
Abstract
Background:
Interactive videogames (IVGs) have been used to reduce risk of falls in the older adult and improve postural control (PC) outcomes.
Objective:
To systematically review trials that examine whether IVGs training is effective in improving PC and managing falls in frail and pre-frail older adults.
Data Sources:
Four databases were searched, Scopus, Web of science, PubMed, and MEDLINE, from January 2007 to March 2019.
Eligibility Criteria:
Frail and pre-frail older adults aged 65+. Interventions were any Nintendo® Wii™ training. The outcome measures were PC and risk of falls as measured by any validated outcome measure.
Studies Appraisal Method:
The PEDro (Physiotherapy Evidence Database) scale and Cochrane risk-of-bias tool were used by two independent authors.
Results:
Eleven papers were included, involving 388 participants, with a mean age of 79 ± 5.7 years. The mean duration of IVGs sessions was 8.8 ± 3.8 weeks, the mean total number of sessions was 20 ± 11.1 session, and the mean length of training was 44 ± 15.7 minutes.
Meta-Analysis:
IVGs achieved better results compared with traditional exercises and control on the Berg Balance Scale (mean difference [MD] 2.80; 95% confidence interval [CI] 1.21 to 4.39; P < 0.001; I2 = 16%), as well as in the short term on Timed Up and Go (MD −1.23; 95% CI −2.37 to −0.09; P = 0.03; I2 = 0%).
Limitation:
Definitive judgement could not be made due to the variability in training, training duration and outcomes measurement.
Conclusion:
IVGs is a promising modality that has a positive effect on PC but not on the outcome of falls, so it should be prescribed with caution among frail older adults.
Systematic Review Registration:
PROSPERO registration number: CRD42019129611.
Introduction
Postural control (PC) is essential in human movement. Along with proper body posture, it is the basis for the successful performance of daily living activities, such as standing and walking. 1 With aging, PC is affected because of visual, musculoskeletal, vestibular, somatosensory, and central nervous system changes that cause physical and cognitive impairments. 2
The aging population is increasing globally. Thirty-seven percent of the total European population is older than the age of 50. 3 Falls are commonly reported by older adults. They are associated with mortality, morbidity, and limited functionality, and they are considered to be a consequence of poor PC. 4 Approximately 10 million fall-related injuries, with ∼5 injuries per 100 people, have been reported among adults older than 65 years. 5 Fall-related injuries cost the National Health Service in the United Kingdom approximately £2.3 billion per year. 6 Higher costs are associated with frail older adults who need expensive and intensive services. 7 Health care for frail older adults costs the United Kingdom an additional £561 to £2108 per person annually. 8 Indeed, frail older adults are at the highest risk for adverse outcomes, such as falls, disability, hospital admission, or long-term care. The British Geriatrics Society has defined frailty as a “distinctive health state related to the ageing process in which multiple body systems gradually lose their in-built reserves.” 9
For older adults with impaired PC, engagement in aerobic, strengthening, and balance exercises at least twice per week is recommended. 10 A systematic review of the effectiveness of exercise for frail older adults suggested that multicomponent exercise is effective. 11 Recent randomized control trials (RCTs) have found strengthening and balance exercises to be more beneficial than stretching and relaxation exercises for the physical performance of frail older adults. 12 Despite the positive effects of exercise, older adults have found it difficult to commit to exercise programs, because they are perceived as boring and non-motivating. 13 They are also considered monotonous because of their repetitiveness. 14 These factors contribute to limited long-term effects because of dropouts and a loss of interest in completing the exercises.15–17
Technology-based interventions have increasingly been used to help older adults to maintain their heath. Recent studies have found positive physical outcomes from engagement in interactive videogames (IVGs) or exergames. 18 The use of IVG training, particularly in cases of chronic illness, has grown rapidly in the past decade.19–23 The training can be delivered through multimodal approaches that allow for visual and auditory feedback. 24
Most systematic reviews on the effectiveness of exergames have focused on healthy older adults,25,26 specific neurological populations,21,27–29 or both populations.19,30 IVGs have been shown to have positive effects on cognition, 31 physical activity, 32 PC, 26 strength, 33 cardiorespiratory fitness, 34 urinary incontinence, 35 and cerebral palsy in children. 36 However, despite these findings, the use of IVGs is at the nascent stage. 19 In addition, the evidence regarding their effectiveness in older adults is limited. 30 Published systematic reviews have not examined the effectiveness of IVGs in frail older adults. Thus, the aim of this systematic review was to evaluate all studies on the use of the Nintendo® Wii™ in IVG training for improved PC and fall management in frail and pre-frail older adults.
Materials and Methods
Protocols and registration
The current systematic review was registered on PROSPERO with the following registration number: CRD42019129611.
Data sources
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed for this review. 37 The search time frame was January 2007 to April 2019. The goal was to identify recent studies on the effects of IVGs on PC and fall-risk outcomes in frail older adults. Two authors independently performed searches in the following databases: Scopus, Web of Science, PubMed, and MEDLINE. The final search was performed in April 2019.
Search strategies
The search terms were specific to each database. The following is an example of the search terms used in Scopus: exergames OR Nintendo Wii OR Wii balance board OR virtual reality OR Video Games AND postural control OR equilibrium OR balance OR falls OR fall risk AND older adults OR older adult OR frail older adults OR old people.
Selection criteria
The study comprised all English-language articles published between 2007 and 2019 in which an IVG intervention was compared with no intervention or other interventions for improved PC and fall management in frail older adults. The Population, Intervention, Comparison, Outcome and Study type (PICOS) framework was used for this review:
P: Population: Frail and pre-frail older adults aged 65+. I: Intervention: IVGs (Nintendo Wii) to improve PC and fall management. C: Comparison: No intervention, traditional exercises or standard care. O: Outcomes: PC and falls as measured by validated outcome measures. S: Study type: All quantitative studies except case series and case studies.
Determination of frailty in included studies
Frailty can affect body functions, such as gait, mobility, balance, strength, cognition, nutrition, endurance, and physical activity. 9 There is a lack of consensus on the definition of frailty. In this review, it was defined on the basis of the following criteria:
Diagnosis based on validated frailty outcome measures.
Mention of frail or pre-fail older adults in titles or full text of article.
Need for assistance with daily living.
History of falls.
Reported poor PC.
Assisted living or nursing home residence.
The use of these criteria could result in the inclusion of pre-frail older adults who might not progress to frailty.
Participants
The studies comprised male and/or female adults with a mean age of 65 or older. They were described as frail older adults, geriatric, aged, or older adults living in the community, independently, in retirement centers or in nursing homes. Studies that included participants with specific medical conditions, such as strokes, Parkinson's disease, or cognitive impairment, were excluded.
Interventions
The reviewed studies used Nintendo Wii, an IVG, for improved PC and fall management. Specifically, trials that compared the outcomes for IVGs with those for traditional exercise, standard care, control, or no treatment were included.
Outcome measures
Studies that used subjective or objective outcome assessments of static, dynamic, or functional PC or decreased risk for and number of falls in older adults were included.
Quality assessment
The Physiotherapy Evidence Database (PEDro) quality assessment tool 38 was used by both authors. In accordance with Herd and Meserve (2008), 39 the total PEDro score indicated the strength of the study. A total score of ≥6 indicated high quality, 4–5 represented fair quality, and ≤3 indicated poor quality. The Cochrane Collaboration tool was used to assess the risk of bias in the included studies. 40
Data extraction
Two authors screened the trials for eligibility by reviewing the titles and abstracts. If an article title or abstract was deemed relevant, the full text was retrieved for evaluation against the inclusion and exclusion criteria. Any disagreement between the authors was resolved by a third author. A data extraction form was created, and the data were extracted independently by two authors. An example of the data extraction form can be seen in Supplementary Appendix SA1.
Data analysis
A random-effects meta-analysis was performed with RevMan 5.3 software. Three primary outcomes were included: the Berg Balance Scale (BBS), Timed Up and Go (TUG) test, and Falls Efficacy Scale International (FES-I). The purpose was to identify the mean difference (MD) in PC and risk of falls in IVG, conventional intervention, and control groups and to determine the overall treatment effect size. In addition, a sub-group meta-analysis was performed to identify differences in the follow-up times. Heterogeneity was assessed with the I2 index, which has four classification levels: unimportant heterogeneity (0%–40%), moderate heterogeneity (30%–60%), substantial heterogeneity (50%–90%), and considerable heterogeneity (75%–100%). 41
Results
A total of 1540 papers were identified as relevant; 905 were duplicates. After the initial screening, 791 papers were excluded on the basis of the titles and abstracts. The remaining 114 were screened after the retrieval of the full text, and 103 were excluded for failing to meet the inclusion criteria. Detailed information about the 103 excluded studies can be found in Supplementary Appendix SA2. The final review included 11 papers. The selection process for this systematic review is presented in the flow diagram in Figure 1, and the characteristics of the final 11 studies are summarized in Table 1.
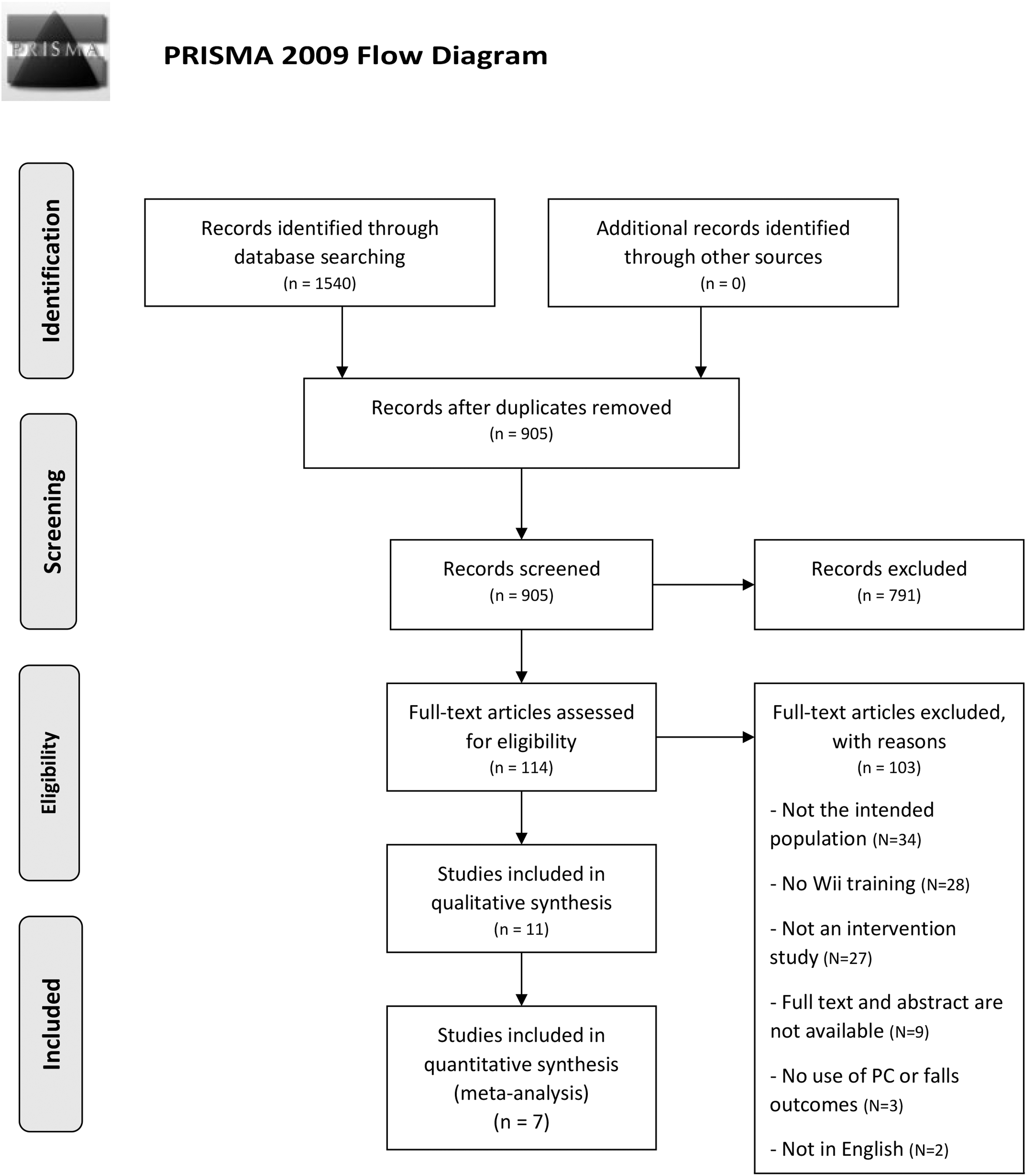
Results of the literature search conducted in April 2019. Adapted from PRISMA statement. 51 N, number; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of Included Studies
BBS, Berg Balance Scale; CG, control group; ex, exercise; FES-I, Falls Efficacy Scale International; IG, intervention group; RCT, randomized control trial; TUG, Timed Up and Go.
Methodological quality
The mean PEDro score was 4.4 (SD = 2.2), with four studies graded as high quality,42–45 four as fair,46–49 and the remaining three as poor quality.50–52 The assessment of the studies on the basis of the PEDro scale is presented in Table 2.
Physiotherapy Evidence Database Scale Assessment for Included Studies
Eligibility criteria are not included in the overall score. 1: Eligibility criteria; 2: Random allocation; 3: Concealed allocation; 4: Baseline comparability; 5: Blind subjects; 6: Blind therapists; 7: Blind assessors; 8: Adequate follow-up; 9: Intention-to-treat analysis; 10: Between-group comparisons; 11: Point estimates and variability.
N, no; Y, yes.
Risk-of-bias assessment
Figures 2 and 3 summarize the risk-of-bias assessment in the included studies.

Risk-of-bias summary: Review authors' judgments about each risk-of-bias item for each included study.
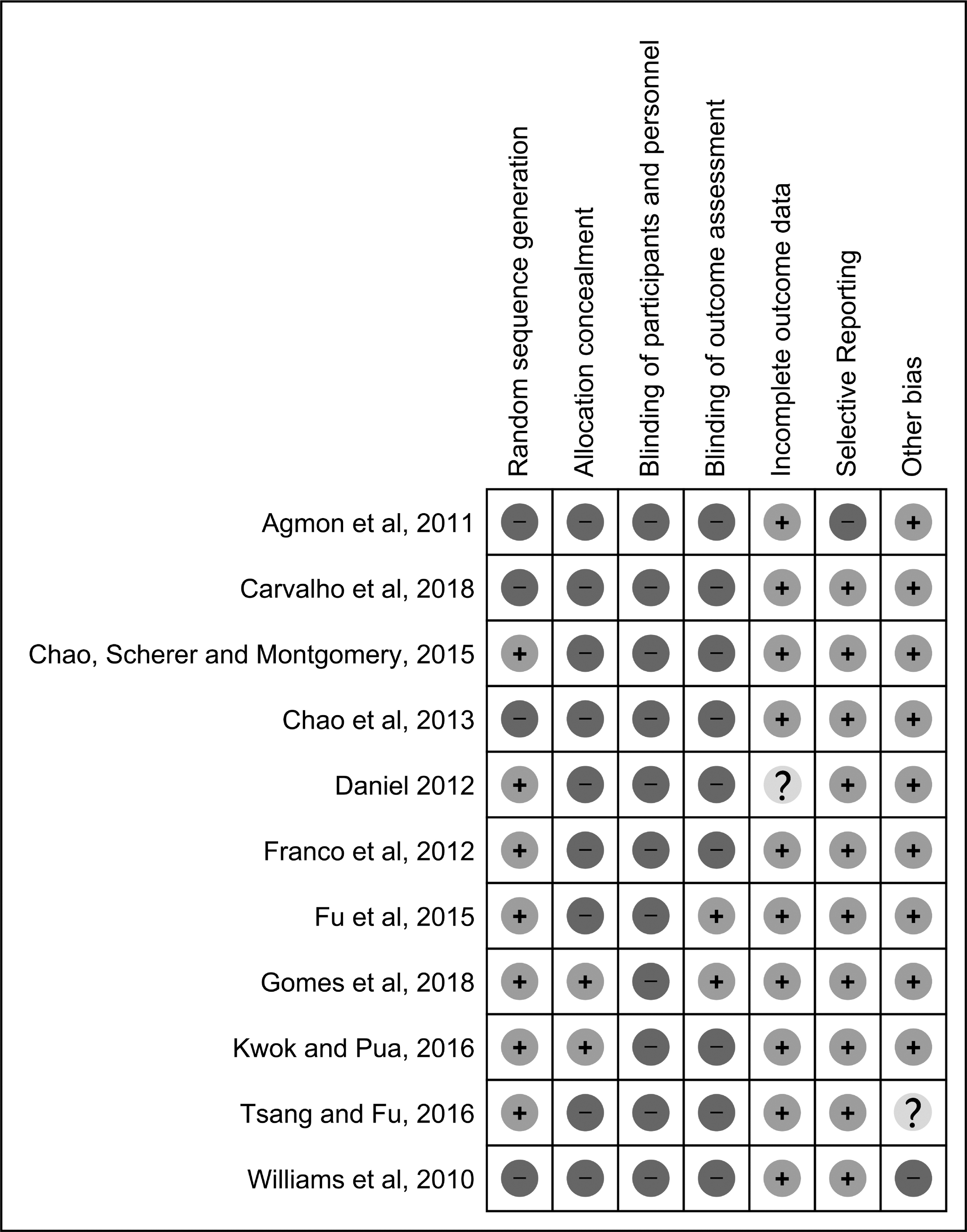
Risk-of-bias summary: Review authors' judgments about each risk-of-bias item for each included study.
Characteristics of included studies
Subjects and designs
Five of the included studies were RCTs42–45,47; the remainder were experimental non-RCTs.46,48–52 The total number of participants in was 388, and the mean age was 79 (SD = 5.7). The IVG groups comprised 255 participants, and the control groups comprised 181. The number of subjects in the IVG groups ranged from 7 to 39, with a mean of 18.2 (SD = 12.2). In the control groups, the number of subjects ranged from 7 to 40, with a mean of 20.1 (SD = 11.8). Most studies were conducted in laboratory settings 46 or living facilities.42–44,49,50,52 One implemented the training in the participant's home. 51
Number and duration of intervention
The duration of the IVGs sessions ranged from 3 to 15 weeks, with a mean of 8.8 (SD = 3.8) weeks. The total number of sessions ranged from 6 to 45, with a mean of 20 (SD = 11.1) sessions. The length of the sessions was 15 to 60 minutes, with a mean of 44 (SD = 15.7) minutes. One study did not report the time spent performing the exercise. 46
Meta-analysis
A total of seven studies were included in the meta-analysis.43–47,49,50 Figures 4 to 6 summarize the overall treatment effect size and the results of each study on the basis of the BBS, TUG, and FES-I.
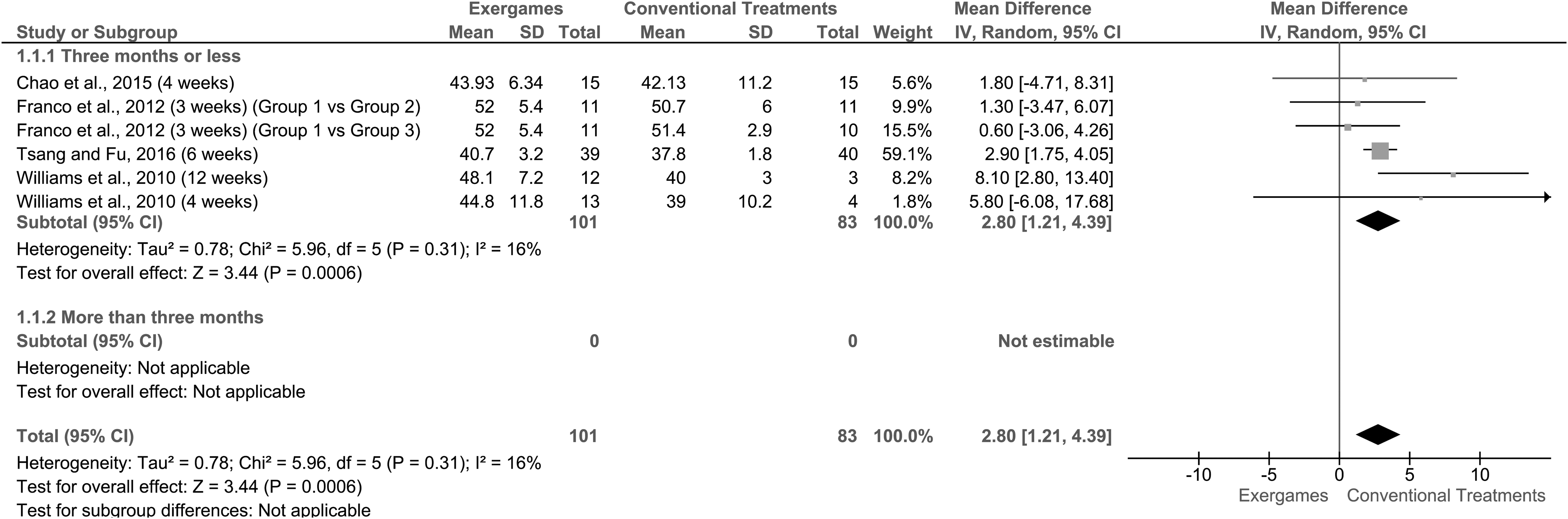
Forest plot for the mean difference of the effect of exergames compared with conventional interventions and control on the BBS; lower BBS mean score indicates higher risk of falling. BBS, Berg Balance Scale.
Berg Balance Scale
Four studies with 184 participants were eligible for inclusion in this meta-analysis.44,47,49,50 A forest plot revealed that on the BBS, IVGs achieved better results than conventional interventions and the control regarding improvements in functional PC (MD = 2.80; 95% confidence interval [CI] 1.21 to 4.39; P < 0.001; I2 = 16%). For the conventional interventions and control, the results of the meta-analysis showed a lower BBS mean score, thereby indicating a higher risk of falling. All four studies assessed the outcome measures within 3 months of the interventions (Fig. 4).
TUG test
Four studies with 277 participants were eligible for inclusion in this meta-analysis.43,44,46,49 The forest plot showed that on the TUG, there was no MD between the IVG groups and the control or other intervention groups (MD = −0.33; 95% CI −0.93 to 0.27; P = 0.28; I2 = 52%). A sub-group meta-analysis showed that IVGs provided significantly better short-term results (<3 months) than other interventions or the control (MD = −1.23; 95% CI −2.37 to −0.09; P = 0.03; I2 = 0%). No statistical difference was found in the longer follow-up time (>3 months; Fig. 5).
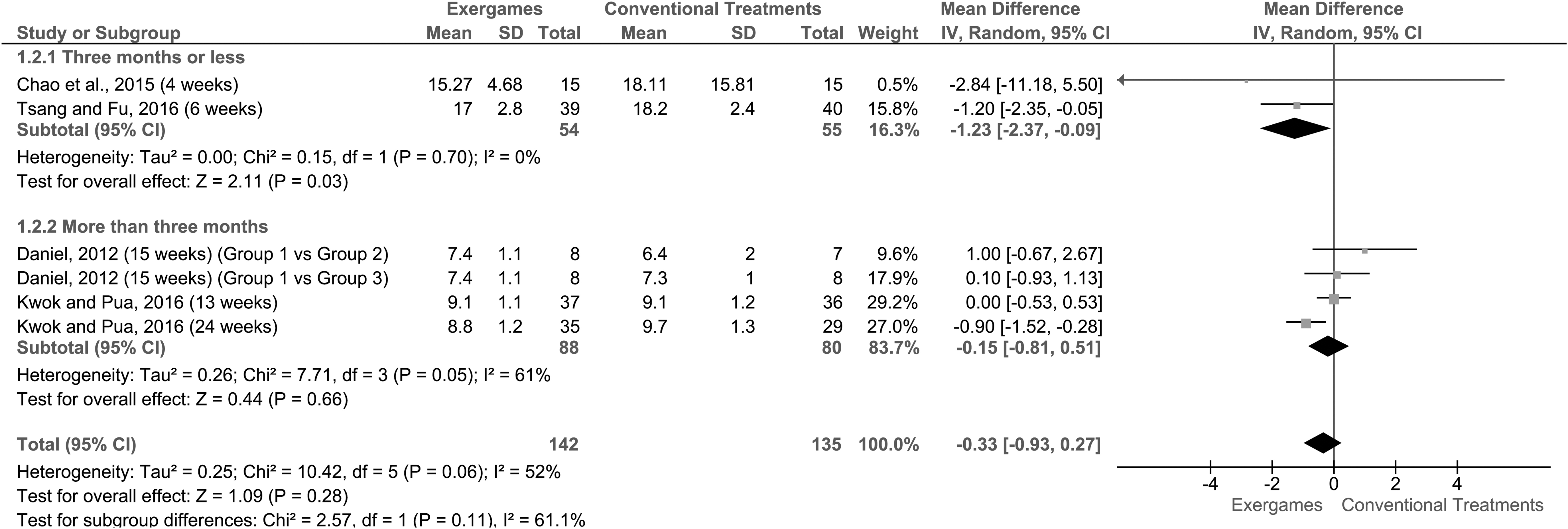
Forest plot for the mean difference of the effect of exergames compared with conventional interventions and control on the time (in seconds) of the TUG; lower TUG mean score indicates better mobility performance. TUG, Timed Up and Go.
Falls Efficacy Scale
Three studies with 122 participants were eligible for inclusion.45,49,50 The forest plot showed that on the FES-I, there was no statistical MD between the IVGs and other interventions or the control (MD = 0.71; 95% CI −3.79 to 5.22; P = 0.76; I2 = 0%). A sub-group meta-analysis found no statistical MD in the short or long term (Fig. 6).
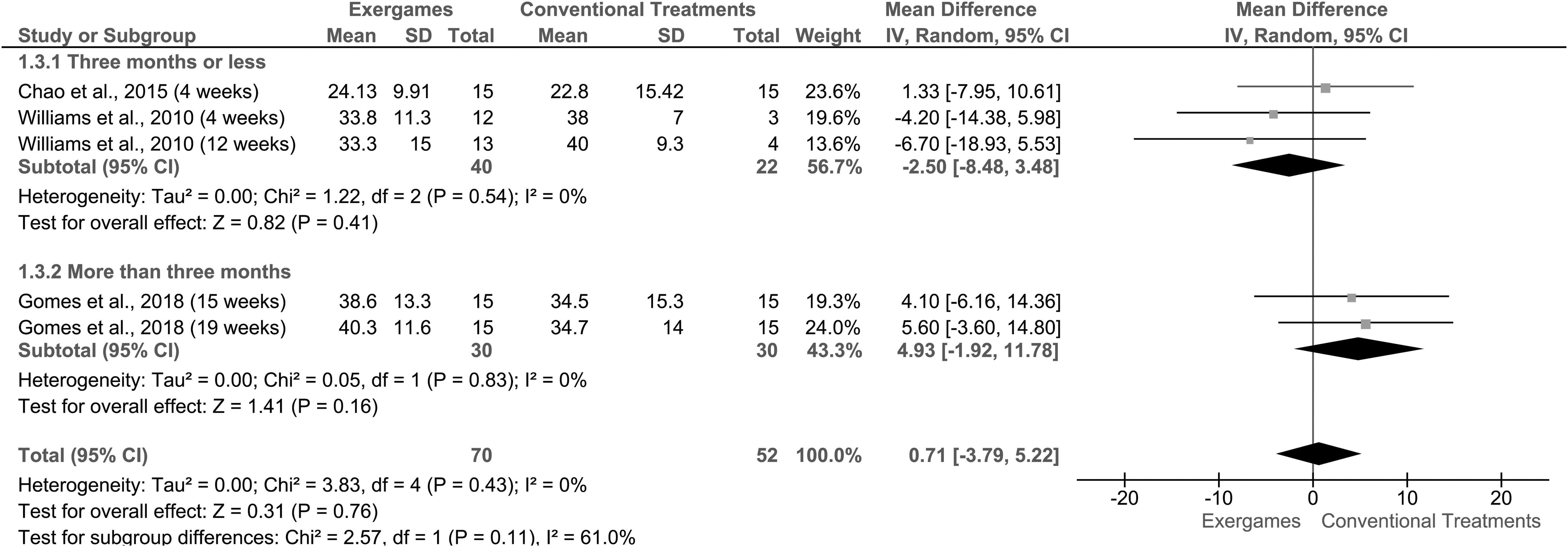
Forest plot for the mean difference of the effect of exergames compared with conventional interventions and control on the FES-I score; lower FES-I mean score indicates lower fear of falling. FES-I, Falls Efficacy Scale International.
Discussion
The current systematic review aimed at retrieving recent studies on the potential effects of IVGs on PC and risk of fall in frail and pre-frail older adults. A few studies have focused on IVG training for older adults. This could be the result of difficulties in using the technology, the novelty of the modality, or the health care workers' lack of knowledge about the use of IVGs in clinical settings. In the included studies, IVGs were found to have positive effects on PC and risk of fall outcomes. This review included studies on frail and pre-frail older adults only. Most of the studies did not specify a criterion for frailty. This lack of consensus regarding the measurements for the identification of frail older adults resulted in variations in participant status.
PC and risk of fall outcomes
The comparisons of IVGs with no intervention showed great variability in effectiveness. Chao et al. 49 found that PC had no significant effects on fear of falling. This could be attributed to inadequate monitoring of the control group, which was encouraged to exercise at home. In addition, the training period, which was only 4 weeks, was short, and the sample size was small. In contrast, Gomes et al. 45 found a significant effect on PC with longer training, 7 weeks, in a laboratory setting. A recent controlled trial with 1016 subjects found that PC training with the Wii Fit™ had no effect. 53 However, there was a difference between the groups in terms of the fear of falling. The study recruited healthy older adults and used one Wii IVG category that focused only on balance training rather than strength, aerobics, and stretching.
Three RCTs that compared IVGs and traditional exercise42,44,47 found significant effects on PC and risk of fall outcomes. The inclusion criteria, training dose, and IVGs were the same for both groups. Fu et al. 42 found a medium effect size, and the latter had a large effect. This variation could be caused by the difference in the research measurements. The first study used a comprehensive PC measurement, the Physiological Profile Assessment, which assesses PC, strength, reaction time, and proprioception. The latter used the TUG and BBS, which assess PC ability only. These positive findings are consistent with those of previous studies on healthy older adults. 25
Kwok and Pua 43 used the Wii games previously examined by Daniel (2012); however, 46 their findings on TUG, modified FES, and number of falls were not significant. First, they used a different type of Wii training, Wii Active, which focused on strength and aerobics training. Second, the control group exercised in a multicomponent program that included balance, strength, and cardiovascular exercises. It has been suggested that training that focuses on multiple physical components, such as strength, aerobics, balance, and flexibility, could improve performance. 11 However, this was the only study with a 3-month follow-up to examine long-term effects. Both groups were asked to perform home exercises for 10 minutes during and after training; however, the retention effects observed in the follow-up could not be attributed to the IVGs or home exercise.
Participation in physical activity training has been found to have positive effects for frail individuals.54,55 The current review supports this claim. The within-group measurements confirmed that IVGs are beneficial for frail older adults with fall and PC problems. However, there were major between-group variations in the studies; thus, definitive conclusions could not be made. Not all of the included studies42–44,46–48,50,51 used multicomponent approaches to addressing PC and falls as recommended.11,56 Hence, the risk of fall outcomes was not significant, because fall management is multifactorial and not limited to exercise. 57
Strengths and limitations
Several types of training are available to improve frail older adults' PC and decrease fall risk. However, regarding the use of IVGs, specifically Wii training, a limited number of high-quality studies have applied rigorous methodologies. The results of this review suggest that frail older adults experienced improved PC. It is worth noting that there was great variability in the sample sizes, assessments, and training doses (duration, number, and frequency of sessions). There were also variations in the definitions and identification of frailty. Risk of falls was often a secondary outcome. A few of the studies examined them as a primary outcome. Thus, conclusions could not be made about the effectiveness of IVGs on risk of fall. One of the included studies used the term “frail” in the title and abstract; however, no clear definition or criteria were provided to confirm the frail status of the recruited older adults. 42 This affected the generalizability of the results. This diversity could be attributed to the lack of consensus about frailty measurements. 58 Most of the studies used the BBS to measure the main PC and risk of fall outcomes. However, recent reviews have not supported the exclusive use of the BBS for fall prediction. 59 A comprehensive assessment, such as the Balance Evaluation Systems Test, could reflect changes in PC. 60
The strengths of the current review include the focus on IVGs that used only Wii training, which features multicomponent exercise (balance, strengthening, stretching, and aerobics), which has been recently recommended for improving outcomes in frail older adults. 11 All four studies45,49,50,52 that included multicomponent exercise found a significant improvement in PC outcomes. Wii trials were included only to differentiate between commercial and non-commercial IVG devices. A recent review indicated that the inclusion of both types of devices could result in evaluation bias. 19
Recommendations
Future studies should investigate health care providers' perceptions of the use of IVGs in older adults to determine the willingness of clinics to adopt this modality. In addition, a standardized protocol that addresses the limitations found in this review should be considered to avoid variability in future trials. Moreover, the use of a standard definition or measurement, especially validated tools such as the Fried frailty index, to identify frail older adults should be considered. 61
Conclusion
The Grading of Recommendations Assessment, Development, and Evaluation system was used to evaluate the quality of the evidence. The BBS, TUG, and FES-I scores did not lead to a strong recommendation for IVGs. IVGs are a promising modality with positive effects on PC but not risk of fall; therefore, caution is needed in prescriptions for frail older adults.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.