
Abstract
Objective:
The purpose of this project was to create a web-accessible drug education program that would positively impact student knowledge and perceptions.
Materials and Methods:
An interactive computer module (Interactive Module to Halt Abuse of Prescriptions in Preteens and Youth [I'M HAPPY]) was created using a combination of e-learning and animation software. The module used narrated illustrations, animations, and games to explain what over-the-counter (OTC) and prescription drugs are, how they are used correctly, and what risks they carry. Animated drug refusal scenarios with user-determined outcomes were also incorporated. Sixth-grade students were asked to complete the module online and were given a 14-question pretest and posttest on the definitions, adverse effects, and proper use of OTC and prescription medicines. They were also asked to rank the perceived helpfulness of several drug refusal strategies. Student opinions about the computer module itself were collected on the posttest.
Results:
Students (n = 34) scored better on quiz questions following the module. They also showed increased favorability toward three of four drug refusal strategies after completing the module, with a greater proportion ranking these strategies “Very Helpful.” Most students indicated they learned new things from the module (79%) and found it enjoyable (88%) and easy to use (97%).
Conclusion:
The I'M HAPPY program improved student knowledge of OTC and prescription drugs and enhanced perceptions of the helpfulness of certain drug refusal strategies. The computer module was considered enjoyable and easy to use, and can be easily disseminated to any student or classroom having internet access.
Introduction
A recent study revealed that 10% of 12th graders in the United States reported misusing a prescription drug within the previous 12 months. 1 The state of Utah alone experienced a nearly 400% increase in the number of deaths due to prescription drug misuse and abuse between 2000 and 2015, placing it in the top 10 in the nation for overdose deaths. 2 The National Institute on Drug Abuse has noted children are likely to first experience drug abuse in early adolescence as they transition from elementary to middle school. 3
The rate of prescription drug abuse among sixth graders in Utah is 3.5%, but that number more than doubles by the time students are seniors in high school. 4 In response to statistics like these, a variety of school-based prevention programs have been developed locally and nationally to reduce improper drug use among youth, with each program having its own particular emphasis.
It has been proposed that drug prevention programs can be categorized based on whether their content focuses mostly on improving (1) knowledge of drug risks and dangers with the intent of building a negative affect in participants, (2) social competency skills such as self-control, decision making, stress management, and self-esteem, (3) social influence, where participants are taught to be aware of, properly contextualize, and manage media, peer, and family influences, or (4) a combination of these. 5
While it can be argued that establishing a baseline knowledge of terms, mechanisms, and complications involved in drug abuse is a requirement for an effective drug prevention program, those programs focused solely on using knowledge to develop a negative attitude toward drug abuse have poor efficacy outcomes. 6 In contrast, a Cochrane review found that programs centered on developing a combination of social competency and social influence skills showed consistent positive effects on prevention. 7
Prevention programs such as DARE 8 or UNPLUGGED 9 are examples of widely used classroom-based curricula. Both programs use combination approaches to drug prevention, in that, they target a broad range of intrapersonal and interpersonal skills, in addition to knowledge. As such, both programs occur over 10 or more sessions and, while they occasionally incorporate activities, quizzes, or audiovisual presentations, their primary focus is on classroom or small-group discussion led by law enforcement officers, teachers, or peer leaders.
Limitations with classroom discussions that may affect their degree of influence are that not all students actively participate in these discussions and that students do not have an opportunity to autonomously revisit the topics discussed. Thus, developing a web-based program that students can work at their own pace may be a potential solution. In addition, if the program can be offered in an entertaining format like a computer game, students may have greater interest in participating. 10 Many other potential advantages of computer-based interventions have also been noted, including less dependence on trained staff, which translates to lower costs for program implementation and dissemination, and more uniform fidelity in the content delivered. 11
In an effort to incorporate knowledge, social competency, and social influence skills into a drug prevention program that can be easily disseminated to widely dispersed classrooms, an online computer module dubbed I'M HAPPY (Interactive Module to Halt Abuse of Prescriptions in Preteens and Youth) was developed. Social learning theory provides the basis for interventions that seek to improve social competency (e.g., decision-making and problem-solving skills) and social influence (e.g., refusal skills), with the premise that interpersonal factors have a significant impact on an adolescent's attitude and behavior toward drugs. 12
The I'M HAPPY module targets knowledge and social skills using gamified elements, such as storytelling, learning challenges, and immediate feedback. 13 According to the theory of gamified learning, gamification has the potential to improve instruction by positively influencing student learning behaviors and attitudes toward the intended learning outcomes. 14 I'M HAPPY was evaluated with sixth-grade students for its ability to enhance baseline drug knowledge and improve perceptions of the helpfulness of drug refusal skills.
Materials and Methods
Intervention
The I'M HAPPY computer program is delivered through the internet and is interactive, in that, user input is required for the program to advance and helps determine the course of events within the program. I'M HAPPY was created using a combination of e-learning authoring software (Storyline® 2; Articulate® Global, Inc.) and a web-based platform for the creation of animated videos (GoAnimate; GoAnimate, Inc.). Students had the option to redo any section of the program upon completing that section.
The program incorporates illustrations, narrated text, games, and animated scenarios to address the following objectives: define over-the-counter (OTC) drugs, describe how OTC drugs are properly obtained and used for various conditions, define prescription drugs, describe how prescription drugs are properly obtained and used for various conditions, demonstrate different dosage forms for prescription drugs, define drug adverse effects, explain how the risk of adverse effects increases with increasing drug dose and drug misuse, explain how the adverse effect of addiction occurs and why it is dangerous, illustrate situations in which drug abuse and misuse may be encountered, and introduce and model drug refusal skills (Fig. 1). Characteristics of the program are outlined in Table 1. The program is available at tmrose.wixsite.com/imhappyproject.
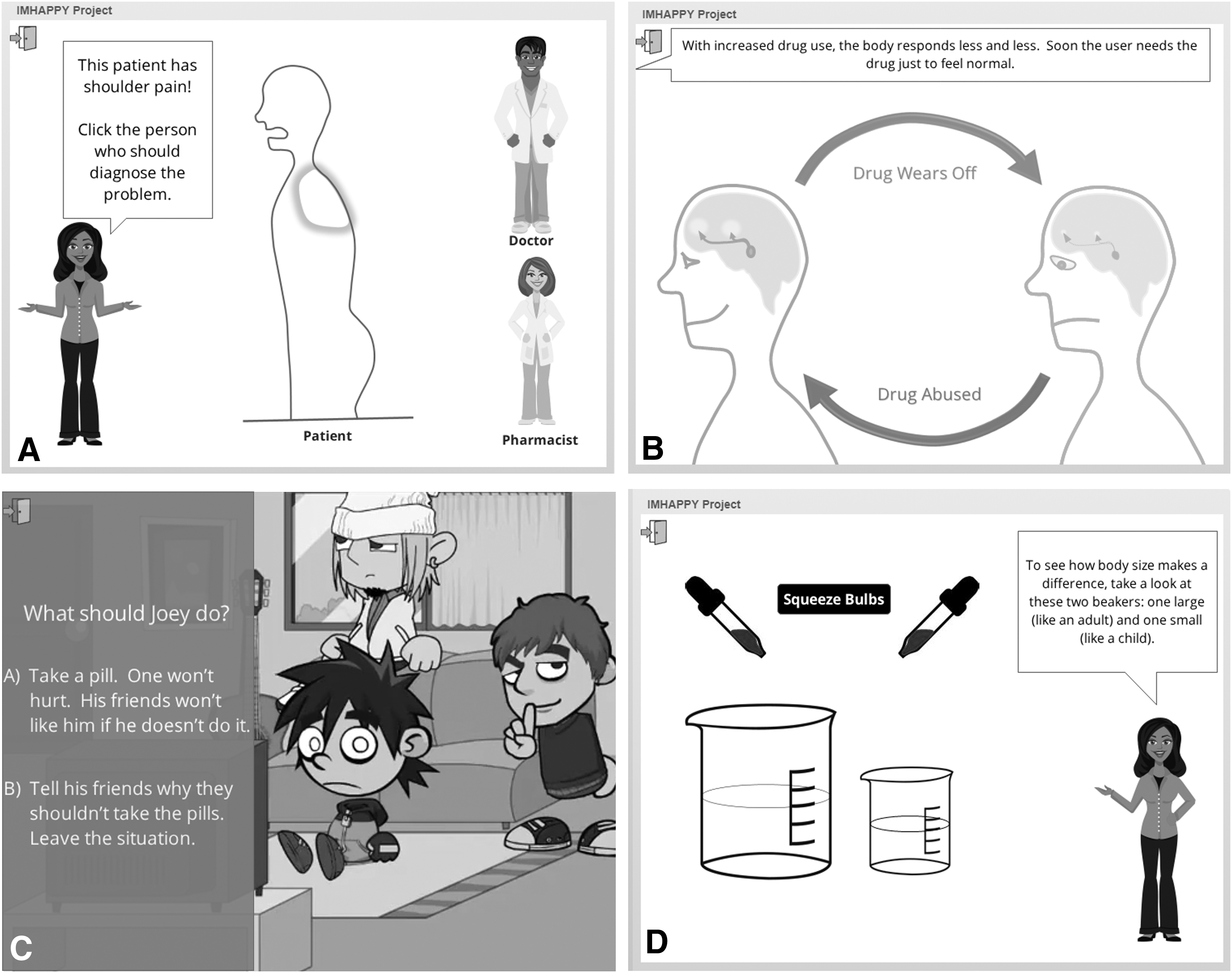
Still images from Interactive Module to Halt Abuse of Prescriptions in Preteens and Youth (I'M HAPPY).
Characteristics of I'M HAPPY
I'M HAPPY, Interactive Module to Halt Abuse of Prescriptions in Preteens and Youth; OTC, over the counter.
The content of I'M HAPPY was guided by input from focus group interviews with parents and staff members associated with the Sandy Club, an after-school program that provides social, academic, and health support for young people in Sandy, Utah. Input was also obtained from focus group interviews with steering committee members of Prevention Dimensions, a publically sponsored entity whose mission is to produce educational resources that help reduce violence and substance abuse among K-12 students in the state of Utah.
The recurring message from these meetings was that, in addition to informational elements, the program ought to teach about short- and long-term consequences of drug abuse/misuse and help support peer/social resistance training and sound decision making. To address these ideas, unique animated scenarios were included in I'M HAPPY, which allowed students to choose how the animated character would respond and observe the outcome (Fig. 1C).
Participants
I'M HAPPY was distributed by an emailed web link to sixth-grade students at a charter school located in northern Utah. Students completed I'M HAPPY using Google Android tablets during their regularly scheduled health class supervised by their regular teacher. Passive parental consent for student participation was obtained before class. The version of the program distributed to the students included a student assent screen that allowed students to opt out of participation before beginning the program. Participation in I'M HAPPY was voluntary and exit points were included frequently throughout the program. The study was approved by the institutional review board of Roseman University of Health Sciences.
Surveys and data analysis
Students who opted to participate were prompted to complete an online (Qualtrics®XM) pretest survey before engaging with the content. The pretest consisted of 18 questions: 14 multiple-choice questions to test student knowledge of prescription and OTC drugs, their safe use, and adverse effects, and 4 opinion-based questions in which students ranked the helpfulness of four proposed refusal methods for avoiding or getting out of a situation where drugs were being abused: (1) asking questions about an activity beforehand (e.g., finding out who will be there and what they plan to do), (2) naming the problems (e.g., explicitly stating that taking drugs is dangerous and illegal.), (3) suggesting something else to do (e.g., proposing a safe, but appealing alternative activity), and (4) leaving the situation (e.g., excusing yourself or just walking away).
Student-perceived helpfulness was reported on a 5-point scale from “very helpful” to “very unhelpful.” The posttest (Supplementary Appendix SA1) contained the same questions as the pretest, plus five additional multiple-choice questions asking about the students' opinions and experiences with the program, and an open-ended question asking what could be done to improve the program. Both surveys were anonymous, but three questions at the beginning of each survey were used to generate a code to match pretest and posttest data to the same student.
A paired t-test was used to compare pretest and posttest performance on the quiz questions. A two-tailed McNemar's test with continuity correction for paired data was used to detect differences in the relative proportion of students who found each refusal method “very helpful” before and after completing the program. Statistical tests were performed using GraphPad Prism 6 and QuickCalcs (https://www.graphpad.com/quickcalcs/).
Results
Testing early drafts of the program with Sandy Club and charter school students of different grade levels suggested the content and tone of I'M HAPPY were most helpful and acceptable for sixth graders (data not shown). The pilot study with charter school sixth graders produced 48 responses to the pretest and 34 responses to the posttest. The 34 paired responses to the 14 quiz questions were compared before (84% correct) and after the program (88% correct), and a significant increase in student knowledge was observed (P = 0.02 [t = 2.405], Cohen's d = 0.28).
On the pretest, student opinions were mixed on the extent of the helpfulness of four refusal skills, but the proportion of students finding these skills to be “very helpful” increased on the posttest, achieving significance in three cases (P-value and chi-square value): “naming the problems (0.03 and 4.90),” “suggesting something else to do (0.008 and 7.11),” and “leaving the situation” (0.008 and 7.11). The proportion who found the fourth refusal skill, “asking questions,” to be “very helpful” did not significantly increase (0.23, 1.46).
When asked their opinions of I'M HAPPY, 97% said it was easy to use, 88% said they enjoyed doing the program, and 79% said they learned something new. Student open-ended responses to the question of what could be done to make I'M HAPPY better are clustered thematically in Table 2. Because it is an interactive program dependent upon user input, the time required to complete I'M HAPPY is variable, but ranged from 17 to 37 (mean = 26 and SD = 3.75) minutes in this study.
Thematic Analysis of Responses to “What Could Be Done to Make the I'M HAPPY Program Better?” (n = 31)
Discussion
Transitional periods in a child's life, such as the onset of puberty or transfer to a new school, have been identified as times when children are most vulnerable to becoming engaged in substance abuse or misuse. 3 For most children, sixth grade occurs at the onset of puberty and marks a transition from elementary to middle school. The number of intrapersonal and interpersonal changes for students in sixth grade makes it an ideal time for prevention program delivery. Testing I'M HAPPY with students in fifth, sixth, and seventh grades suggested sixth graders gained the most knowledge and enjoyment from the program.
Online delivery of prevention programs is a growing trend, but there are no published examples of programs focused on the misuse or abuse of prescription or OTC drugs.11,15–19 However, computer-based prevention programs targeting students at or near the sixth-grade level, which use a similar approach to I'M HAPPY, have shown significant, beneficial effects on knowledge, use, and/or intention to use tobacco, alcohol, and cannabis.18,20–24 I'M HAPPY improved student knowledge and perceptions of the helpfulness of drug refusal strategies, which accomplished the intended aims of positively affecting student knowledge, social competency, and social influence skills.
In the theory of reasoned action, behavioral intentions are influenced by attitudes, which are in turn shaped by beliefs. 25 The positive effect of I'M HAPPY on student perceptions of drug refusal skills may therefore lay the groundwork for future use of these skills. The user-directed, animated scenarios were the only elements of I'M HAPPY that included drug refusal skills and are likely responsible for the improvement in student perceptions. Previous research has shown that relatable narratives can influence participants by demonstrating plausible pathways for resolving problems.26,27
A full-scale evaluation of I'M HAPPY should compare baseline to postintervention misuse or abuse of prescription or OTC drugs, intention to misuse or abuse, and self-efficacy for refusal. Multiple postintervention measures should be employed to determine the duration of program influence, and a control group should be added. Gender differences could also be studied, as previous work with online prevention has shown greater knowledge gains by girls.23,28
I'M HAPPY was delivered online and almost all students found it easy to use, which met the intended aim of developing a drug prevention program that can be easily disseminated. It is unclear why 14 students (29%) who completed the pretest did not complete the posttest. There may have been technical issues, student withdrawals, or time constraints. The posttest was voluntary and required students to click a link at the end of the module.
The effects of I'M HAPPY on drug-related behavior were not measured; however, a one-time intervention is unlikely to have long-term behavioral effects. It has been noted that 4–12 computerized learning sessions are typically required to measurably lower substance use. 16 Future work may therefore include expanding I'M HAPPY to include additional sessions. It has also been suggested that a program's effects can be amplified by increasing peer interaction. 29 I'M HAPPY could easily be adapted to have student groups work together to solve problems, make choices, and engage in discussion. Development of classroom guides for I'M HAPPY may therefore be a logical and fruitful extension of the work described in this study.
A limitation of this pilot study was that it was only carried out in one school with one cohort. The relatively small number of participants also resulted in low statistical power. Although the program was developed with input from parents and education specialists, the study did not ask for feedback from the health class teachers, who could have provided insight on implementation of the program.
Footnotes
Acknowledgments
The authors gratefully acknowledge Gichin Marsden for approving, coordinating, and overseeing pilot testing of I'M HAPPY; Mike Cottam, Verne Larsen, and other members of the Prevention Dimensions Steering Committee for providing feedback and guidance during the creation of I'M HAPPY; Rod Hopkins for providing input and advice on the student questionnaire; and, Linda Martinez Saville, the staff, parents, and students of the Sandy Club.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a Health Living Grant from the American Medical Association Foundation awarded to E.J.U.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.