
Abstract
Objectives:
Recent studies have established the usage of virtual reality (VR) to help alleviate acute and chronic pain. VR technology can be cost prohibitive and cheaper alternatives are desired. In this study, a Google Cardboard headset ($15) combined with a smartphone was used as a low-cost VR device to assess efficacy in altering the perception of pain.
Materials and Methods:
The cold pressor test, a minimal-risk method, was used to simulate pain. Participants immersed their hands into ice water, with and without VR, in a crossover manner, and their pain perception data were recorded.
Results:
Forty-eight healthy volunteer participants completed the study between 2017 and 2018. Participants were randomized to right hand control, left control, right experimental, and left experimental groups, respectively, before the crossover. Data collected included pain threshold (time at which participants first reported pain), pain tolerance (time at which participants removed their hand), and pain intensity (highest reported pain level on a [1–10] scale). Approximately two-thirds of participants had improvements in pain threshold and pain tolerance with a mean improvement of +13.0 seconds (P = 0.0045) for pain threshold and +29.8 seconds (P = 0.0003) for pain tolerance. Pain intensity had a reduction of 0.43 points (P = 0.0371).
Conclusion:
Our results demonstrate that inexpensive VR devices, such as the Google Cardboard headset used in this study, may be a safe, portable, and cost-effective way to alter the perception and improve tolerance of pain.
Introduction
Pharmacological management of acute and chronic pain with over-the-counter analgesics and opioid use is often complicated by adverse side effects. More commonly, these are constipation, nausea, vomiting, headaches, and dizziness; however, long-term therapy can lead to gastrointestinal bleeding, sleep disorders, respiratory depression, cardiovascular events, addiction, and opioid-induced hyperanalgesia. 1 Nonpharmacological therapies have the potential to provide therapeutic and/or adjuvant treatment for patients experiencing pain. In the acute pain setting, usage of transcutaneous electrical nerve stimulation, acupuncture, psychological distraction (music, video), have shown to be beneficial, 2 whereas in the chronic pain setting, usage of cognitive behavioral therapy, hypnosis, occupational therapy, and physical therapy, have been successful.3–5 Recently, studies have shown immersive virtual reality (VR) therapy as an increasingly effective nonpharmacological method for reducing the level of perceived pain.6–11
The perception of pain is influenced by cognitive function, emotional state, level of attention to pain, and past experience with pain. 12 Because of limited capacity for attention, it is postulated that reducing attention to pain through distractions that engage multiple senses can reduce the ability to perceive pain. 13 It is theorized that VR's ability to provide an immersive distraction allows for less preoccupation with pain. 14 A study by Hoffman et al. in 2004 15 supported this hypothesis through functional magnetic resonance imaging (fMRI) testing where they found that engagement with VR resulted in decreased pain-related brain activity. 16
Recently, there has been rapid growth in research conducted on VR in medical literature, with 131 publications in 2000 to 949 in 2017. 17 Benefits of this technology are found in multiple health care sectors, including physical rehabilitation, stroke rehabilitation, cancer treatments, dental procedures, invasive medical procedures, burn/wound care, phobias, anxiety, eating disorders, and phantom limb symptoms.18–24 VR has also shown superiority to other distraction techniques, including watching television, playing handheld videogames, and listening to music, likely from its ability to provide a more immersive and engaging experience. 25
A significant challenge of implementing VR in clinical medicine is the cost. 22 When VR was first introduced in clinical research, head-mounted VR displays cost several thousands of dollars, which included the cost of the computer system.26,27 It was not until recently that more affordable headsets have enabled more affordable clinical trials in VR.20,22,28 However, literature from early VR studies suggests low-cost VR may be less efficacious than high-quality VR for pain. 29
Given the recent expansion in availability of inexpensive, simple, and portable VR technology, we believe it reasonable to re-evaluate the potential therapeutic effects of low-cost devices as research is limited for new, inexpensive devices. We conducted a study to investigate the effects of low-cost VR on the perception of pain in healthy adults using a headset produced by Google, Inc. (Mountain View, CA), called Google Cardboard ($15), evaluated with the cold pressor task, a validated method of simulating pain in a controlled, minimal-risk trial.30–32
Materials and Methods
Trial design and randomization
With approval from the Mayo Clinic Institutional Review Board, we conducted an open-label, multicenter (Mayo Clinic, Rochester, MN and Mayo Clinic, Scottsdale, AZ), randomized crossover trial from September 2017 to June 2018. The procedures in this study were in accordance with institutional ethical standards and with the Helsinki Declaration of 1975. The aim of the trial was to compare pain tolerance, pain threshold, and pain intensity for each participant with and without low-cost VR. The trial was registered at ClinicalTrials.gov, registration NCT03268863.
After obtaining written consent, participants were randomized to one of four conditions: (1) left hand+Control (VR headset with blank screen), (2) right hand+Control, (3) left hand+Experiment (VR headset with immersive game), and (4) right hand+Experiment. Participants then crossed over to the opposite intervention (i.e., right hand+Control → left hand+Experiment), as shown in Figure 1. This allowed each individual to act as his or her own control. The researchers and participants were unaware of the condition assignments until the trial was initiated.
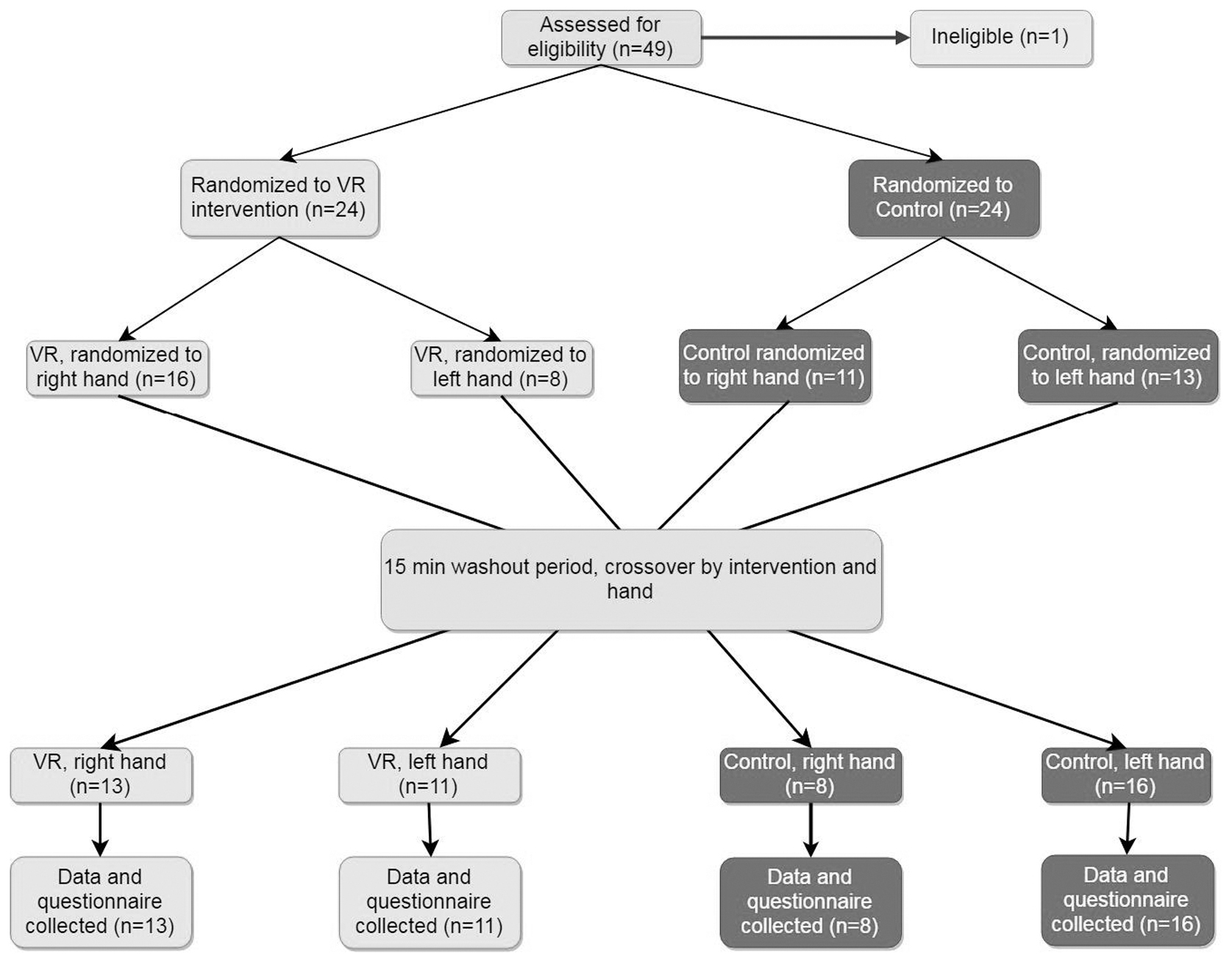
Randomization of original 49 participants using random number generator. One participant was excluded for meeting ineligibility criteria after study was completed.
Participant recruitment
We set a recruitment target of 50 participants for our pilot study to match the sample size of similar VR trials with positive effect.25,32–34 Eligibility criteria were defined as healthy adults between the ages of 18–65 years without history of cardiovascular disease, metabolic disorders, Raynaud's disease, substance use disorders, severe neurological disorders, and chronic pain conditions. 32 Healthy participants were selected for easier recruitment and retention, ability to compare results to similar cold pressor studies conducted on healthy adults, and desire to minimize unnecessary harm on participants with conditions predisposing them to increased pain sensitivity. Participants with known negative interactions with VR were also excluded. Participants were recruited using IRB-approved communication materials. They provided informed written consent and were given the option to voluntarily leave the trial at any time. No compensation or academic incentives were provided.
Study procedure and data collection
We used the Google Cardboard headset, which is an affordable and portable cardboard VR apparatus that accommodates most touchscreen smartphones through which a VR software or game is played (Fig. 2). We chose “InCell VR,” a freely available VR game by NIVAL, Inc. (Moscow, Russia), where players completed a timed track while collecting or avoiding certain objects along the track using head movements. An iPhone (Apple, Inc., Cupertino, CA) was used to run the game software for our study.

Image of Google Cardboard Virtual Reality Headset manufactured by Google, Inc. (Mountain View, CA).
After randomization, each participant was brought to the study room and given instructions through a preformed PowerPoint. Once they confirmed understanding, they were asked to put on the headset with earphones, with or without the interactive game running. Each participant was given 1 minute to acclimate before the cold pressor test began at which the participants submerged their assigned hand up to the wrist in the ice water container kept at a constant temperature of 4°C ± 1°C. Once submerged, a timer was started, and participants were asked to audibly indicate the moment they felt discomfort; this time was recorded and defined as “pain threshold.” The participant then withdrew their hand, as initially instructed, when the discomfort was too great; this time was recorded and defined as “pain tolerance.” A maximum cutoff time of 3 minutes was employed based on previous literature that has shown the average pain tolerance for men to be <150 seconds at 5°C, and <50 seconds for women. 35 In addition, after about 2 or 3 minutes, participants' hands would go numb, dulling perception of pain, allowing participants continue for extended periods of time. 36 Once participants withdrew their hand, they were asked to report their perception of pain from [1–10] using the numeric rating scale (NRS), and reported any side effects such as nausea or dizziness.
For each participant, a 15-minute washout period was kept between the two interventions, chosen based on previous research suggesting that temperature recovery occurred after 5 minutes with no significant improvement after 10 minutes. 36 Also between sessions, the ice water was recirculated and the temperature was checked with a thermometer and adjusted to 4°C ± 1°C as needed. After the washout period, participants switched to the opposite condition. The second phase was procedurally identical to the first phase, and data were collected in the same manner as the previous phase.
Study outcomes
Pain threshold, pain tolerance, and pain intensity measured with the NRS were our primary outcomes. Participant's subjective experience and reported side effects were our secondary outcomes.
Data analysis
A student paired t-test was used to calculate the effectiveness of the intervention by analyzing the difference between each participant's pain threshold, pain tolerance, and pain intensity with and without the intervention. The null hypothesis of each test assumed no difference between the intervention (VR) and control (no VR) portions of the study. An alpha value of 0.05 was used to determine statistical significance. A multivariate test was performed to examine the association of factors of hand dominance, previous exposure to VR, and order of intervention (experimental vs. control) with the pain variables.
For the pain tolerance outcome only, a supplemental analysis was done with a student paired t-test after excluding participants who reached the maximum time cutoff and were deemed pain tolerant.
Results
Participant demographics
Forty-nine healthy adults were initially recruited for the study. One participant was excluded for Raynaud's disease leaving a final count of 48. The median age was 26 (range: 23–61) years, with 24 women and 24 men. A total of 18 participants had previous exposure to VR and 43 of the 48 were right hand dominant.
Primary and secondary outcomes
For the 48 participants, there was a statistically significant mean improvement of pain threshold by13.0 seconds (95% confidence interval [CI]: 4.35–21.71 seconds, P = 0.0045) with VR (Fig. 3). Pain tolerance improved by 29.8 seconds (95% CI: 14.25–45.45 seconds, P = 0.0003) (Fig. 4). Pain intensity measured with a [1–10] NRS had a statistically significant mean reduction of 0.43 points (95% CI: 0.03–0.85, P = 0.0371) (Fig. 5). A graphical representation of the total time duration participants had their hand immersed in the cold pressor test is shown in Figure 6.
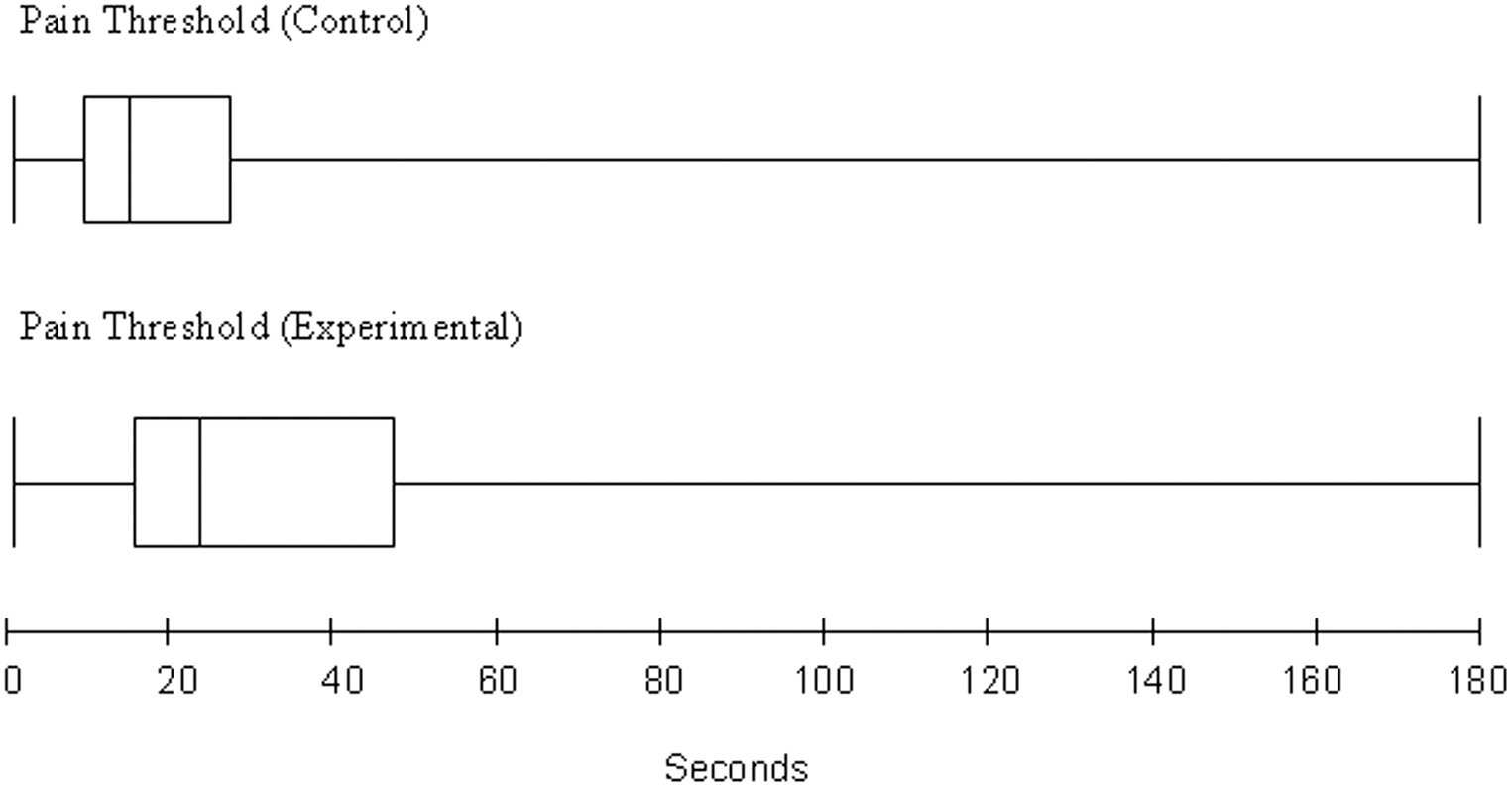
Comparison of Pain Threshold (time of onset to pain) of participants for control (without VR) and experimental (with VR) interventions. The mean time for control: 28 seconds and mean for experimental: 41 seconds. VR, virtual reality.

Comparison of Pain Tolerance (time to removal of hand) of participants for control (without VR) and experimental (with VR) interventions. The mean time for control: 72 seconds and mean for experimental: 101 seconds.
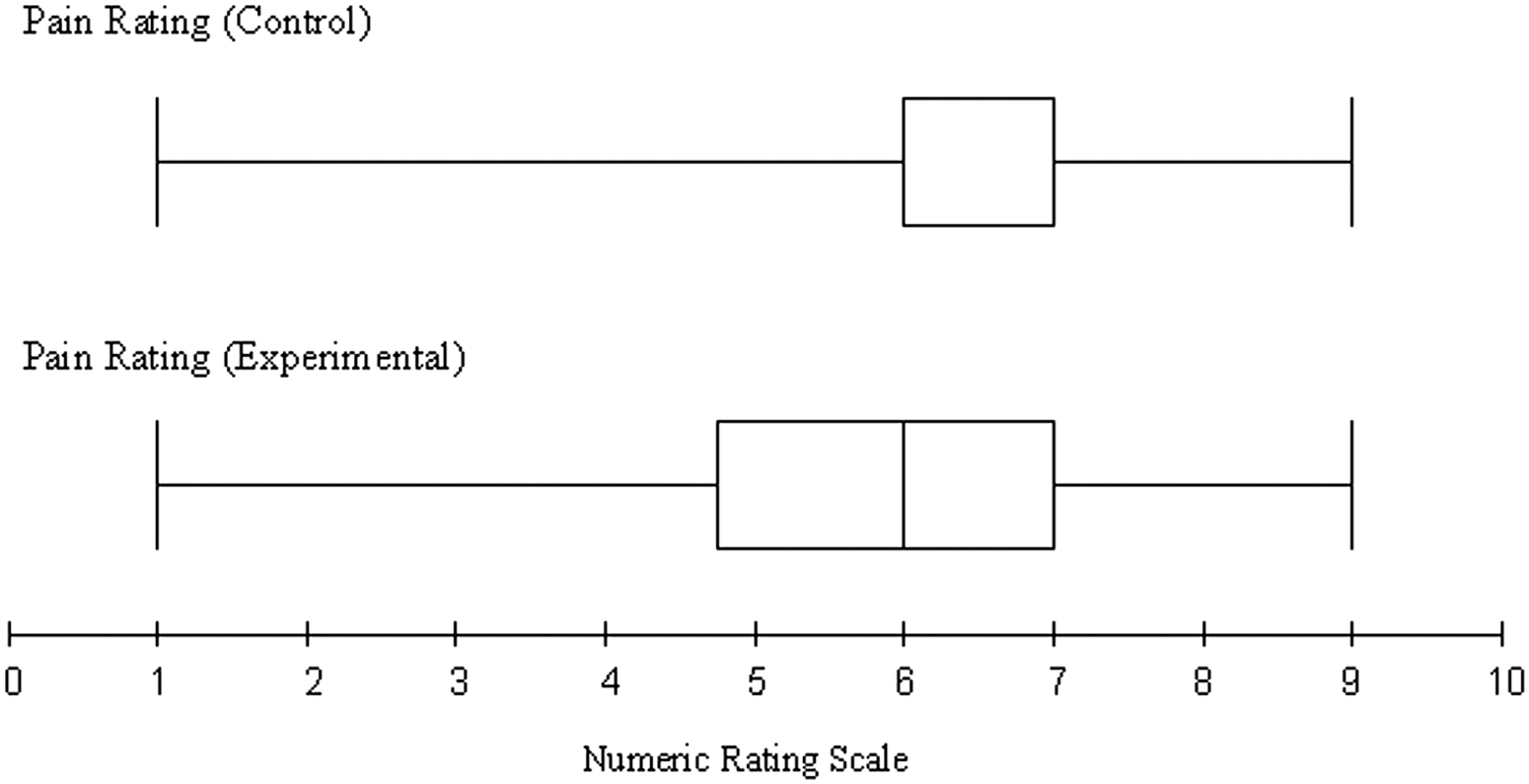
Comparison of Pain Rating (maximum pain felt measured with Numeric Rating Scale) of participants for control (without VR) and experimental (with VR) interventions. The mean for control: 6.3 and mean for experimental: 5.9.
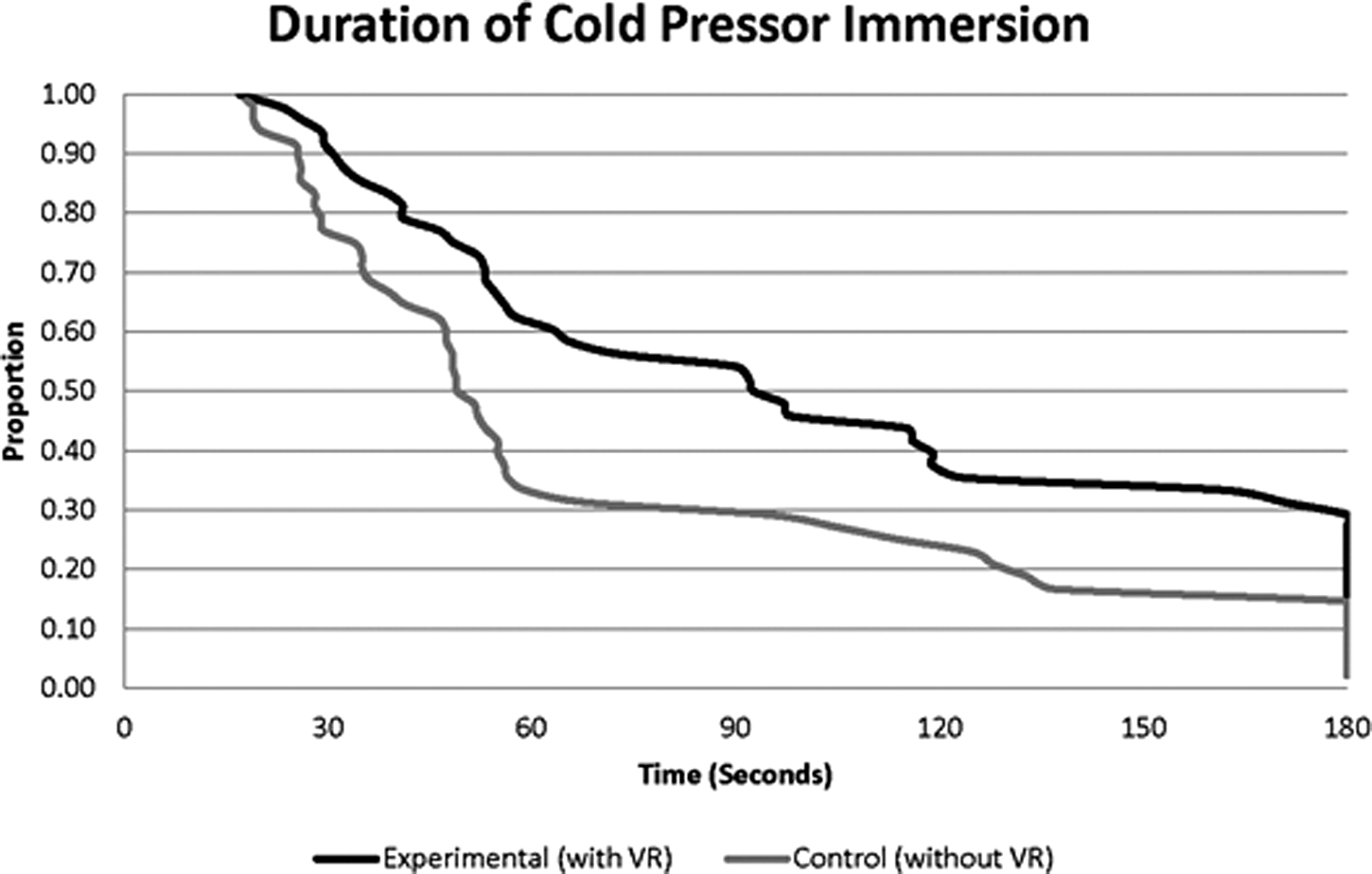
Graph for duration of immersion for control (without VR and experimental [with VR]).
Five participants reached the maximum time limit of 3 minutes on the control and experimental portions of the study. A supplemental analysis performed after excluding these participants demonstrated a pain tolerance mean improvement of 33.2 seconds (95% CI: 16.3–50.2 seconds, P = 0.0003).
Analysis of potential confounding variable
A multivariate analysis of variance (ANOVA) test of covariates analyzing the effects of hand dominance, order of intervention, and prior exposure to VR on pain tolerance (after excluding the five time-limited participants), pain threshold, and pain intensity, found no evidence (P > 0.10) that any of these variables influenced the positive results of the VR intervention.
Secondary outcomes
Two cases of nausea and three of dizziness were attributed to VR technology, none that prompted participants to end the trial early. Some participants also provided verbal feedback of the experience. Overall, participants felt VR may be useful, some comments made:
“I liked the competitive nature of the game” “I was distracted from the pain with virtual reality” “Pain came in waves in the virtual reality”
Discussion
We conclude statistically significant improvements in pain tolerance, pain threshold, and perceived pain intensity in healthy adults, when using low-cost, immersive VR technology while receiving a pain-inducing stimulus through a cold pressor task. Our findings corroborate previous trials and growing body of evidence that VR can help alleviate pain in the acute setting.7,8,16,24,32 We additionally report a subjective satisfaction with the VR experience from participants and a mild side effect profile.
We report improvement of pain threshold in 68.8% and pain tolerance in 66.7% of all participants with a 46.4% increase in mean pain threshold time and 40.3% increase in mean pain tolerance time when using VR. The Hedges g effect size was small (0.31) for pain threshold and medium (0.51) for pain tolerance. The mean pain intensity score had a decrease of 6.3% in mean pain intensity that although statistically significant, did not translate to clinical significance. When analyzing the three variables together, we can suggest that VR may not reduce the perceived intensity of pain but allow one to tolerate pain for longer periods of time. A similar study 32 that employed a cold pressor test to test VR using higher-costing equipment had results of a 73.7% increase in mean pain threshold time, 51.1% increase in mean pain tolerance time, and 3.5% decrease in mean pain intensity. The Hedges g effect size was medium for pain threshold and pain tolerance. This may indicate low-cost VR to be effective, although marginally less so than the higher-cost devices. Since, however, there are no established guidelines for conducting VR studies in terms of game type, audio level, and level of immersion, it is difficult to directly compare our results to other VR trials, as these other factors may influence the results independently of the chosen headset.
Three possible confounders we analyzed using an ANOVA test included hand-dominance, order of intervention, and previous VR exposure. Studies employing a cold pressor test with a control and experimental phase often select between using the nondominant hand for both immersions and switching hands. 31 Our decision to alternate hands stemmed from a desire to avoid any known or unknown physiological changes for pain perception that may come about after the first immersion. However, alternating hands could introduce a potential confounding variable, as it has been found in healthy right-handed males that pain sensitivity was reduced in their dominant hand. 37 Given this, we conducted an ANOVA analysis for hand dominance and pain outcomes and did not find a statistically significant difference. In addition, order of intervention (control or experimental) also showed no difference in reported outcomes, in line with other cold pressor studies.33,38
The cold pressor test provided an acute painful stimulus with resolution of pain once the stimulus was removed. Thus, our study supports VR's ability to improve acute pain likely by creating a distracting environment. Our conclusions also suggest low-cost, portable, VR headsets to be viable alternatives to expensive VR equipment for these acute pain situations where cost is a limiting factor and medications are not desirable. 29 To our knowledge, this is one of the first randomized controlled trials to demonstrate effectiveness of low-cost VR on pain threshold and pain tolerance in healthy adults.
Research in low-cost VR is limited. A systematic review of VR trials in the inpatient setting found 2 of 11 identified trials specifically studied low-cost devices. 6 In one study done in a South African hospital with limited resources, Morris et al. used a low-cost VR device (eMagin Z800 3DVisor; eMagin, Hopewell Junction, NY) that was purchased for approximately$1400 (L.D. Morris, personal correspondence, January 2019) to alleviate the pain perception during dressing changes for burn patients. Nine of the 11 of their patients treated with VR and analgesics (vs. analgesics only) had a decrease of pain of up to 6 points on the pain NRS. 28 Furthermore, in 2018, Ford et al. tested Sunnypeak VR headset (discontinued) that cost $15–$20 (C.L. Duncan, personal correspondence, January 2019) on 10 burn patients during their dressing changes. All of their patients and providers surveyed were satisfied with using VR and 60% of patients stated their pain during the dressing was reduced. 22
We believe that VR technology could provide benefits for patients in multiple settings. First, the technology could help patients in developing cost-limited countries. While the Google Cardboard VR headset does not include the processor and display, the surge of low-cost smartphones, with prices starting around $40, could make VR more marketable and feasible. 39 Currently, there is an expected increase of 1.6 billion new smartphone users in sub-Saharan Africa, according to GMSA Intelligence, Global Trends 2017 Report 12, with 27% of the population using smartphones in 2017 to an expected 55% by 2020. 40 These trends strengthen the notion that cheap VR technology could be a financially feasible option.
Second, simple, cheap, and easy-to-use VR may be useful in the inpatient hospital setting. Two commonly cited barriers to an adoption of VR technology in the hospital setting are crosscontamination and difficulty cleaning the headsets between patients. 10 The Google Cardboard headsets we used in our trial consist of little more than cardboard, two biconvex lenses, and some Velcro to hold a smartphone up to the lens. These can be purchased and produced as disposable medical equipment, eliminating the cumbersome cleaning process and the risk for crosscontamination between patients as long as the smartphone or touchscreen device is wiped with a sterilizing solution.
Several limitations were present in this trial. First, our intervention was not compared with another distraction technique (music, television, etc.) that could have shown a similar effect with pain perception. Second, given the design of the study, we were unable to blind the participants or researchers on the intervention being used. Third, we conducted our research on healthy participants who were primarily students or employees of Mayo Clinic in a controlled environment who are not representative of true patient populations. Lastly, we were unable to analyze gender differences with VR as these data were not recorded with the individual trial data. Of note, VR headsets, including the one used in the present study, have not been approved by the FDA for medical purposes.
While the low-budget nature of our trial lends itself to replicability of our study design, it may have introduced some error. Our cold water apparatus lacked a pump to recirculate the water to keep a constant temperature and the temperature of the water was only readjusted between participants.
Additionally, we used the handheld form of the VR headset instead of a model with head straps, which introduces a difference between our VR trial and many others.
Although the evidence is growing for the potential benefits of VR, there are challenges with implementation of VR in the clinical setting. Undesirable effects, including dizziness, nausea, headaches, eyes train, and lightheadedness, could result. 41 This may prevent usage with patients experiencing or predisposed to these symptoms. Additionally elderly patients, who compose the majority of hospitalized patients, are less receptive to VR compared with younger patients, likely due to unfamiliarity. 10 Patients and health care staff may also have challenges with using the device itself and may believe VR is too bulky or cumbersome to administer in a clinical setting.22,42
Despite these limitations, we advocate for more research in low-cost VR that would be more accessible for patients experiencing acute pain in facilities with limited resources. Further research should also apply VR technology to hospitalized and/or elderly patients that may be more representative of the patient population at large and increase the number of long-term trials on patients with chronic pain. Lastly, VR games and simulations should be evaluated against each other to determine which are more immersive, efficacious, and enjoyable for the patient.
Footnotes
Acknowledgments
The authors would like to thank Dr. Brandon Birckhead, Dr. Janet Vittone, and Dr. Nandita Khera for assistance with supplying the Google Cardboard headset product, mentorship, and guidance in this project. They also like to thank their reviewers for comments that greatly improved the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
None of the authors have conflicts of interest or sources of funding to report.