
Abstract
Objective:
The benefits of exergaming on executive function in children have been increasingly reported; however, weight-dependent effects of exergames on executive function, and inhibitory control in particular, remain poorly understood. We examined performance on an inhibitory control task at baseline and following acute bouts of exergaming in children who varied in weight status.
Materials and Methods:
Forty 8–12-year-old children with obesity (n = 20) and normal weight (n = 20) performed neutral, congruent, and incongruent conditions of a Victoria Stroop Test (VST) before and after exergames through an Xbox One in an elementary classroom. We measured time spent in moderate-to vigorous-intensity activity through ActiGraph accelerometers and recorded gameplay time.
Results:
At baseline, children with obesity relative to their normal-weight peers had significantly longer reaction times (P = 0.011), resulting in significantly longer completion time (P = 0.005) during incongruent trials requiring greater inhibitory control, and therefore had higher interference scores (P = 0.024). However, following acute bouts of exergames, children with obesity compared with their normal-weight counterparts significantly decreased completion time (P = 0.013), made fewer errors (P = 0.012) during incongruent trials, and subsequently had reduced interference effects (P = 0.037). Children with obesity and normal-weight children spent similar time (minutes) (7.8 vs. 8.6, P = 0.725) in moderate-to vigorous-intensity activity during similar gameplay time (8.7 vs. 10.5, P = 0.819).
Conclusion:
Our results suggest that greater, acute cognitive gains occur in children with obesity relative to normal-weight children following similar intensity and duration of exergames, which may be due to reduced inhibitory control capacity at baseline in childhood obesity.
Introduction
The prevalence of childhood obesity has gradually increased across recent decades, and currently one in three children in the United States is overweight or obese. 1 Obesity is defined as excessive fat accumulation that adversely affects physical, social, and emotional health, 2 and influences healthy growth and pubertal development 3 in children. More importantly, childhood obesity has been linked to impairments in executive functioning, which controls and regulates cognitive operations underlying goal-directed behaviors essential for optimal learning and scholastic performance. 4 Furthermore, children with obesity often remain obese into adolescence and adulthood. 5 As such, the time spent in elementary school, a critical period of rapid growth in physical, cognitive, and motor development, requires healthy behaviors such as sufficient physical activity and maintenance of a healthy body weight.
The role of physical activity in protecting against childhood obesity is well documented; however, the rate of physical activity engagement begins to decline 6 and differs by weight status 7 around age 7. Currently, the majority of U.S. children (75%) are insufficiently active. 8 Of the known methods (e.g., curricular physical activity in physical education) for increasing the amount of active time in school, other types of physical activity (e.g., in-classroom, during recess, after school) have been examined and may constitute an effective strategy for providing additional opportunities to increase physical activity levels, 9 ultimately contributing to the recommended amount and intensity of daily physical activity. 10
Many available technology resources have been used for a school-based physical activity, which affords the opportunity to examine the effects of such physical activity on executive function, classroom behavior, and academic performance.11–13 Exergaming is defined as “interactive videogaming that stimulates an active, whole-body gaming experience.” 14 Exergames through a Kinetic sensor on a game console have been used as an alternative to children's physical activity in the school environment15,16; however, the cognitive effect of exergaming has been less examined in a school setting.
Executive functions refer to a set of cognitive processes, consisting of three core components, including inhibitory control, working memory, and cognitive flexibility, which enable planning, problem-solving, flexible reasoning, and behavioral regulations. 17 Inhibitory control is a central component of executive functions and involves the ability to suppress or control prepotent responses as well as to resist interference from distracting stimuli.18,19 Inhibitory control and other components of executive function (e.g., working memory, cognitive flexibility) are linked to academic success. 20 Researchers have evaluated inhibitory control performance among children using different types of Stroop test, 21 which have been widely used with traditional physical exercise in a laboratory setting, but have not been used with exergames in a school setting.
Exergames that involve short bursts of moderate or vigorous activity22,23 are associated with acute cognitive enhancement,24,25 which is probably due to the physical activity effects. Increasing evidence suggests that acute cognitive benefits mostly related to prefrontal-dependent executive functions are elicited by short bouts of traditional aerobically physical exercise. 26 These benefits may derive from acute physiological changes in brain-derived neurotrophic factor (promoting neuroplasticity), 27 dopamine (carrying signals between brain cells), 28 and cerebral blood flow (maintaining proper brain perfusion) in response to physical exercise 29 that are known to act as mediators for the increased brain activation underlying executive function.
However, to our knowledge, little is known about how weight-dependent effects following acute bouts of exercise or exergames may differentially modulate physiological changes or executive functions especially in children. Furthermore, the cognitive gains associated with these physiological changes may be greater after a more intense level of physical activity. 30 Results from our recent work in children 22 and adults in their early twenties 24 found that both age groups spent time predominately in moderate-to vigorous-intensity activity (as measured by accelerometers) during short bouts of exergames, suggesting that exergaming is physically exerting enough to facilitate cognitive benefits.
In addition to physical activity effects, several studies have indicated that cognitive engagement involved in exergames might play a mediating role in performance on executive function tasks. Benzing et al. 31 recently compared different levels of cognitively engaging exergames in adolescents and found that more cognitively demanding exergame produced better performance on their executive function measures compared with less cognitively demanding exergames. Furthermore, Flynn et al. 32 compared the effects of cognitive and physical engagement on executive function in children and speculated that children playing a cognitively engaging exergame or sedentary videogame improved executive functioning performance more than those who engaged in an exercise condition (stepping) or a nonplaying control condition. However, Best 25 found that, regardless of cognitive engagement, physical activity delivered through exergames was only a significant factor enhancing children's executive function ability to resolve interference from conflicting visuospatial stimuli. As such, the findings from these studies suggest that both cognitive engagement and physical activity involved in exergame play may underlie the acute effects of exergames on executive function.
Given that some researchers have proposed that childhood obesity is linked to cognitive deficits,33–35 the level of executive functioning in response to physical exercise may vary as a function of childhood weight status. Drollette et al. 36 recently measured inhibitory control performance after an acute bout of exercise (i.e., moderate walking) in children with different inhibitory control capacity (low vs. high) and found the cognitive gains were larger in children with lower inhibitory control capacity. This result suggests that the acute cognitive effects of physical activities delivered through exergames may be larger in children with obesity if children with obesity possess a relatively lower capacity for inhibitory control at baseline. In cross-sectional studies, an inverse relationship between obesity and executive function often has been reported for children35,37; however, the acute effect of physical exercise delivered through exergames on executive functions in children of different weight statuses is less understood. It is therefore important to examine the extent to which executive function in children of different weight status is affected by acute physical exercise delivered through exergames.
Currently, a paucity of literature exists regarding the effects of exergames on executive function in children of different weight status. We therefore examined (1) relationships between childhood obesity status and inhibitory control at baseline and (2) the weight-dependent effects of acute bouts of exergames on inhibitory control. We hypothesized that the differences in children's weight status (normal weight vs. obesity) would differentially affect inhibitory control performance due to differences in baseline executive functioning capacity. Our findings aim to provide insight into the effect of childhood obesity on the acute exercise/cognition relationship.
Materials and Methods
Participants
We collaborated with a local elementary school in the Greater Boston area to recruit 8- to 12-year-old boys and girls of different ethnic backgrounds from 10 third-to sixth-grade classes in the after-school program. Before testing, parents mailed a completed questionnaire (we previously mailed) to report their child's demographic characteristics (including date of birth, sex, and race), handedness, height, and weight, as well as measures of socioeconomic status (SES; i.e., parental education level, annual household income). Parents also reported whether their child had ever been diagnosed with an attentional disorder or other neurological disorder, was taking medications affecting the central nervous system that may interfere with study assessments, had any mobility limitations, or had previous experience playing the exergame used in our study. We used this information to determine whether children met our inclusion criteria, which consisted of “no” responses to all of the questions. Using the parental reports of height and weight, we estimated body mass index (BMI) percentile and categorized children into either normal weight or obesity status. On the day of the participant's visit, we confirmed the pre-estimated BMI percentile using an objective assessment of height and weight. We assessed whether participants met the inclusion criteria through a health screening before their study participation. All participants assented and their parents consented to participate in the study, which was approved by the Institutional Review Board of Northeastern University.
Procedures
We conducted our data collection in a classroom at the participating elementary school. After school had ended for the day (around 3 pm), we set up an Xbox console connected to a smart board in the classroom for the data collection. Once a participant arrived in the classroom, we provided the participant with an orientation to the study procedures. We measured the participant's height and weight. Based on the calculated BMI percentile from the measured height and weight, we categorized participants into one of two groups as follows: normal weight (BMI percentile <85%) or obese (BMI percentile ≥95%). Next, we affixed devices for the measurement of heart rate and physical activity to the participant and then carried out cognitive assessment before and after the participant performed the exergaming sessions. Data were collected with a single participant per day, with a single visit of ∼1 hour required for this study.
Measures
Exergame and game console
We used an Xbox One console (Microsoft, Inc., Redmond, WA, USA) connected to a Kinect camera monitor sensor. The sensor enables a user to project his/her body onto the screen to keep track of the position of their body during gameplay. We chose a fitness-based exergame called Shape-Up (Ubisoft, Montreal, Canada) comprising a number of minigames; however, we used five minigames (Stunt Run [running, jumping], Piano Step [side stepping], Waterfall Jump [jumping, surfing], Squat Me to the Moon [squatting], and Volcano Skate [skating]) because these games primarily required lower-limb movements capable of eliciting greater amounts of energy expenditure at a moderate- or vigorous-intensity level. 22 The order of the exergames was random, with each exergame lasting ∼90 seconds and the period between games taking around 15 seconds for the switch to occur. During gameplay, a participant could stop the game at any time or control his/her pace during gameplay, both of which reflect children's naturalistic movements when engaging in school-based physical activities. 38
Anthropometric measurement
We measured height (to 0.1 cm) using a ShorrBoard (Weight and Measure, LLC, Olney, MD, USA) and weight (to 0.1 kg) using a SECA scale (SECA, Inc., Chino, CA, USA) and then computed BMI (kg/m2). We also obtained a participant's BMI percentile using the Centers for Disease Control and Prevention BMI-for-age growth charts. 39
Executive functioning assessment
We used a computerized Victoria Stroop Test (VST) 40 as a brief version of the original Stroop test to measure the ability to inhibit irrelevant interfering stimuli. 21 The VST consists of three conditions: “Dot,” “Word,” and “Interference” corresponding to “neutral,” “congruent,” and “incongruent” of the original Stroop test. Each condition includes 24 trials, colored in blue, green, yellow, or red; and the 24 trials were randomly distributed in four rows of six items on the computer screen. All participants used the same laptop computer with Microsoft Windows 10 and its keyboard to perform the selections. The participants used the keys 1, 2, 3, and 4 corresponding with the colors red, green, blue, and yellow for the VST. Before administering the VST, we explained the procedure and provided several practice trials. We asked participants to respond as quickly and accurately as possible by selecting the color of the dots (the neutral condition), the color of the ink which was presented as neutral words (the congruent condition), and the color of ink which did not match with color names (the incongruent condition) during the 24 trials of each condition. The VST requires participants to correctly complete the 24 trials of each condition to proceed to the next condition; thus, we measured the completion time (seconds) and the number of errors (score) for each condition as well as the reaction time (mseconds) for each item. We then computed two interference scores: (1) the ratio of congruent completion time to neutral completion time (low interference), and (2) incongruent completion time to neutral completion time (high interference). 21 The single VST took less than 5 minutes.
Physical activity, exertion, and heart rate assessments
We fitted the participant with two tri-axial GT9X accelerometers (ActiGraph LLC, Pensacola, FL, USA) on the nondominant wrist with a silicone wristband and at the anterior axillary line of the nondominant hip with a belt clip. 22 From a hip-worn accelerometer, we obtained total steps taken; and computed the time spent in moderate or vigorous intensity of physical activity using activity counts based on the Butte's cut-points. 41 We also placed a Polar H7 Bluetooth heart rate sensor (Polar Electro, Inc., Lake Success, NY, USA) below the participant's chest with a soft textile strap to detect continuous heart rate during the testing session and to send signals through the Bluetooth to a wrist-worn accelerometer. We then obtained heart rate data at 10-second intervals from the wrist-worn accelerometer and converted the values to beats per minute (bpm). We collected the participant's heart rates and rating of perceived exertion (RPE, category range: 0–10) 42 before and after exergames as well as before cognitive testing. As changes in heart rate might be related to weight status during gameplay, 22 accelerometry-based intensity and volume were prioritized to determine exercise intensity.
Data analysis
We completed our data collection with 45 participants. Of the 45 participants, 5 participants were eliminated from data analysis because they were identified to be overweight range (85 ≤ BMI% < 95%), and the present study sought to investigate children with obesity compared with normal-weight peers. 39 We therefore included 40 participants for data analysis; and we divided them into two groups based on the participants' BMI percentile: (1) 20 normal-weight children and (2) 20 children with obesity.
We conducted our statistical data analyses using Stata/SE 14.2 (StataCorp LLC, College Station, TX, USA). For the group differences, we used chi-square (χ 2 ) tests to assess the distributions of demographic categorical variables (i.e., sex, race) and independent t-tests to assess the demographic, exergaming continuous, and baseline VST variables. Furthermore, we tested the validity of VST variables using the Pearson correlation coefficient and found all variables were significant (P < 0.01) with the range of the correlation coefficients (0.5–0.9), except for incongruent error in the pretest, which suggests that the VST variables were valid. We employed Cronbach's alpha tests to measure the reliability of the VST variables for reaction time, errors, and time taken to complete the test separately for pre- and post-test, and found Cronbach's alpha values to range between 0.6 and 0.9, which represents an acceptable level of reliability. We also used canonical correlations to assess associations between VST variables at pre- and post-test, specifically for reaction time, error, and time taken to complete the test and found that the test–retest reliability coefficients were within the range 0.7–0.9, which indicates a good or excellent level of reliability. A participant's SES level was then calculated to generate a total parental SES score using the Hollingshead index (i.e., parental education level, annual household income). 43
Furthermore, we performed repeated-measures analysis of variance (ANOVA) with normal-weight children and children with obesity as the between-subjects factor. The pre–post heart rate and RPE were analyzed separately using a 2 (group: normal weight, obese) × 2 (time; pre-, post-exergaming) model. Also, VST reaction time, response accuracy, and completion time were separately analyzed using a 2 (group) × 2 (time) × 3 (condition) models. Additionally, analysis of interference was performed separately using a 2 (group) × 2 (time) × 2 (interference) model. We assessed main and interaction effects and reported partial η 2 ; and estimated effect size for further reporting. Secondary analyses examined group differences in the dependent variables within each compatible condition using unpaired t-tests and the time effect on dependent variables within each group using paired t-tests. We set our significance level at P < 0.05 and reported means and standard deviations for all continuous dependent variables.
Results
Participant characteristics
The demographic variables, including age, sex, race, and SES were not significantly different between groups, implying that the variables were reasonably well balanced (Table 1). Also, more details of the SES components are presented in Supplementary Table S1. The mean weight, BMI, and BMI percentile were significantly greater in obese children than normal-weight children (all, P < 0.001) as shown in Table 1.
Mean (±Standard Deviation) Values for Normal-Weight and Obese Children's Demographic Information
SES represents a total score of education and income in the household.
BMI, body mass index; SES, socioeconomic status.
Physical activity, exertion, and heart rate in response to exergaming
As shown in Table 2, we observed no significant differences and small-to medium-effect sizes in all indices of the exergaming performance, including in the number of mini exergames, the duration of total exergame activity, total steps taken, and time spent in moderate or vigorous exergaming intensity level between groups during game play. Also, both children with obesity and their normal-weight counterparts had a similar physical fatigue level as indicated by a lack of difference in the mean changes in pre- and post-RPE level between groups. However, the mean changes in pre- and post-heart rate (t = 2.86, P = 0.004) and the mean heart rate measured during game play were significantly higher with larger effect sizes in obese children than normal-weight children (t = 2.84, P = 0.004) due to excess body mass requiring more oxygen delivery to working muscle.
Mean (±Standard Deviation) Values for Physical Activity, Exertion, and Heart Rate During Exergames
d represents Cohen's effect size in obesity versus normal weight.
HR, heart rate; MVPA, moderate-to-vigorous physical activity; RPE, rating of perceived exertion.
Inhibitory control performance at baseline
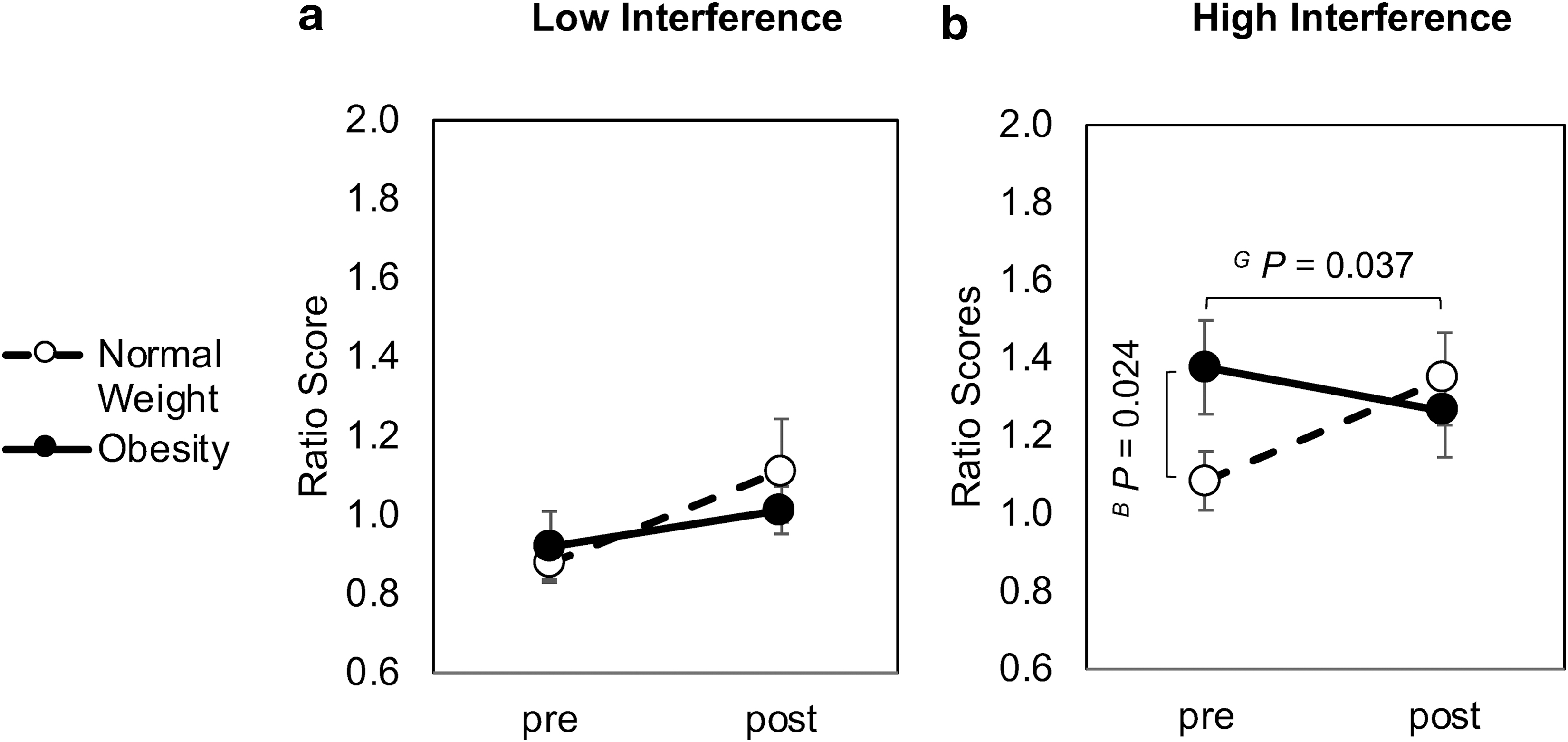
Baseline comparison of VST using t-tests indicated that children with obesity compared with their normal-weight counterparts had significantly longer reaction times in the congruent (t = 2.15, P = 0.019) and incongruent conditions (t = 2.39, P = 0.011) as well as a longer completion time in the incongruent condition (t = 2.74, P = 0.005) (Table 3). We also found a significantly greater ratio score for high interference (incongruent/neutral) in children with obesity relative to their normal-weight peers (1.4 ± 0.5 vs. 1.1 ± 0.3; t = 2.03, P = 0.024) as displayed in Figure 1.
Low
Mean (±Standard Deviation) Values for Cognitive Measures of Inhibitor Control Performance Before and After Exergames
Baseline difference between groups.
Time difference in normal weight or obesity before versus after exergaming.
Group difference in normal weight versus obese.
P < 0.05; **P < 0.01; ***P < 0.001.
CT, completion time; RT, reaction time; SD, standard deviation.
Inhibitory control performance in response to exergaming
Completion time
The omnibus analysis for the VST mean completion time revealed a congruency effect (P < 0.001) with shorter completion time for neutral (P < 0.001) and congruent (P < 0.001) relative to incongruent trials. Furthermore, the analysis for the VST mean completion time revealed a main effect of time (P = 0.005, η 2 = 0.04) that was superseded by a group × time interaction (P = 0.014). Specifically, the t-tests indicated that children with obesity had a significantly shorter VST completion time (seconds) following exergames only during the incongruent trials (−5.1 ± 38.4 vs. 18.14 ± 24.9, P = 0.013), compared with normal-weight children who had a longer VST completion time (P = 0.002) (Table 3). Furthermore, the secondary analysis comparing the interference effect (ratio score) for the VST completion time yielded a significant group × time interaction (F1,38 = 5.99, P = 0.016, η 2 = 0.05), indicating that children with obesity (pre: 1.4 ± 0.5, post: 1.3 ± 0.5) relative to their normal-weight counterparts (pre: 1.1 ± 0.3, post: 1.4 ± 0.5) displayed a significantly lower ratio score in their high interference (incongruent/neutral) (−0.1 ± 0.7 vs. 0.3 ± 0.6, P = 0.037). This result was due to a significant increase in ratio score for normal-weight children (P = 0.025) following exergames. However, we observed a nonsignificant difference in their low interference ratio score (congruent/neutral) (P = 0.215) after exergames (Fig. 1).
Accuracy
The omnibus analysis for the VST accuracy revealed main effects of time (P < 0.001) and congruency (P = 0.001) that were qualified by a group × time interaction (P < 0.001). Even with the reduction in their VST completion times, the t-tests indicated children with obesity made fewer errors (score) than normal-weight children for the congruent condition (1.2 ± 3.5 vs. 4.1 ± 4.9, P = 0.021) and the incongruent condition (1.6 ± 6.0 vs. 6.3 ± 6.9, P = 0.012) after exergames. This was due to a significant increase in errors for the congruent condition (P < 0.001) and the incongruent condition (P < 0.001) following exergames in normal-weight children. (Table 3).
Reaction time
The omnibus analysis for the VST reaction time exhibited main effects of group (P = 0.044) and congruency (P < 0.001) but yielded no further significant interactions. More specifically, the t-tests revealed that children with obesity had a shorter reaction time (millisecond) after exergames only during the incongruent trials (−244.6 ± 275.3 vs. −53.2 ± 393.3, P = 0.041), compared with their normal-weight peers. This was because of a significantly shorter reaction time in children with obesity (P < 0.001), but a nonsignificantly shorter reaction time in normal-weight children (P = 0.723) (Table 3). Additionally, no further significant interactions were observed for the mean completion time, reaction time, accuracy, or interference (Supplementary Table S2).
Discussion
We found that: (1) inhibitory control was inversely related to BMI percentiles, and (2) children with obesity relative to their normal-weight peers gained more cognitive benefits after spending a similar amount of time in moderate-to-vigorous physical activity during a short bout of exergames. Our findings suggest that children with obesity compared with their normal-weight counterparts gained more cognitive benefits from an acute bout of exergames, which might be related to lower executive functioning at baseline in the children with obesity.
The inverse relationship between childhood obesity and executive functioning in different cognitive domains has been indicated in cross-sectional studies with a relatively large sample sizes using BMI33,44 or adiposity. 34 Furthermore, an observational study over ∼100 days also indicated that overweight/obese children had lower executive and academic performance compared with normal-weight children, which was independent of known confounders (e.g., fitness). 37 Consistent with these results, we found that, even given our relatively smaller sample size, children with obesity relative to their normal-weight peers had a higher interference score based on processing speed (longer reaction times and completion times in children with obesity compared with their normal-weight counterparts), which implies greater difficulty in managing interference. This effect was comparable across task conditions, regardless of executive function demands, and occurred independently of health conditions (e.g., physical activity, fitness) known to influence executive functioning, suggesting that childhood obesity itself is related to impairments on a task that modulates inhibitory control. In support of the above findings, neuroimaging studies have observed that children with obesity relative to their normal-weight peers had a reduction in cortical thickness (reflecting increases in cortical myelination 33 ) and a decrease in neuroelectric activity (reflecting an ability to modulate the cognitive control network 35 ) particularly for the prefrontal cortex, 45 which primarily regulates inhibitory control. These effects may also be associated with obesity-induced increase in metabolic abnormalities, which leads to alterations in brain structure and function. 46
Acute bouts of physical exercise are linked to enhanced inhibitory control, which has been observed in multiple studies using traditional modes of exercise 26 and classroom-based physical activity 11 ; however, to our knowledge, no prior studies have investigated the effect of exergames as a school-based physical activity on inhibitory control. The enhancement in inhibitory control reported from the studies above was based on acute exercise-induced decreases in cognitive processing time, which corresponds to our present findings indicating significant reductions in reaction time following exergames, particularly for children with obesity. Empirical evidence suggests that cognitive benefits result from acute exercise-induced physiological changes combined with increases in brain-derived neural factor, 27 neurotransmitters, 47 and cerebral blood flow, 29 which provide support for neural activity underlying changes in cognition. 48 However, as we did not include a non-exergaming control condition, we cannot conclude that the enhanced inhibitory control were purely the results of engagement in the exergames. We instead focused on whether differences in weight status may modulate cognitive performance in response to exergaming.
One of the key findings with respect to our central research question was that children with obesity relative to their normal-weight counterparts reduced VST completion time and made fewer errors after exergaming. Above all, children with obesity had lower interference scores indicating better cognitive processing speed and greater response accuracy in resolving the conflict between competing stimulus and response demands. 49 We speculate that changes in cognitive gains may be larger in those individuals who have relatively lower baseline executive function performance, offering the possibility of greater capability for cognitive enhancement. In support of this speculation, Drollette et al. 36 assessed inhibitory control performance and event-related brain potentials, and found that cognitive benefits from single bouts of exercise were larger in children with lower inhibitory control capacity. Although there is a paucity of data concerning the effect of weight status on the acute exercise/cognition relationship, our findings and those reported in other studies34,35,44 suggest that children with obesity are more likely to have lower inhibitory control and therefore stand to gain more cognitive benefit following acute bouts of exercise.
In terms of a dose/response relationship between exercise and cognition, recent meta-analyses suggest that acute bouts (∼10 minutes) of traditional exercise modes 26 or classroom-based physical activity 11 with more intense activity can facilitate executive function. The current study used a similar duration (9.5 minutes) as well as moderate-to-vigorous intensity (87%) during the exergames for both groups. As our exergames induced a similar dose of physical activity (i.e., step counts, moderate- or vigorous-intensity) and game play duration across groups, children's weight status might be a moderating factor that differentially affects acute cognitive gains. Additionally, mean heart rate (lower in normal-weight children than their counterparts with obesity) indicates that exergaming might not be physically exerting enough for normal-weight children or might be more physically exerting for children with obesity to gain cognitive benefits. However, Hwang et al. 22 recently compared weight-dependent effects and observed that relatively higher heart rate in children with overweight/obesity might relate to their excessive body mass, which demands more energy expenditure to meet muscle work requirements during a similar intensity and duration of exergames. Above all, the mean heart rate during exergames for all groups were within a range of ≥64% and ≤76% of their maximum heart rate, which is a conventional cut-point for the moderate-intensity heart rate zone. 50 Thus, cognitive gains based on group differences in mean heart rate might not be meaningfully different, especially when all mean heart rate values fell within a certain range of exercise intensity. 24 However, we cannot rule out the possibility that such significant difference in heart rate between groups may differentially affect cognitive performance. Furthermore, the exergames feature intermittent activity and shorter session duration, which may have induced less fatigue and/or boredom, and thereby may have positively impacted the ability and motivation to perform exercise. 22
We should note several important limitations to our study. First, we used a convenience sample that may not be representative of our target population. Second, multilevel statistical models may be needed to properly analyze group differences because of the different school classes included in the present study; however, the analyses were not performed due to our small sample size. Third, as previously mentioned, without a control condition, we cannot rule out the possibility that the enhanced inhibitory control resulted from other factors rather than the acute exergaming effect. Fourth, we did not assess aerobic fitness, which is a known moderator of the acute exercise/cognition relationship. 48 Lastly, exercise intensity and duration might not have been exactly the same between both groups during game play, and these factors may differentially affect cognitive performance. Future studies using the same exercise duration and intensity (based on maximal heart rate or maximal oxygen consumption) are needed to examine the weight-dependent effects of exergaming on executive functions.
Conclusion
We demonstrated that childhood obesity was inversely associated with inhibitory control performance. However, acute cognitive effects of exergames were greater in children with obesity compared with their normal-weight peers. Our results suggest that children with obesity who demonstrate a relatively lower cognitive capacity may derive more cognitive benefits from exergames. Moreover, regardless of weight status, both normal-weight children and children with obesity similarly spent the majority of their exergame time at a moderate-to vigorous-intensity activity. Exergames serve as a promising tool to increase physical activity behaviors and may enhance cognitive health in a manner that can be applied between periods of academic instruction, during recess, or after school hours. Future studies investigating the short- and long-term effects of exergames on executive function are warranted.
Footnotes
Acknowledgments
The authors would like to thank the children for their participation in this study. The authors would also like to thank Mie Hashimoto, MPH; Carlos Andres Hoyos Cespedes, MPH; Miranda Prasad, MS; and Samantha Gutiérrez-Arango, BS, for their help with data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported in part by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases (R01DK109316), PI: A.S.L.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.