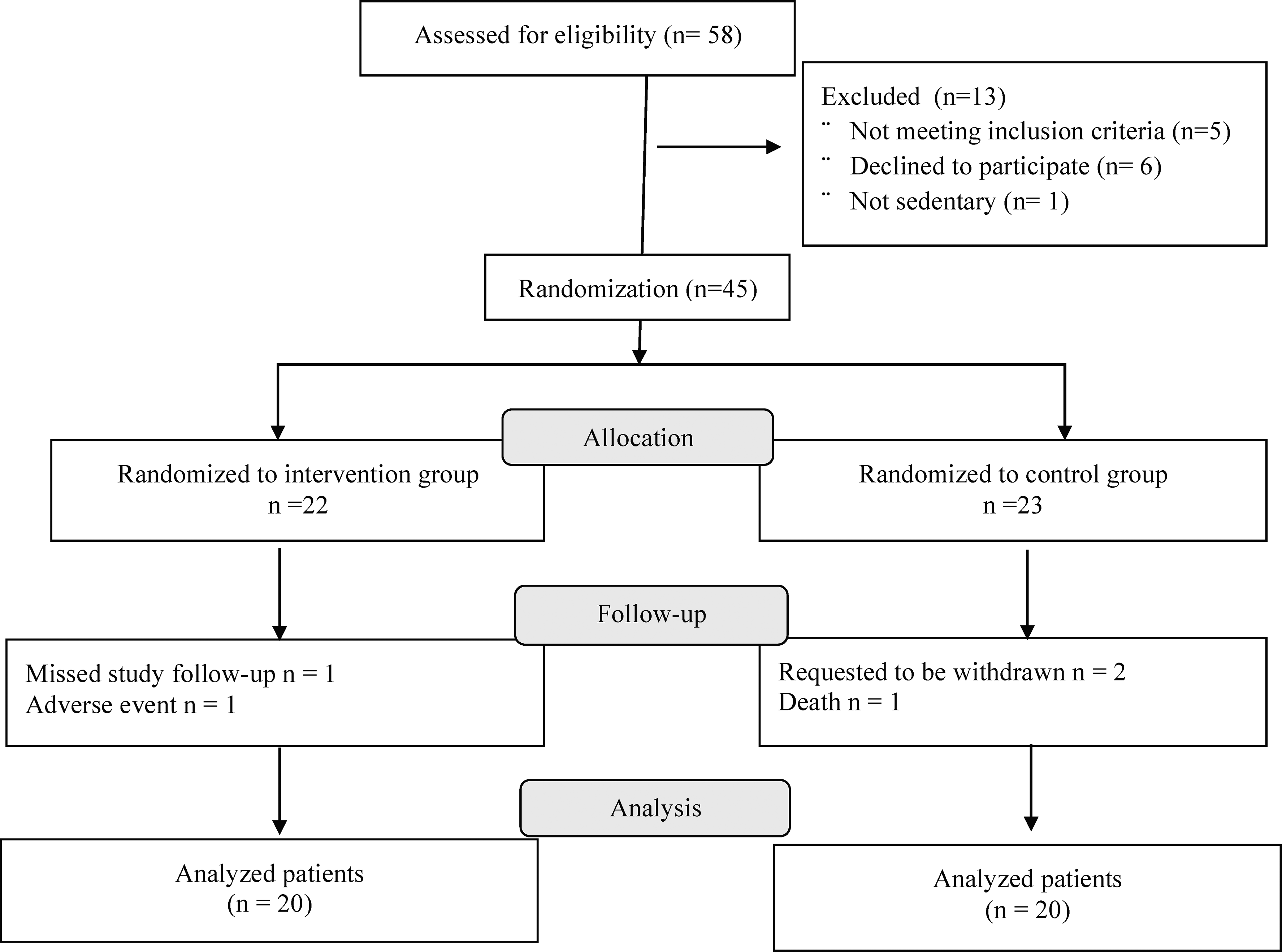
CONSORT diagram.
The sociodemographic characteristics (Table 3) and clinical, functional, and quality-of-life profile (Table 4) were similar at baseline. The main comorbidity associated with renal disease was hypertension (Table 3).
Sociodemographic Profile of the Study Population
BMI, body mass index; CG, control group; IG, intervention group; SD, standard deviation.
Clinical, Functional Profile of Quality of Life and Depressive Symptoms in the Baseline Period
Baseline values were obtained in the prestudy session. s, second(s); m/s, meter(s) per second.
CES-D, Center for Epidemiological Scale-Depression; DASI, Duke Activity Status Index; DBP, diastolic blood pressure; HR, heart rate; KDQOL, Kidney Disease and Quality of Life; MCS, mental composite; PCS, physical composite summary; RR, respiratory rate; SBP, systolic artery pressure; SpO2, partial oxygen saturation; T10, gait speed test; TUG, timed up and go test.
There was no significant change in hemodynamic aspects after 12 weeks (Table 5). For IG, comparing to baseline, the exercise combined with VR revealed a significant improvement in functional capacity as seen in TUG (P = 0.001), T10 (P = 0.036), and Duke Activity Status Index (DASI) scores (P < 0.001) (Table 5). Comparing both groups at the end of 12 weeks, the IG group presented a significant improvement of the TUG (P = 0.002) and the DASI (P < 0.001) (Table 5).
Hemodynamic, Functional, Quality of Life, and Depressive Symptoms' Response to Intradialytic Physical Training Combined with Nonimmersive Virtual Reality
Baseline values were obtained in the prestudy session. The postintervention measures were made at the session following the closure of the 12th week. s, second(s); m/s, meter(s) per second.
P < 0.05 versus baseline (intragroup).
P < 0.05 interaction in time (analysis of variance repeated measures).
At the end of the study, IG was able to modify the quality of life significantly in relation to baseline. Differences were described in domains of effects of kidney disease (P = 0.05), work status (P = 0.042), physical functioning (P = 0.013), role physical (P = 0.028), general health (P = 0.011), and PCS (P = 0.002) (Table 5).
At the end of the 12th week, IG improved significantly in relation to the CG in domains of effects of kidney disease (P = 0.013), physical functioning (P = 0.047), and role physical (P = 0.021), as well as in PCS (P < 0.001) (Table 5).
Concerning depressive symptoms, 35% of IG subjects and 45% of CG had depressive symptoms at the beginning of the study. After 12 weeks, this frequency reduced to 15% and 40%, respectively. However, there was no significant group interaction in time for the CES-D score (P = 0.154) (Table 5).
Discussion
Despite the benefits of exercising, important gaps in knowledge about meaningful change in performance of patients with CKD remain. To the best of our knowledge, the present study is the first randomized clinical trial in Brazil to work on nonimmersive VR during hemodialysis.
The most significant result was the improvement in functional capacity and HRQoL. Similar findings were described in our previous research with patients in the immediate postoperative period of cardiac surgery. 43
In this population, a low functional capacity is a significant predictor of mortality, even more than loss of muscle mass. 44 Therefore, performance measures provide important information on how physical components could lie in the pathway between CKD and adverse health outcomes. Besides, physical performance has the potential to serve as primary indicator of benefit in future clinical trials.42,45
The results showed a significant increment of 0.1 meter per second in WS within the IG. According to Sawant and Overend, 46 patients on HD are slower by 1.26 meter per second when compared with age-matched normal controls with no kidney disease and effects of exercise led to a mean change of 0.08 meter per second on functional performance. Differences of 0.10–0.20 meter per second are considered meaningful changes.47–49 In this research, the comparative analysis between the groups did not present a significant difference possibly due to total duration of exercise, since four more weeks of training in a similar study obtained significance in the analysis. 50
Many people with CKD on hemodialysis have great difficulty to stand quickly from a chair. Considering important activities for mobility, such as sitting, lifting, and walking, 51 the physical training combined with VR provided an improvement of 18% in TUG performance with an average reduction of 1.9 seconds in the test. The comparison with GC was significant demonstrating that subjects from IG walked more briskly.
Similar findings can be seen in the studies by Heiwe and Jacobson 14 that reported a 13% improvement in TUG after 12 weeks of exercise and by Bullani et al., 52 who after 6 months of resisted moderate-intensity exercises found a statistical improvement of 1.1 seconds in mobility (P = 0.015). The TUG has shown strong test/retest reliability in ESKD patients undergoing HD.34,35,53
The aerobic conditioning in our research was intensified by the use of the cycle ergometer. The influence of this tool on physical performance was described by Storer et al. 54 showing a 12% increase over TUG (P = 0.012) after 9 weeks.
Performing physical exercise during HD may induce complications as documented by Himmelfarb, 55 but those adverse effects can be minimized by respecting the recommendation of training in the first 2 hours of the HD session and considering the subjectivity of the individual. During our research, except for one subject, no one exhibited increased unwanted symptoms, such as muscular cramps, hypotensive episodes, arrhythmia, nausea, vomiting, or headaches, demonstrating safety in performing the exercises.
The self-reported level of fitness was measured with the DASI.28,37 The IG presented a significant increase of 35% in the score corroborating with the improvement in the functionality and physical performance of the tests mentioned previously. CG showed a 14% reduction in the DASI score. After 12 weeks, the groups were significantly different as to functional capacity. Studies with similar physical rehabilitation programs also achieved an increase of 35% 56 to 50% 57 in the DASI score, revealing significant functional improvement (P = 0.013).
Functional impairment is adversely associated with quality of life. Nowadays, promotion of HRQoL is generally one of the major goals in the treatment of chronic diseases. 58 The analysis of HRQoL in all domains of renal patients serves as a parameter of impact and adequacy of treatment as already described by the American National Kidney Foundation and the National Institutes of Health. 59
We chose to use the KDQOL-SF (v. 1.3) questionnaire from RAND corporation. The combination of generic with a kidney disease-specific domain allows us greater approach about a chronic renal patient's quality of life. 60 Results from SF-36 can be further summarized into a PCS and a MCS score.
From the baseline period to the end of 12 weeks, there was no protocol interference on the emotional domains of the questionnaire for both groups. However, IG showed an improvement in physical domains (role physical, physical functioning, general health, and PCS) and specific (effects of kidney disease and work status). Ouzouni et al. 61 also reported modifications only in the physical components arguing their findings with the fact that chronic patients, over time, learn to deal with the disease and its commitments.
The comparison between the groups after 12 weeks demonstrates a significant improvement of the physical aspects (role physical, physical functioning, and PCS) and the effects of kidney disease in patients who exercised. These findings are consistent with the study by Wu et al. 62 who found the same duration of physical exercise to be significant for the same domains described, as well as others, such as vitality, sleep, patient satisfaction, team encouragement, and symptoms of diseases.
On deepening the analysis of the emotional aspects, we investigated the presence of depressive symptoms by the CES-D and detected that 40% of all patients presented depressive symptoms in the basal period (seven individuals of the IG and nine of the CG). Depressive symptoms are frequently detectable in this population and can be described in ∼50% or more of the evaluated patients.63,64
VR training therapy minimized depressive symptoms (P = 0.154) although it was not statistically significant. This result may have been influenced by the duration of the exercise protocol, since longer protocols, such as Kouidi et al. 65 and Jung and Park, 66 showed a significant improvement in depressive symptoms. Besides, Dialysis Outcomes and Practice Patterns Study (DOPPS) demonstrated that the practice of exercise is inversely associated with depressive symptoms. 67
Previous studies in the same center revealed a prevalence of depression higher than that described for the general population. 65 In addition, depression was the major predictor of quality of life in patients on hemodialysis 65 and depressive symptoms and anxiety were independent factors associated with HRQoL. 67
Our findings reveal that the combination of training with VR brings benefits similar to those of conventional physical training described in the literature. Our differential lies in the playfulness of therapy.
The main nonphysical complaint of patients on hemodialysis is monotony. Physical training combined with VR was a playful proposal, confirming our hypothesis that patients would remain adherent to the protocol until the end of their duration and would achieve an improvement in the outcomes.
The immediate feedback provided by games facilitates motor learning and maximizes the therapeutic effects and encourages patients to overcome their own limits in the pursuit of better performance in games.68,69 Thus, videogames can captivate even those groups stigmatized as resistant.
Videogame is an opportunity to help people reduce the impact of chronic disease limitations. The combination of VR and exercise might promote the mood benefits of exercise. Improving psychological mood plays an important role in enhancing performance and adherence. 70
The great limitation of our study lies in the Hawthorne effect. Because physical exercise is not a common practice in the population studied, individuals could have responded positively to the therapy simply by being accompanied and observed during the 12 weeks of exercise. Another possible limitation is the fact that physical training was not performed exclusively by VR games but associated with the cycle ergometer. It is difficult to transpose the benefits achieved only through the VR tool. Lastly, depressive symptoms were evaluated by a self-reported scale, which does not allow us to diagnose depression.
From the data obtained in this study, it was possible to conclude that physical exercise combined with VR was able to improve the functional capacity and some domains from HRQoL of patients on hemodialysis, especially those related to the physical components. This research has added new information to the knowledge gap on VR and renal disease.
Footnotes
Acknowledgments
The authors would like to show their gratitude to Clinese: Clínica de Nefrologia de Sergipe for having opened doors for the development of research and all clinical staff who provided insight and expertise that greatly assisted the research. This study was self-funded.
Author Contributions
L.G.M., J.A.S.B.F., and K.A.B. had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: L.G.M., J.A.S.B.F., and K.A.B. Acquisition of data: L.G.M., D.L.M., N.S.L., and J.C.D.S. Analysis and interpretation of data: L.G.M., J.A.S.B.F., K.A.B., and W.M.S.J. Drafting of the article: L.G.M., J.A.S.B.F., and K.A.B. Critical revision of the article for important intellectual content: L.G.M., J.A.S.B.F., K.A.B., and W.M.S.J. Administrative, technical, or material support: D.L.M., N.S.L., N.L.S.A., and E.M.J. Study supervision: J.A.S.B.F., and K.A.B.
Author Disclosure Statement
Dr. K.A. Bastos is part of the clinical staff of the Clinic of Nephrology of Sergipe (Clinese) as nephrologist.