
Abstract
Objective:
Mild cognitive impairment (MCI) is a broad term for people at a stage between normal age-related cognitive decline and dementia, where cognitive problems are present but do not impair activities of daily living. This study aimed at evaluating the effectiveness of a virtual reality (VR)-based rehabilitation program on cognitive functions in MCI.
Materials and Methods:
Sixty-one older adults (25 men, 36 women) with MCI were randomized to the intervention group (n = 30; 70.12 ± 2.57 years) or control (n = 31; 70.30 ± 2.73 years) group. The intervention group received a VR (computer-generated interactive environments) intervention in addition to a conventional cognitive rehabilitation (CR) intervention, whereas the control group received only the CR intervention. Cognitive functions were assessed in both groups before and after the 12-week interventions by using the Loewenstein Occupational Therapy Cognitive Assessment-Geriatric.
Results:
Between-group comparisons revealed significantly greater improvements in orientation, visual-spatial perception, visuomotor organization, thinking operation, and attention/concentration functions in the VR group than in the control group (P < 0.001 for all).
Conclusion:
Our results showed that 12 weeks of VR-based rehabilitation enhanced cognitive functions in older adults with MCI. Using VR applications in CR is recommended to improve cognitive functions of older adults with MCI.
Introduction
The older people are growing worldwide, leading to increases in the incidence of chronic diseases such as neurological, orthopedic, psychiatric, and cognitive impairments. 1 Recent studies have shown that cognitive functions are significantly affected in middle age and early old age. 2 Mild cognitive impairment (MCI), also referred to as the pre-dementia stage, is one of the most common cognitive dysfunctions seen in the elderly population. 3 It is also a predictor of numerous types of dementia. It was reported that 10%–15% of older adults with MCI develop dementia every year. 4 The prevention of MCI and dementia is very important. Therefore, it is necessary to develop rehabilitation approaches for these disorders in the elderly population and to apply them, especially in the early period, to protect and maintain independence in activities of daily living. 5
Various rehabilitation approaches for cognitive dysfunction in older people with MCI have been described in the literature, including focused restorative cognitive training, focused compensatory cognitive training, comprehensive interventions that focus either on memory alone or on multiple domains, focused lifestyle interventions, and focused activity-based interventions. 6 In addition to these approaches, recent technological advances have enabled the use of interactive and immersive virtual reality (VR) applications in cognitive rehabilitation (CR). 7
Introduced in the 1980s, VR is a simulation system in which a sense of reality is created with a multisensory (visual, vestibular, etc.) effect via a human-machine interface system.8,9 Because motivation can wane in conventional rehabilitation interventions, VR-based rehabilitation approaches may increase patients' active participation and motivation during the treatment process. 7 VR technology also offers therapists and researchers benefits in terms of evaluation and research. 10 In addition, the simulated environment of VR avoids adverse events that may occur in the real environment, such as falls and injury. 11 Thus, Larson et al. 12 stated that using VR in CR processes is more effective than conventional evaluation and interventions. A recent review evaluating VR-based interventions emphasized the need for further studies on the impact of these interventions on cognitive functions. 7 Therefore, the aim of this current study was to examine the effect of VR-based CR on the cognitive functions of older adults with MCI.
Materials and Methods
This single-blinded, randomized controlled study investigated changes in the cognitive functions of older adults with MCI after CR interventions with and without a VR component. The protocol used in this study was approved by the University Ethics Boards and Commissions (permission number: GO19/406). Written informed consent was obtained from all participants before the study.
Participants
Sixty-six older adults who presented to the occupational therapy department of a public university between 2019 and 2020 were screened. Inclusion criteria were: (1) age between 65 and 75 years; (2) MCI diagnosis; and (3) ability to understand and follow verbal instructions. Exclusion criteria were: (1) secondary chronic disease that may affect cognitive functioning; (2) auditory and visual problems that may affect rehabilitation implementation and communication; and (3) attending any rehabilitation program (physiotherapy, speech therapy, psychotherapy, etc.) during the study period. Based on the inclusion and exclusion criteria, two subjects were excluded due to participation in another rehabilitation program. The remaining 64 participants were randomized to either the CR group (control) or the CR+VR group by using a computer-generated randomization technique. The allocation process was carried out by the third author of this study (S.P.). Two participants from the CR+VR group and one participant from the control group were excluded from the study, because they could not adhere to the frequency of the study intervention. Therefore, the study was completed with a sample of 61 older adults (Fig. 1).
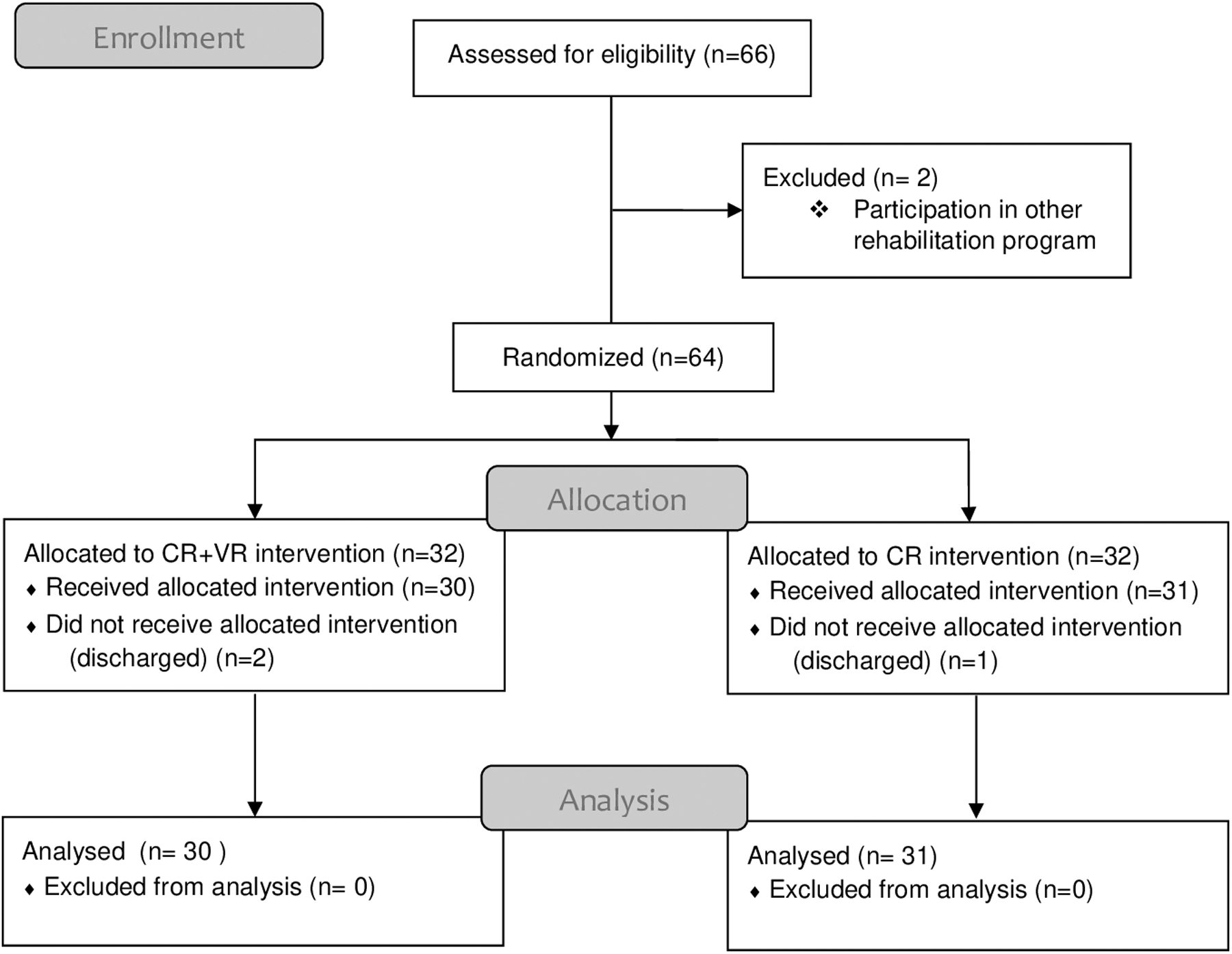
CONSORT diagram.
Measurement
Demographic information of the participants was collected, including their age, sex, education level, and marital status. All participants underwent cognitive function assessment by using the Loewenstein Occupational Therapy Cognitive Assessment-Geriatric (LOTCA-G) twice, once before the intervention and again after the 12-week intervention. These evaluations were done by the second author (S.Ş.), who was blinded to the group allocation process and did not know that VR intervention was performed in the study.
The LOTCA-G
The LOTCA-G is a cognitive assessment tool adapted for the older population. 13 This 24-item test is widely used by occupational therapists and evaluates 8 cognitive areas: orientation, visual perception, spatial perception, motor praxis, visuomotor organization, thinking operation, memory, and attention/concentration. Items in each subtest are assessed on an ordinal scale from 1 to 4 except for the orientation items, which are evaluated from 1 to 8. A higher score indicates better cognitive performance. The LOTCA-G discriminates between healthy older adults and those with dementia and MCI. It is sensitive to levels of dementia and identifies changes over time. 14
Interventions
The recommended duration for VR and CR interventions is 10–12 weeks, administered two or three times a week.6,7,15 According to this information, we planned both interventions in this study to be performed in 45-minute sessions twice a week for 12 weeks. Both the CR and VR programs were carried out by the first author of the study (B.T.).
CR intervention
Based on the eight cognitive subtests in the LOTCA-G, the authors designed a CR intervention procedure consisting of two parts.
Week 1–8: Each of the first 8 weeks featured interventions for one of the cognitive domains of the LOTCA-G (attention/concentration, memory, orientation, visual perception, spatial perception, visuomotor organization, praxis, and thinking operation).
Week 9–12: The last 4 weeks of the CR program included interventions involving all of the cognitive functions.
VR intervention
The Microsoft Kinect for PC program without immersion was used in the VR-based intervention. Kinect has a system that detects the 3D movements of the participants. The interventions were carried out in a 20-m2 room with the participants 1.5 m from the viewer (65-inch flat-screen LED screen television). During VR activities, the floors were padded to prevent injuries as the participants were standing.
The intervention involved four different games that can be played with Kinect and purchased commercially in the online system. First, all authors except the second author independently observed each game to determine what cognitive functions were required to execute the games successfully. After this evaluation, meetings were held to discuss and reach a consensus regarding these requirements. The cognitive function requirements of the four games were determined as follows:
Boxing Trainer is a game in which the player that controls two boxing gloves punches pads at different sides of the screen and requires orientation, attention/concentration, visual-spatial perception, reaction time, visuomotor organization, visual and spatial perception, and cognitive time management (racing against time). Jet Run is a racing game in which the player's avatar is controlled by jumping and body movements. The game requires attention/concentration, visual-spatial perception, visuomotor organization, reaction time, and orientation. Superkick is a penalty shootout game that requires orientation, attention/concentration, visual-spatial perception, visuomotor organization, contralateral perception, cognitive time management (racing against time), and reaction time. Air Challenge is a skydiving game in which the player passes through checkpoints and circles. The player controls the game in which the avatar moves in the opposite direction with body and shoulder movements (participant moves his arm to the right, the avatar goes to the left, etc.). In addition to the similar requirements listed for the other games, this game also requires mirroring.
As all the games involved similar cognitive function requirements, they were all offered to the participants to encourage motivation and participation.
Statistical analysis
Data were analyzed with SPSS version 22.0 statistical software package program. Data are presented as mean ± standard deviation. Normality of the data was analyzed by using Kolmogorov–Smirnov test. Differences between groups were analyzed with chi-square test for nominal data. Comparisons between the groups were conducted by using Mann–Whitney U test. Pre- to post-intervention changes within the groups were analyzed with Wilcoxon signed-rank test. Significance was evaluated at levels of 0.05. Effect size was calculated by using the means and standard deviations of the groups. Effect size benchmarks were determined as <0.30, 0.30–0.80, and >0.80 and considered small, moderate, and strong, respectively. 16
Results
Mean ages of the CR group (n = 31) and CR+VR group (n = 30) were 70.30 ± 2.73 years (range 5–7 years) and 70.12 ± 2.57 years (range 66–74 years), respectively (P > 0.05). Table 1 shows the other demographic characteristics of the study groups. There were no significant differences between the groups in terms of sex and education level (P > 0.05) (Table 1).
Demographic Characteristics of the Groups
CR, cognitive rehabilitation; VR, virtual reality.
Pre-intervention LOTCA-G scores did not differ significantly between the study groups (P > 0.05) (Table 2). Within-group analysis showed a significant increase in all functions (P < 0.001) in except praxis and memory in the study group (P < 0.05), and in the control group (P < 0.05). Between-group analysis showed a significant increase in orientation, visual-spatial perception, visuomotor organization, thinking operation, and attention/concentration in the study group. Although participants in both groups showed an increase in LOTCA-G total score, between-group analysis showed that there was significantly more improvement in the CR+VR group compared with the control group (P < 0.001). Comparisons of the changes over time for cognitive functions within and between groups, as well as effect sizes, are shown in Table 3. Comparing the groups, strong effect sizes in all cognitive areas in the LOTCA-G are shown in the study group.
Comparing Pre-intervention LOTCA-G Scores Between Groups
LOTCA-G, Loewenstein Occupational Therapy Cognitive Assessment-Geriatric; SD, standard deviation.
Comparing Cognitive Group's and Cognitive-Virtual Reality Group's Pre-intervention and Post-intervention LOTCA-G Results
P < 0.05, **P < 0.01.
P < 0.05 within-group differences.
Effect size >0.80.
Discussion
This study examined the effect of VR-based rehabilitation on cognitive functions in older adults with MCI. According to the results of our study, 12-week CR and CR+VR interventions had positive effects on cognitive functions, but the CR+VR group showed greater improvement in the areas of visual-spatial perception, visuomotor organization, orientation, thinking operation, and attention/concentration than the CR group.
Orientation involves multidimensional cognitive functions and is the first affected in diseases such as MCI and dementia. 17 Kim et al. 18 reported that orientation deteriorated with increasing age in the elderly population. Hofmann et al. 19 showed that orientation skills were impaired in older adults with Alzheimer's disease and MCI and that 12 sessions of VR-based applications (involving the real local and social environments of the participants and applied with the interface system) resulted in greater improvement in orientation compared with the control group. Similar to this study, we found that the CR+VR group showed more improvement in orientation skills than the CR group. A possible explanation for this result is that VR settings may elicit orientation functions more than the normal environment for older adults.
In a study investigating visual processing skills in MCI, Krajcovicova et al. 20 detected impairments in the visual-spatial perception and visuomotor task pathways, which they interpreted as supporting the view that MCI is a transition stage before Alzheimer's disease. They also emphasized that these connection changes are task specific; that is, they are located in the regions that were activated during the execution of a visual task. Haque et al. 21 stated that visual-spatial perception and visuomotor functions are worse in older adults with MCI compared with their healthy peers, and likewise stated that many areas in the brain actively work together for these functions. In their mini-review, D'Cunha et al. 7 emphasized that VR-based interventions have positive effects on cognitive functions. They stated that VR applications actively engage visual functions due to the intensity of the simulation and have an immersive effect. In this study, the CR+VR group showed better performance in visual-spatial perception and visuomotor functions after the intervention. This may be a result of the intense visual stimuli in VR applications and the integration of visual and motor functions in the VR setting.
Apraxia is caused not only by poor motor execution skills but also by the loss of information about the correct use of objects.22–25 Shaver 26 showed that praxis skills gradually deteriorated in individuals aged 65 and older and demonstrated the necessity of well-designed and effective rehabilitation programs for the protection of praxis. The researcher also noted that praxis skills have varying activations in the frontal, premotor, and parietal cortex, suggesting that it would be beneficial to create more personalized and effective rehabilitation programs. 26 Although an increment in motor praxis skills was observed in both groups in our study, the CR group showed more improvement in praxis compared with the CR+VR group. The reason for this may be that the VR setting used in our study did not include motor imitation, utilization of objects, or symbolic action sections, which are under motor praxis. We believe that VR scenarios that include these sections should be developed for use in rehabilitation interventions.
Petersen 3 reported that one of the first cognitive components they looked at when diagnosing elderly people with MCI was memory and that most elderly individuals' complaints consisted of forgetfulness, confusing names, and forgetting their address. The researchers showed the importance of implementing VR-based CR intervention approaches for improving memory in people with MCI.27,28 Contrary to these results, our findings did not support the superiority of VR-based CR over standard CR techniques. Again, this may be attributed to the VR scenarios used in this study, which did not include memory-related parameters. In contrast, the VR-based interventions mentioned earlier involved scenarios focused on memory.27,28 Therefore, we think that in VR-based interventions, adapting the presented scenarios according to the affected cognitive function of the participant will provide a greater therapeutic effect.
Andersen defined the executive function areas as attention control, cognitive flexibility, goal setting, and information processing. 29 The thinking operation domain of the LOTCA-G evaluates this executive function. Anderson-Hanley et al. showed that cognitive training on a tablet while cycling on a stationary bike (Neuro-exergaming) supports executive function. 30 Similarly, we observed better performance in this area in our CR+VR group. The VR setting that we implemented included ranking, categorizing, planning, attention/concentration, maintaining and completing the game, visual-spatial perception, and visuomotor skills. This may explain the greater improvement in the CR+VR group compared with the CR group.
The LOTCA-G also has an attention/concentration section. Petersen 3 reported that cognitive functions such as executive attention/concentration, visual-spatial perception, and executive function are frequently affected in older adults with MCI. Manera et al. 31 showed that attention/concentration areas were affected in these patients, and there was more improvement in the attention/concentration skill in the VR group with randomized controlled immerse cognitive training. In our study, there was an increase in attention/concentration scores in both groups, but the CR+VR group improved more compared with the CR group. We believe that this difference occurred, because the games in our VR-based intervention focused heavily on attention and concentration. We are of the opinion that games that enhance attention/concentration functions can be used to effectively promote cognitive functions in older adults.
There are several limitations to this study that deserve comment. First, although the cognitive test we used included many cognitive parameters, the lack of cut-off value required us to interpret the participants' cognitive function levels. The second limitation is that the VR setting is standard and could not be graded for the individual subjects. We recommend further studies to compare games with different challenge levels and scenarios. Despite these limitations, older adults with MCI who completed 12 weeks of VR-based CR showed greater improvement in orientation, visual perception, spatial perception, visuomotor skills, thinking operation, and attention/concentration scores when compared with the non-VR CR group. The VR-based rehabilitation approach provides support for CR interventions in older adults with MCI, and it is appropriate for research and clinical interventions targeting cognitive functions in this population.
Footnotes
Ethical Approval
Ethical approval was obtained from Health Sciences University (Ref: Go 19/406).
Author Disclosure Statement
The results of the study are presented honestly, clearly, and without falsification, fabrication, or inappropriate data manipulation. The authors have declared no conflicts of interest.
Funding Information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.