
Abstract
Sleep deprivation and emotional problems such as stress, anxiety, and depression commonly occur in university students. Exercise is beneficial to ameliorate those problems; however, university students are not serious to take up physical activity. Commercially available exergame such as Xbox® 360 Kinect is one of the alternatives. This study aims at investigating the feasibility and the potential efficacy of using Xbox 360 Kinect game among health care undergraduate students. A pilot two-armed parallel randomized controlled trial was implemented. A total of 36 undergraduate students was recruited and randomly allocated into the intervention group (playing Xbox 360 Kinect) or the control group (continue with normal daily routine). The intervention group received 30 minutes of Xbox Kinect activity, three times per week for 6 weeks. Information on psychology (Depression, Anxiety, and Stress Scale-21) and sleep (Functional Outcome Sleep Questionnaire-30) status was collected at pre- and post-experiment. The researcher-developed feasibility questionnaire was given to the participants in the intervention group at post-experiment. Repeated-measures analysis of variance was used to investigate within-between group comparison, and significance value was set at p ≤ 0.05. The analysis found potential improvement on sleep (p = 0.039) and psychological health (p = 0.002–0.067). The intervention protocol is feasible and highly accepted by the participants. The required optimum amount of dosage, sample size, and the use of outcome measures are suggested from the findings. This pilot and feasibility study supports the use of Xbox 360 Kinect games in practice and to be implemented for future research.
Introduction
University students are the backbone of a nation's future. Maintaining good health is, therefore, necessary. However, university students are burdened with many academic tasks with limited time to do physical activity and are sleep deprived.1–3 University students were reported to suffer from psychological problems such as high stress and anxiety, 4 and these symptoms are worse among health care students. 5 Psychological issues and sleep problem are interconnected: Suffering individuals show worse mental health-related quality of life.6–8 Sleep has an impact on one's ability to carry out activities of daily living effectively. Sleep insufficiency is a public health problem; however, many health care providers do not counsel their clients about healthy sleeping habits.9,10 A proactive active healthy lifestyle is required to help university students maintain good health.
Many studies investigated the intervention on sleep from either a pharmacological approach such as oral melatonin intake11,12 or a non-pharmacological approach such as stress management, sleep hygiene, psychotherapeutic techniques, education, and also environmental adaptation.11,12 Recently, exercise was found to be beneficial in maintaining good health and good sleep hygiene.13,14 However, research shows that exercise activity is difficult to be maintained if the person does not exercise regularly as a habit. 15 Current trends show that working adults and university students lead a sedentary lifestyle and neglect exercise due to limited time available and being too busy working and studying.2,16 Several factors were identified that become barriers for the university student and prevent them from being physically active such as lack of time, social influence, lack of energy, lack of motivation, lack of skills, lack of resources, and fear of injury. 17 Exercises commonly undertaken by Malaysians are outdoor activities such as jogging, badminton, and football/soccer. This requires the individuals to prepare in terms of apparels, equipment, and location outside from the convenience of their house. This again brings another issue on the time required and commitment.
Exergame is one of the alternatives to facilitate active physical activity. It brings the benefit of exercise and the joyfulness element of game under one platform. 18 Exergame has therapeutic value, is effective for improving rehabilitation outcome on physical function, and is cost-effective for use with children and teens as well as in physical rehabilitation. 18 The use of exergame for older people is found to be positive—it encourages physical fitness intake, improves health quality and wellness, and improves social quality.19,20 Exergame was also found to be beneficial and to add positive psychological values such as enjoyment and immersion, while giving adequate feedback and feedforward on psychomotor and sensory (i.e., visual, auditory) aspects. 21 Exergame can have positive effects on reducing depression and elevating positive mood. 22 Games in the exergame are usually interactive, softcore, and not too challenging, thus ensuring positive motivation throughout the game. Many health literature experts supported and recommended the use of exergame as one of the intervention mediums.18–25 Exergame is beneficial, as it can be conducted at one's preferred area such as home or student's hostels. University students comprise part of the population group that are actively involved in gaming activity. 26 However, research using the exergame among adults, especially young adults, seems to be lacking in the literature.
The currently available commercial exergame equipment is Xbox® Kinect. 18 The Xbox Kinect is a hands-free videogaming—where a motion-detected camera is used—that detects full body motion; whereas other commercial exergaming platforms' use of handheld equipment (i.e., joystick or nunchuks) was found to cause injuries due to knocking and slipping from one's hand. 23 Thus, giving an optimal body movement is desired for active physical activity. However, studies investigating the use of Xbox Kinect are limited compared with other exergame such as Wii™ Nintendo® or PlayStation Move.18,25 In addition, Xbox Kinect was investigated with an older population, athletes, people with conditions (i.e., chronic patients, multiple sclerosis, obesity), and children but it was found to be negligible among university students especially at the tertiary level.18,23
Xbox Kinect was also found to be mostly investigated for physical aspects and emerging research on cognitive aspects; however, it was hypothetically beneficial for psychological and emotional well-being but was not properly investigated. 23 No study was conducted on the efficacy of exergame toward sleep. Given the benefits and potential use of exergame, this study aims at investigating the feasibility and the potential efficacy of using Xbox 360 Kinect game among university students. Therefore, the research question for this study is “What is the feasibility of Xbox 360 Kinect to effectively manage sleep and emotion among university students?.”
Methods
Study design
A pilot, two-armed, parallel, randomized controlled trial was implemented for this study. A pilot and feasibility study is important to ensure whether the protocol is realistic and workable, determines sample size, investigates the suitability of the outcome measurements, and evaluates the potential effectiveness of the intervention.27,28 This study received ethical approval (NN-2018-167) from Universiti Kebangsaan Malaysia Research Ethics Committee and protocol is registered with ClinicalTrials.gov (NCT03906396). This study was conducted between February and April 2019.
Participants and procedure
As this is a pilot study, a pre-determined sample size was considered. An optimal number of 12–18 samples per group is required for a pilot study. 29 This pilot study recruited the highest optimal number, and a total of 36 students was recruited. Recruitment was done conveniently during early semester at one higher education institution though poster promotion and flyers distributed manually and online (e.g., WhatsApp). Interested participants contacted the researcher, and screening was done according to specific criteria.
Students were included if they were undergraduates, English literate, and had a body mass index less than 25; students were excluded if they had a condition (i.e., asthma, heart problem) that prevented them from participating in active physical activities, had a known history of mental illness, were visually impaired, and owned any exergame (i.e., Nintendo Wii, PlayStation Move, Xbox Kinect). The recruitment stopped when the desired number (n = 36) of samples was successfully obtained.
The researcher then arranged an appointment to collect demographic information; conduct the International Physical Activity Questionnaire (IPAQ) and baseline data on the outcomes for each participant. Participants were then explained about the study and the probability that they would be allocated to either the intervention or control group, provided with the information sheet, and obtained consent. The participants were randomly allocated to either the intervention or the control group based on the pre-existing random table that was generated by using a computer generator (https://www.randomizer.org/), and the experiment began soon afterward.
The intervention group underwent exergame activity in pairs for 30 minutes per session, three sessions per week for 6 weeks' duration; whereas the control group did not receive anything and continued with their daily routine for 6 weeks. At the end of the duration, data on the outcome measurement were collected and the intervention group was required to answer the feasibility questionnaire. Participation in this study was entirely voluntary, and participants did not receive any monetary incentive.
Intervention
An activity room at the university's hostel was rented for the whole study duration. The room is an enclosed space of a large empty floor and is equipped with air-conditioning. Since the room is large, sometimes it is also half-rented by other students to conduct one's research, which compromises on privacy. The activity utilized Xbox 360 Kinect (Microsoft, Inc.) with the choice of Kinect Sports 1 (six activities: bowling, boxing, track and field, table tennis, beach volleyball, and football/soccer) or Kinect Sports 2 (six activities: golf, darts, baseball, skiing, tennis, and American football) games.
The equipment is placed on a 50-cm-high table, connected to a mini projector (Keruo L7 Smart Projector), and projected to a front wall equivalent to a 40-inches screen (∼1.5 m of distance) (Fig. 1). The participants are free to play any games available within the 30-minute session (Fig. 2). The researcher is available during the session to ensure safety and to operate the equipment without interfering with the participants. The activity was conducted during weekends (i.e., Saturday and Sunday) from morning till evening, and refreshments were provided.

Xbox 360 Kinect setup. Color images are available online.

Xbox 360 Kinect activity. Color images are available online.
Outcome measurement
International Physical Activity Questionnaire
IPAQ is used to evaluate the level of physical activity within the past 1 week. It contains 27 self-reported items, and the score is calculated and categorized as either low, moderate, or vigorous physical activity level. IPAQ is internationally used
30
and has evidence of validity and reliability in Malaysia.
31
The test
Functional Outcome Sleep Questionnaire
Functional Outcome Sleep Questionnaire (FOSQ) is a 30-item instrument measured on a 4-point Likert scale. The FOSQ focuses on functional ability and is related to daytime sleepiness.
32
The score calculation is based on a simple formula, and a higher score indicates a better outcome. The FOSQ has been used with students and has good validity and reliability.
33
The FOSQ has excellent internal consistency (α = 0.95) with a test
Depression, Anxiety, and Stress Scale
Depression, Anxiety, and Stress Scale (DASS)-21 is a screening instrument and outcome assessment that contains 21 items evaluating three mental health components: depression, anxiety, and stress. 34 Total score is calculated by adding the rating on each item devoted to specific components, and a higher score indicates a poorer outcome. It has been used with university students and has evidence of validity and reliability for either use internationally or use in Malaysia. 35 The internal consistency reliability of DASS is excellent (α = 0.94 for overall scores), whereas the construct validity is satisfactory (factor loading >0.3). 35
Feasibility questionnaire
The questionnaire is researcher-developed (M.H.R. and F.W.Y.) and consists of 23 items evaluating the intervention procedure, duration, setting, equipment, time, and preferences on a five-point scale.
Bias management
Blinding of the participants on the intervention might be compromised, as a true placebo effort could not be performed. Nevertheless, several efforts were taken for conducting the experiment in a closed environment and the participants in both groups were instructed to minimize their communication about their participation in the study. However, chances of the participants to share their experiences of involvement during the intervention might occur unintentionally and this is beyond our control. In addition, participants in the experiment group were aware about their existence as the intervention receivers whereas the participants in the control group were aware that they were in the control group as they did not receive any intervention due to the nature of the protocol.
To minimize the effect of contamination, participants in the control group were instructed to continue with their normal daily routine without adding any new active activity (i.e., exercise or playing any exergame) and participants in the intervention group were asked to do the same, except attending the experiment session. The research equipment was kept by the researcher in a secured facility outside the experiment to prevent any misuse. For outcome, the measurements are self-administered; thus, the researcher collected the completed forms, and one independent personnel blinded to the study was hired to calculate the score and computed the data in the SPSS.
Data analysis
Statistical Package for Social Sciences version 22 (SPSS v.22) was used. Characteristics of the participants were analyzed descriptively by using frequency and percentage for categorical data and mean with a 95% confidence interval for continuous data. Outcomes between the two groups were normally distributed (kurtosis and skewness value are within assumption of −1 and 1) and analyzed by using Kolmogorov
As this is a pilot study, the outcome is used to calculate the required sample size, suitable dosage, and utility of the outcome measure by calculating the effect size. Optimal sample size can be calculated from the difference mean between the two groups and standard deviation of each group. 36 Calculations were made by using MedCalc software (https://www.medcalc.org/), considering the power at 80% with a significant level set at 0.05. For intervention utilizing activities, dosage is calculated based on the duration and frequency of the activity. 37
Advanced analysis on the effect size and standardized response mean (SRM) were calculated. Calculation of the effect size was conducted by calculating the difference value of the pre
Result
A total of 36 participants were recruited within a week, and no drop-out was reported (Fig. 3). No statistical differences were found between the two groups (Table 1).
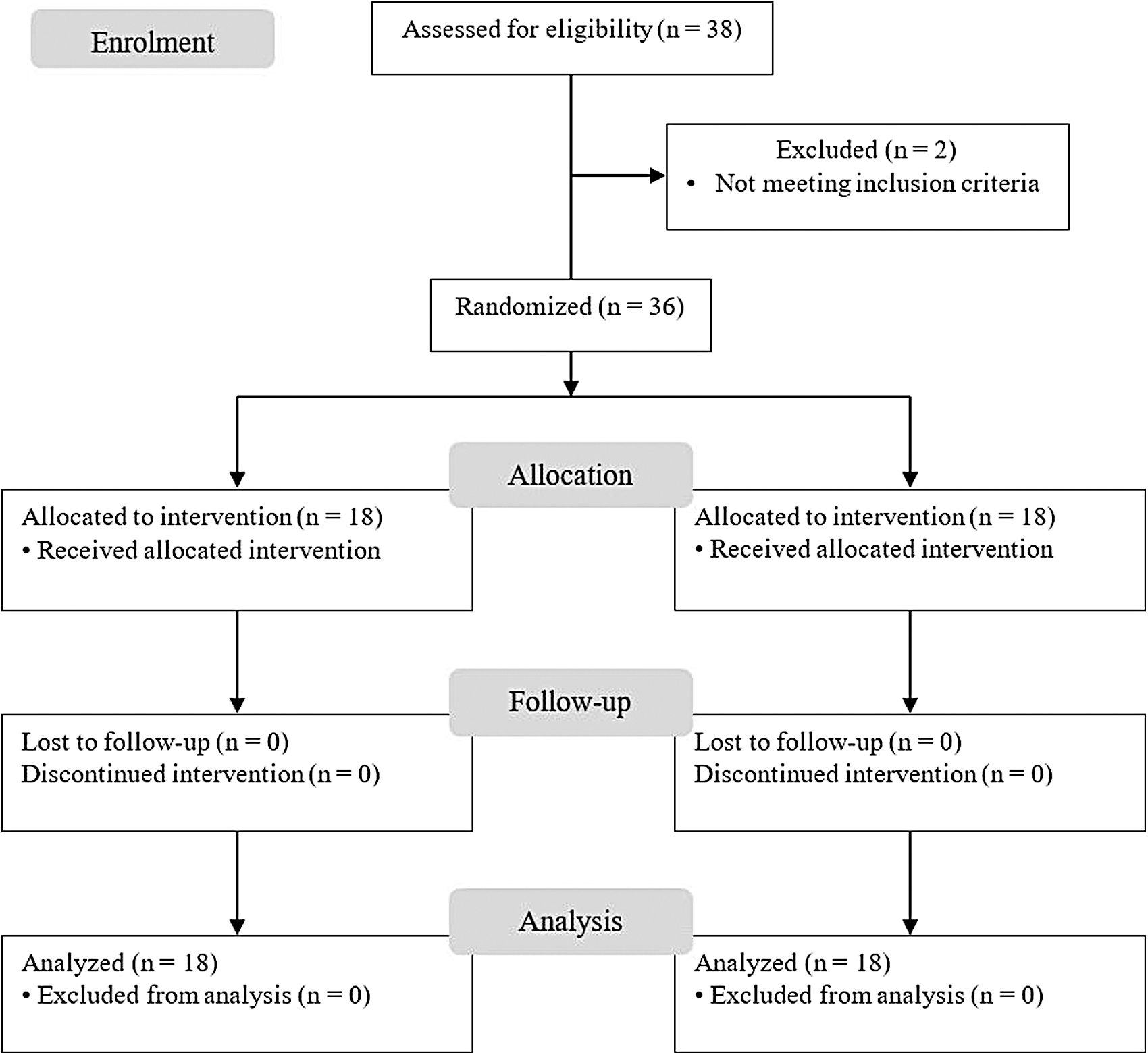
CONSORT flow diagram.
Baseline Differences in Participants' Characteristics Between Groups
Values are mean ± standard deviation, n (%).
Analysis was performed by using the independent t-test.
Analysis was performed by using Chi-square test.
IPAQ, International Physical Activity Questionnaire.
Overall, there is a potential improvement on sleep impacting functions between the control and intervention group before and after the experiment (p = 0.013), and similar patterns were found on psychological health (p = 0.002–0.067). Deeper investigation revealed that all outcomes do have potential improvement in the intervention group after completing the Xbox 360 Kinect activity. No differences were reported in the control group after the study duration. Detailed analysis is reported in Table 2.
Comparison Within-Group (Paired t-Test), Between-Group (Independent t-Test), and Within
p ≤ 0.05.
p ≤ 0.01.
ANOVA, analysis of variance; CI, confidence interval; DASS, Depression, Anxiety and Stress Scale; FOSQ, Functional Outcome Sleep Questionnaire.
For the feasibility aspect, the protocol is generally acceptable (Fig. 4). However, minority considered that three times per week frequency is frequent than ideal (33%), and the duration of 6 weeks is long (11%) or short (6%) than ideal. Visual-related satisfactions (i.e., visibility, lighting) and Kinect camera sensitivity were found to be interfered with.
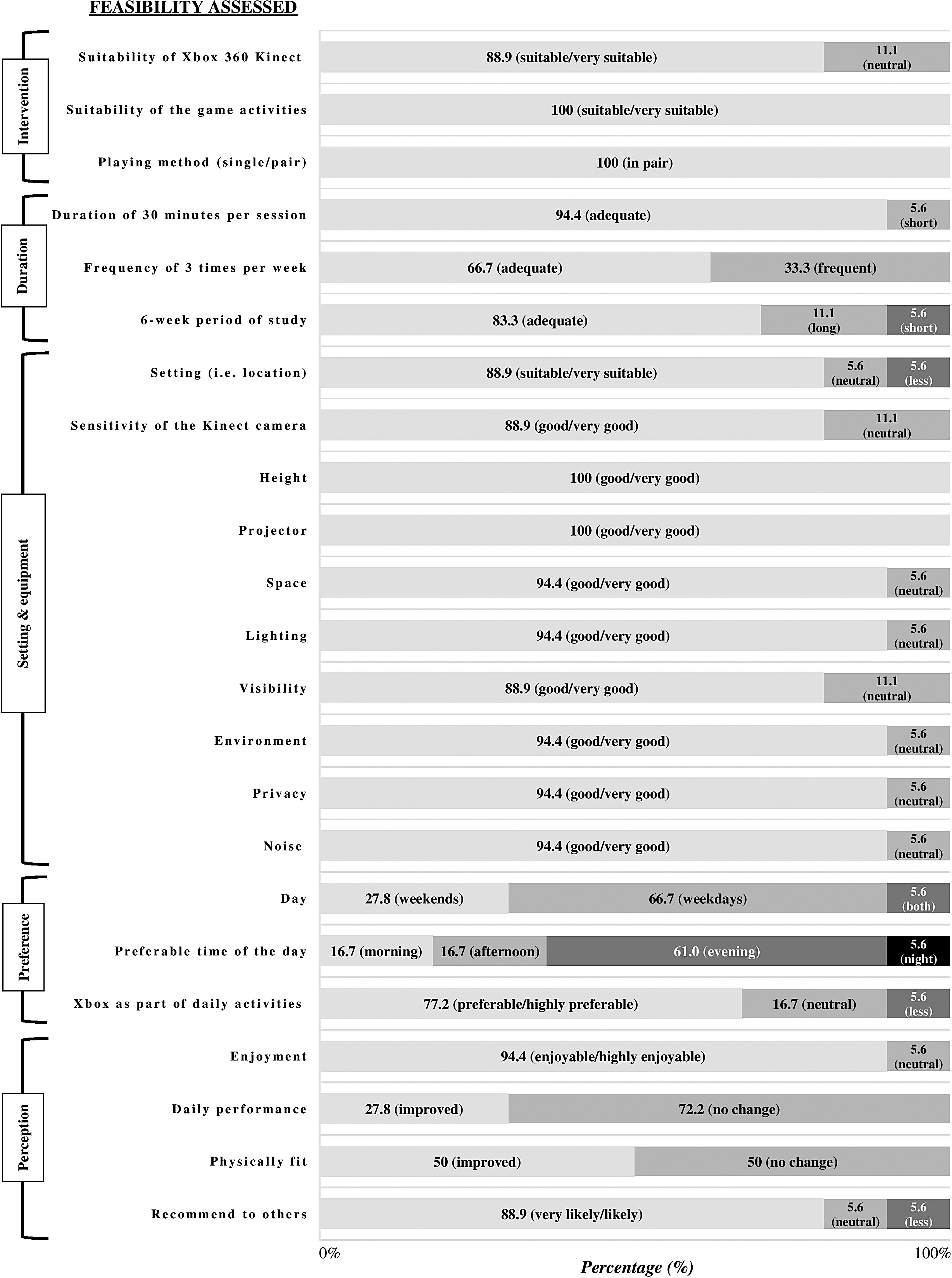
Response on the usability and feasibility of the intervention protocol (n = 18).
Sample size calculation
Sample size calculation indicates a sample between 25 and 105 per arm, with a total of 50 to 210 samples being required for a two-arm trial.
Dosage
Three dosages are considered as optimal based on the difference of the outcomes on the two time points and difference on the significant value, in addition to the response of the participants in the feasibility questionnaire. First, a 45-minute session with 3 sessions per week for a total of between 18 sessions (∼6 weeks) and 33 sessions (∼11 weeks) is suggested to be the most optimal. Second, a 1-hour session with 3 sessions per week for a total of between 14 sessions (∼5 weeks) and 25 sessions (∼8 weeks) and third, a 30-minute session with 3 sessions per week for a total of between 27 sessions (∼9 weeks) and 49 sessions (∼16 weeks) can be considered.
Outcome measurements
The effect size and SRM for emotions in DASS-21 are estimated to be moderate to large and for sleep via FOSQ-30 is large for effect size and moderate for SRM (Table 3).
Effect Size and Responsiveness of the Outcome Measures
SRM, standardized response mean.
Reflection and feedback
Challenges occur in maintaining commitment of the participants due to schedule arrangement. Conducting the activity on weekdays is less possible as the participants are busy with their study responsibility, whereas on weekends they usually return to their hometown. Logistic issues such as limited space and limited choice of games are identified. During week 4, the activity becomes stagnant as participants choose similar games with lighter physical activities involved. Participants' feedback indicated that they enjoyed the activity and it was a way for them to relax from their academic work and to socialize with friends.
Discussion
The effectiveness of exergame using Xbox 360 Kinect to manage emotional issues and functional performance due to sleep disturbance is plausible. Previous studies supported the benefits of exergame on psychological and emotional health.21,22 Exergame has the element of exercise; hence its benefits on sleep were also tangible, and this was supported by a previous review. 13 Literature argued that playing videogames may cause photosensitive reactions such as dizziness, nausea, or seizure39,40; however, our protocol did not notify any prominent adverse effect. Nevertheless, Wang and Reid 41 suggested that virtual reality videogames provided a more secure and safer environment for the participants.
University students were expected to have different exposure toward stress at a different time point throughout the study semester. This may have contributed toward confounding effects on the findings. The recruitment and baseline data collection were done during the early semester. All participants were recruited within 1 week and were evaluated during similar time points. During that time the students recently returned from their holidays and were at the beginning of their study. Their emotional level and sleep pattern were manageable and under control. During the post-evaluation at week 6 of the semester, the students were in the middle of the mid-semester examination; therefore, they needed to prepare for the exams and assignments. University tasks were found to be the factors contributing toward stress among university students. 5 This may have influenced their emotions and sleep pattern. This pilot study indicated that the exergame protocol may have been minimally affected by the factors cited earlier; however, this issue should be taken into consideration in future research.
The protocol of this study allows for the exergame activity to be played in pairs. Potential bias on the outcomes due to social factors may occur. Social factors were found to contribute toward a better quality of life but their role in sleep is limited. 42 Social aspects may become a crucial element to enhance adherence on exergame 18 as supported by the study findings. Exergame activity, similar to other physical activities, has the tendency to be abandoned especially when performed individually. 23 As social factors are a common part of young people's daily living activities, they should be utilized for the benefits of well-being. We believed that the impact of social element is not prominent.
Recommendation for future research
The current protocol of using the Xbox 360 Kinect as an intervention outcome is feasible and is practical for future study. The protocol may enhance university students' behavior to engage in healthy and active exercise as supported by a previous review. 25 User experience on visual aspects can be improved by using a large-size television for clear visibility. The current protocol of using a projector requires for the light to be dim or switched off and this may bring discomfort to the participants. In addition, the use of Kinect Wide-Angel Lens accessories may be beneficial toward reducing the space requirement without sacrificing the comfortability and enhancing sensitivity; thus, more space is available for multiplayer activity. Adding more game choices may prolong the participants' adherence in the experiment and increase their interest and motivation.
Having a good sample size is important for the actual study. Optimal sample size may provide enough power and potential to get significant outcomes, utilize resources optimally, and prevent wastage. 28 A sample size of 30 per arm is recommended and this is within the sample size suggested from the finding. A sample size greater than 25 or 30 is adequate. 43 Further, our recommended sample size is parallel with the calculation by Nitz and colleagues cited in Street et al. 25 Given the logistic issues, the 30 samples are reasonable.
The purpose of a pilot study is to identify an optimal dosage of intervention. Some standard guidelines considered five sessions per week of exercise (with 30 minutes per session) as the recommended frequency; 44 however, the feasibility findings do not permit this for an option. A higher rate of attrition might result in being too frequent. The use of three sessions per week is a reasonable and acceptable practice. 45 Increasing the time duration of the session is the best option as supported by the feasibility outcome and is considered reasonable. The average duration for exercise done by the population is between 30 and 60 minutes per session and for therapy sessions between 45 and 60 minutes.18,44 Cultural aspects in Malaysia that have less appreciation for physical activities need to be considered. 46 Our optimal recommended dosage supported the hypothesis by Street et al. 25 that a longer duration of exergame for more than 1 hour may increase the risk of injuries as shown in many studies that were conducted between 40 days and 12 weeks; hence, increasing the period to more than 6 weeks may increase the risk of drop-out and non-adherence. A protocol with relevant time duration and less burden to the participants is important to ensure low risk of non-adherence among participants.
The use of FOSQ and DASS-21 as outcome measures are found to be responsive and are considered suitable. Although one aspect of the emotional outcome (i.e., depression in DASS-21) was found to be not significant, it is still considered as meaningful and valuable. 47 However, several measures to capture more meaningful outcomes can be considered. Physical fitness assessments (e.g., Eurofit, FitnessGram, Alpha-fit) are recommended, as they are related to physical activity. 48 The aim of FOSQ is to measure functional performance due to sleep problems; thus including assessment focused on sleep quality such as Pittsburgh Sleep Quality Index might be beneficial. 49 Previous studies are lacking in investigating the impact of exergame on quality of life, therefore using a specific quality-of-life instrument such as WHOQOL-BREF is desirable. Huge effect size may occur due to the small sample size, short duration, intensity of the intervention, and the nature of the comparator (i.e., no intervention control group). 50 The active control group is recommended to be implemented: standard exercise protocol—as best available evidence—with a comparable level of Metabolic Equivalent of Task as exergame.
Using healthy subjects may have benefits and challenges. The benefits include less risks, being easier to handle, and being flexible. However, healthy participants may contribute toward a plateau of findings, as their performance already achieved an optimal level. Therefore, improvement is difficult to be detected as the change is small. Other populations such as adolescents, working adults, older people, and people with certain conditions (e.g., obesity, mental illness, cognitive impairment such as dementia, physical illness such as stroke and musculoskeletal injuries) can also be potentially recruited. Adolescence is the period during which emotions develop and seem unstable. 51 This generation is also the one that is mostly attracted to games. 52 In Asian countries such as Malaysia, working adults are reported to face lots of stress from work due to high work burden, overwork, and high personal commitment (i.e., family responsibility, financial). 53 Older people in Malaysia are receptive to illness and have a sedentary lifestyle where physical activity is less appreciated but social activities are highly regarded.46,54 Thus, the recommended protocol from this pilot study can be explored further to other populations.
Footnotes
Acknowledgments
This study is part of the second author's undergraduate research project under the supervision of the first author. The project was originally initiated by the first and third author. The authors would like to thank all participants who voluntary participated in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.