
Abstract
Videogames have been applied to improve health-related outcomes in people with intellectual disabilities (ID). For this purpose, it seems necessary to make available the best scientific information concerning the feasibility and potential benefits of playing videogames within this population. This study aimed to systematically review the existing scientific evidence regarding the effects of videogaming on the physical and mental health of people with ID. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, a literature search was performed using MEDLINE/PubMed, PEDro, SPORTDiscus, and Scopus up to June 2020. The Physiotherapy Evidence Database (PEDro) scale was used to rate the methodological quality of the included investigations. A total of 17 randomized controlled trials (RCTs) were selected. Data synthesis examined physical health, including anthropometrics, physical fitness, and motor skills, and mental health and cognitive function. Intervention protocols were based on videogames of different nature (i.e., exergames and computerized cognitive training) and showed substantial heterogeneity in duration. Session length varied from 15 to 60 minutes. Five studies achieved a high intervention adherence rate, whereas a low drop-out rate was reported in eight RCTs. Videogaming is a useful therapy for improving physical and cognitive function in people with ID. Exergaming seems to be an interesting physical intervention for increasing fitness and motor skill levels, while sedentary videogaming has shown potential for stimulating cognitive function. Further research to analyze its feasibility and its impact on body composition and mental health is needed.
Introduction
Intellectual disability (ID) is a condition characterized by significant limitations in both intellectual functioning and adaptive behavior as expressed in conceptual, social, and practical skills. These series of limitations originate before brain maturation. 1 Prevalence rates for ID have varied from 3.31 to 36.75 per 1000; giving a pooled prevalence rate of 9.2 per 1000. 2 The global prevalence has been suggested to be below 1%, with rates ranging from 0.22% to 1.55% in children/adolescents and from 0.05% to 0.8% in adults. 3
People with ID show an inactive lifestyle that puts them at a higher risk of developing health problems. 4 Therefore, preventive measures are needed to reverse their sedentary behavior. In this regard, the promotion of physical exercise appears to be an accurate strategy for improving both physical 5 and mental health 6 in this population. Nevertheless, such action seems difficult to put into practice, given that those with ID generally exhibit low exercise participation rates. 7 To rectify this situation, facilitators and barriers to exercise should be first identified.
According to the existent literature, the primary barriers to exercise reported by people with ID are transportation issues, financial limitations, and lack of awareness of options, motivation, and time.8,9 Exercise facilitators commonly reported in this population are ability, positive experience, accessibility, family/friends to be active with, and support to participate in fitness activities.9,10 In this vein, alternative exercise interventions, such as dancing, 11 aquatics, 12 or martial arts, 13 have appeared to be feasible and enjoyable. However, people with ID might not be able to access exercise facilities to perform these activities.
In this sense, videogaming could also be an interesting option for overcoming the aforementioned barriers since it constitutes a low-cost and attractive leisure activity that can be practiced at home at practically any time. 14 Besides, some videogame modalities do not require high skill levels and can be played with family and friends. Hence, playing videogames, particularly the type that demands the performance of physical activity (commonly known as “active games” or “exergames”), might be considered as an exercise modality that could generate greater acceptance and foster higher levels of adherence, which are both key elements for the effective promotion of exercise among those with ID. 11
Exergames are gaming applications capable of improving users' physical health. 15 For instance, their practice can help to reduce the prevalence of obesity and enhance aerobic fitness. 16 This is an important point to consider since the high prevalence of obesity and the low level of aerobic fitness that are usually present in individuals with ID constitutes a threat to their health.17,18 Similarly, exergaming has shown to be effective at improving motor skills. 19 Motor skills potentiate functional independence in people with ID, and the need for further research focused on therapies aimed to stimulate them has been highlighted. 20
It should also be noted that exergames are not very physically demanding and are played in a safe and familiar environment. Thus, its practice can help to overcome several exercise barriers related to the health status of this population (i.e., fear of falling, overweight, heart condition) and to different environmental factors (i.e., lack of acceptance, negative societal influences, and weather constraints). 21
Exergames can also be a promising physical exercise strategy to improve mental health. Individuals with ID face a great prevalence of mental disorders, including challenging behavior, anxiety, or depression. 22 Scientific evidence has revealed that exergames can positively affect on psychological and emotional health, through increments on tryptophan levels, a precursor of cerebral serotonin that regulates behavior, mood, and anxiety. 23 Exergames may also help reduce depression levels since their practice promotes distraction from routine and reduces loneliness and social isolation. 24
Finally, exergames are considered as valuable resources for stimulating cognitive function. This is an important fact to consider given that people with ID manifest a high risk of developing cognitive deficits, 25 which are core features of mental health conditions. For instance, neuropathological changes of Alzheimer's disease are present in the brains of persons with Down syndrome (DS), and prevalence rates for dementia have been documented to be as high as 50%–75% in this population. 26 Likewise, the overall prevalence of dementia among those with ID is considerably higher than that observed in the general population, achieving rates up to 70%. 27
In this aspect, exergames propose the performance of dual tasks, which stimulate the brain to generate cognitive and motor responses simultaneously, requiring cortical and subcortical circuitry activation. As a result, improvements in parameters related to cognitive impairment of older adults, namely semantic memory, executive function, and short-term memory, can be expected, which led to thinking that such therapy might prevent the risk factors for dementia. 28
Other videogame modalities can be of interest to people with ID. For example, sedentary videogames (i.e., “Super Mario,” “Space Fortress”) have demonstrated beneficial effects on the cognitive function of healthy populations. 29 Similarly, some authors have proposed computer-based cognitive training, based on playing user-friendly videogames, as a strategy for preserving cognitive functioning in adults at risk for cognitive decline. 30 This kind of therapy has also proved to be helpful in treating depression. 31
In light of all these, videogaming appears to be a promising therapy for individuals with ID, and thus, its practice could be prescribed to them. For this purpose, it seems necessary to make available the best scientific information concerning the feasibility and potential benefits of playing videogames within this population. This goal can be accomplished by performing systematic reviews that collectively summarize scientific evidence on the topic. However, no systematic review on this subject has been published to the authors' knowledge so far. To provide the highest level of scientific evidence, this kind of research should be based on the inclusion and detailed analysis of the randomized controlled trials (RCTs) that have been conducted on the topic. 32
Under these circumstances, the purpose of the present work is to conduct a systematic review of the methodological quality and main results of the RCTs published to date that aimed at analyzing the effects of videogaming interventions on the physical, mental health, and cognitive function of people with ID.
Methods
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 33
Search strategy
An extensive literature search for RCTs related to the topic of videogaming and ID was conducted using four electronic databases: MEDLINE/PubMed (January 1945–June 2020), Scopus (October 1964–June 2020) SPORTDiscus (January 1970–June 2020), and Dialnet Plus (November 1984–June 2020). The following search terms, Boolean operators, and combinations were used: “Videogames” OR “Exergames” AND “Intellectual Disability.” The search was focused on titles and abstracts of peer-reviewed journal articles since abstracts, proceedings, book chapters, or theses were not included as they could not be searched systematically in databases. 34
Eligibility criteria
RCTs that provided information regarding the effects of playing videogames on children/adolescents and adults with ID were considered eligible. Investigations were excluded if: (a) videogaming was performed in combination with other therapies; (b) the study did not provide data on the effects of playing videogames on physical, mental health, or cognitive function outcomes; (c) the intervention was based on the performance of a single videogaming session; (d) the research was not written in English, Portuguese, or Spanish language.
Study selection
Two authors screened the titles and abstracts of the identified articles for eligibility. After independently reviewing the selected studies for inclusion, the kappa's Cohen statistic was calculated to achieve agreement between reviewers. Once the agreement had been reached, a full-text copy of every potentially relevant article was obtained and revised by both authors. If it was unclear whether the investigation met the selection criteria, advice was sought from a third author, and a consensus on opinion was achieved. Moreover, the full texts of the reports that met the inclusion criteria were manually screened for any additional relevant references.
Data extraction
Information on study design, participants' characteristics, intervention details, drop-outs, and outcomes were extracted from the original reports by one researcher and checked by a second investigator. For this purpose, we designed a data extraction form together with coding instructions for data collection following previous procedures. 5 Contacting author details of eligible primary studies were also registered if necessary, to ask for missing data or obtain additional information on poorly reported items. 35
Quality appraisal
For assessing the methodological quality of the selected investigations, ratings were extracted from the Physiotherapy Evidence Database (PEDro). 36 Studies not included in PEDro were rated by one author. In the case of doubt, advice was sought from a second author. The PEDro scale has 11 items corresponding to 11 quality criteria. Each item awards one point when it is satisfied. The first item is not included to calculate the PEDro score; therefore, scores range from 0 to 10, with higher scores indicating a better methodological quality of the study. The suggested cut points to categorize studies by quality were excellent (9–10), good (6–8), fair (4–5), and poor (<3). 37
Results
Studies' selection
The independent reviewers agreed on 82/88 of the titles and abstracts initially found (93%). The interrater agreement (kappa) was 0.77. From the retrieved articles, 17 RCTs were included in this systematic review (Fig. 1).38–54 The main characteristics of the included articles are summarized in Table 1.
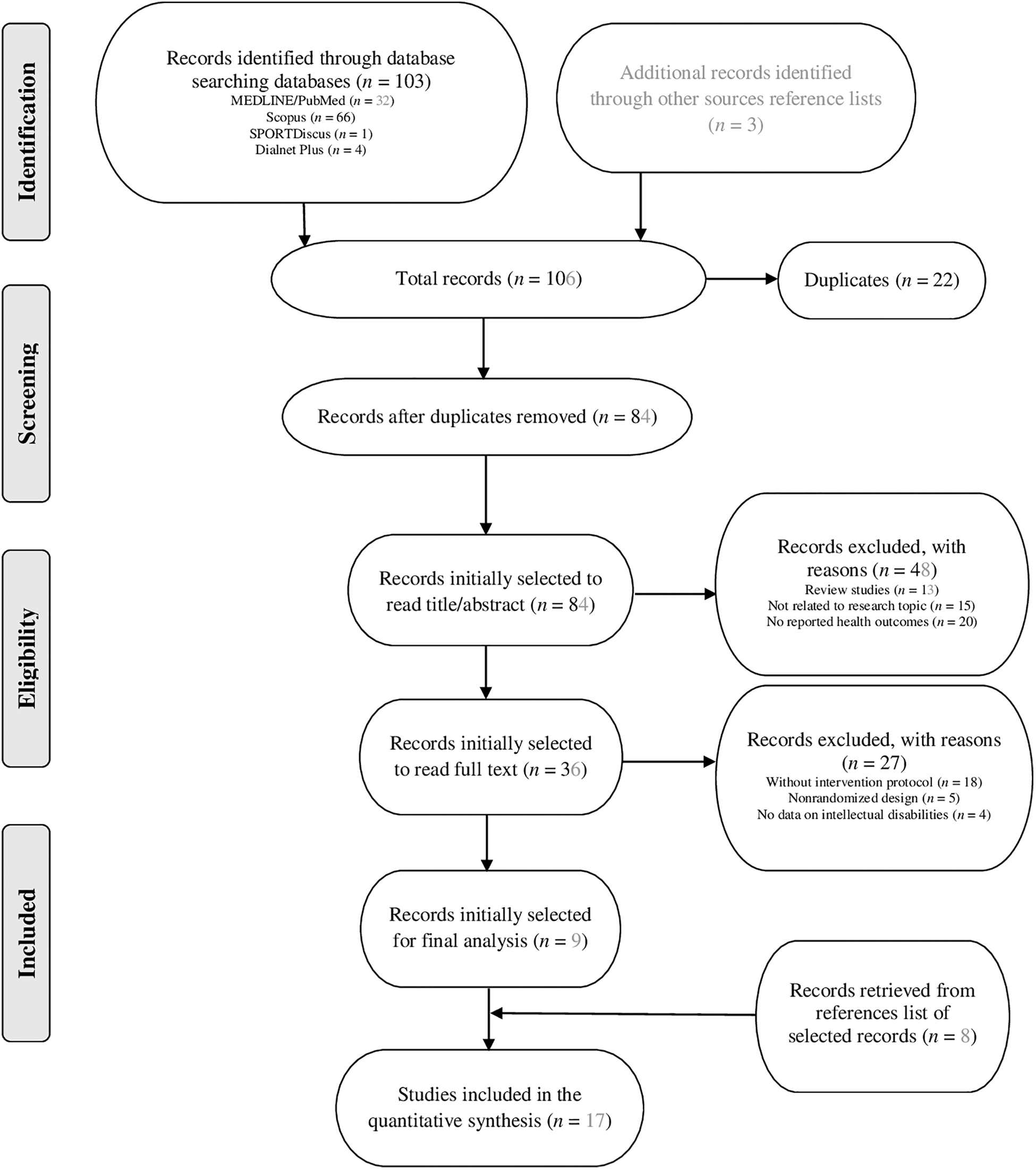
PRISMA flow diagram of articles included in the systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Summary of the Randomized Controlled Trials Included in the Systematic Review
P < 0.05; **P < 0.01.
ADHD, attention-deficit/hyperactivity disorder; BMI, body mass index; BOT-2, Bruininks–Oseretsky Test of Motor Proficiency-seconded.; %BF, body fat percentage; CG, control group; DS, Down syndrome; EG, experimental group; F, female; IQ, intelligence quotient; ID, intellectual disability; KBIT-II, Kaufman Brief Intelligence test; M, male; NR, not reported; SD, standard deviation; STM, short-term memory; WC, waist circumference; WM, working memory.
Methodological quality and risk of bias
The methodological quality of the RCTs was good (6–8 points) in eight studies28,41–43,45,47–49 and fair (4–5 points) in the remaining nine.39,40,44,46,50–54 The median score in the PEDro scale was 5 (Table 2).
Quality Assessment of Randomized Controlled Trials
Eligibility criteria item does not contribute to total score. Items: (1) eligibility criteria; (2) randomization; (3) concealed allocation; (4) similarity at baseline; (5) subjects blinding; (6) therapists blinding; (7) assessors blinding; (8) one key outcome measured in >85% of subjects; (9) intention-to-treat analysis; (10) between-group statistical results for one key outcome; (11) measures of variability and point measures for one key outcome.
All reviewed trials clearly described and adequately completed the randomization process and these also provided both point measures, and measures of variability for at least one key outcome. Four PEDro scale items (eligibility criteria, similarity at baseline, a key outcome measured in >85% of subjects and between-group statistical results for one key outcome) were achieved in majority of studies (14 out of 17). Six out of 17 investigations incorporated assessors blinding.38,41,42,47,48,50 Besides, participants were blinded in four trials,40,41,45,48 where the control group received a placebo activity, whereas allocation concealment was reported in another four RCTs.38,41,42,48 An intention-to-treat analysis was used in three studies.43,49,53 Finally, only one research attempted therapist blinding. 41
Participants' characteristics
Across the 17 studies, 1022 participants were involved. The sample sizes of the RCTs were generally small and varied considerably, ranging from 12 to 203 participants (median, 44; first quartile, 25.5; third quartile, 77.5); however, 4 investigations39,42,45,47 accounted for ∼54% of the overall sample size.
Among the included studies, most individuals were males, and the proportion of females ranged between 21.0% 39 and 61.2%, 49 in the 13 trials that reported this information; yet 1 research involved solely male participants. 54 No data were available about the proportion of male or female participants in 3 of the 17 articles reviewed.38,47,53 Nine of the studies in this review included children and/or adolescents ranging from 5 to 18 years,39,41,42,44–47,52,53 whereas seven trials targeted adults of varied ages (18–69 years).38,40,43,48–51 Only one RCT did not provide information on the age of the participants. 54
Eight studies reported the degree of ID, which was classified as mild (n = 2),42,53 mild to borderline (n = 2),44,45 mild to moderate (n = 2),49,52 moderate (n = 1), 51 moderate to severe (n = 1), 39 and severe (n = 1). 50 One RCT considered participants as educable mentally retarded. 54 However, information on the severity of ID of the study's participants was not available in seven investigations.38,40,41,43,46–48
Descriptions of ID etiology were found in eight trials.38,39,41,42,46,47,49,52 Among 6 of these articles, in total, 250 participants were diagnosed with DS. Specifically, Abdel Rahman, 52 Bennett et al., 46 Silva et al., 38 and Wuang et al. 47 included individuals with DS exclusively, with the latter also excluding participants with a coexisting diagnosis of autism. Moreover, 15 participants from the sample of 49 of Cooney et al. 49 presented with DS, as well as 2 individuals from the sample of 41 of Söderqvist et al. 41
In particular, participants with additional diagnosis such as attention-deficit/hyperactivity disorder (n = 9), epilepsy (n = 2), or neurological disorders (n = 7) were involved in the study by Söderqvist et al. 41 Only one investigation included solely participants with autism (n = 100), 39 whereas 104 individuals recruited by Wing-Chung et al. 42 also had comorbidity with autism. Notably, three RCTs stated that those diagnosed with autism were excluded.41,45,47 Eventually, eight trials had no information on the etiology of the ID of the participants they studied.40,43,44,48,50,51,53,54
Intervention characteristics
The interventions showed substantial heterogeneity in duration, ranging from 5 weeks 40 to 1 academic year. 39 Most of them were implemented in 2–3 days/week,38–40,42,43,45–48,50–53 but one study was implemented once a week. 49 One investigation did not detail the frequency. 54 Session length varied from 645 to 60 minutes.38,47,49
The activities carried out during the interventions were videogames of different nature. Nine RCTs included commercial gaming systems where participants practiced physical exercise while playing.38,39,42,43,47,50–53 On the one hand, Lotan et al. 51 used Sony's PlayStation® 2 EyeToy® video capture virtual reality (VR) system and selected different games, including cleaning dirty windows, sports events, or defeating enemies; on the other hand, Lotan et al. 50 provided game-like exercises (i.e., catching balls) using the GestureTek IREX video capture VR system. One additional study 42 used Microsoft Xbox® 360 Kinect to play team-based and individual sport games.
Nonetheless, up to six trials were based on implementing VR training through the Nintendo® Wii™ gaming system.38,39,43,47,52,53 Notably, the balance board of the Nintendo Wii was employed in four investigations.38,43,52,53 The interventions used several types of games, from sports-related and dancing games38,39,43,47 to balance board mini-games that comprised static and dynamic balance activities38,43,52,53 or aerobics.38,43
Correspondingly, the approaches of the other reviewed studies involved intense, repeated practice, specifically on cognitive training tasks based on a computer game environment.40,41,44–46,48,49,54 The delivered interventions included a computerized adaptive training targeting the visual decision-making process, 40 the nonverbal reasoning, 41 the executive functions and math skills, 44 the working memory,41,45 the visuospatial memory, 46 and the cognitive function. 48 Furthermore, Cooney et al. 49 applied a cognitive-behavioral therapy computer game to treat anxiety and depression. Lastly, Rezaiyan et al. 54 implemented a pathfinding computer game to increase attention capacity.
Most computerized training programs provided a game designed to adapt to an individual's current ability level. The game typically spread over a range of difficulty levels.48,49,54 The content of the activities tended to reflect everyday situations with familiar people, animals, plants, or objects,40,41,44–46,49 including animated characters, pictures, texts, or sounds.41,48 Various colors, shapes, sizes, or speeds of appearance were used to distinguish among these kinds of stimuli.40,41,45 Some detailed graphic and verbal feedback were provided during and after each training task. 48 Once the participants completed different in-game tasks or the training, they could receive a virtual or physical reward for their achievement.44–46
Frontline and support staff included in the interventions had a role of supervision to observe and direct participants during the game,39,41,43,48–51,54 and gave physical or technical assistance and words of encouragement.40,42,46–48,50 One article further established that the staff did not help participants when they played the active videogames. 42 The staff were teachers,39,41–43,46 social work, psychology or gerontology students, 48 two occupational therapy students supervised by a physiotherapist, 51 six caregivers supervised by a physiotherapist, as well as an occupational therapist that provided technical support, 50 physical therapists, 52 pediatric occupational therapists, 47 a clinical psychologist, 49 the researchers,40,54 and parents. 41 In contrast, three RCTs38,45,53 did not provide information in this regard.
All exergaming interventions (n = 9),38,39,42,43,47,50–53 as well as three studies46,49,54 using computerized cognitive training programs, were compared with nonintervention control groups (i.e., usual daily activities, standard education, and treatment as usual). In two trials,40,41 participants in the control group were on placebo (i.e., played a similar game). Likewise, in one RCT, 45 the difficulty of the game of the experimental group was adjusted accordingly for the participants assigned to either a second training condition or a control group. In another research, 48 the first control group underwent a computer games program designed to act as a placebo, whereas the second control group was a wait list group. Also, a wait list control design was followed by Jansen et al. 44
Intervention adherence and drop-out
Five studies41,43,44,46,48 described the adherence rate to the videogame intervention. In general, these trials registered high adherence rates to the interventions, as more than 90% of the total sessions were attended by participants.43,46 One intervention 44 had lower adherence rates, and the analysis was performed after splitting the experimental group into high- and low-practice groups. Van der Molen et al. 45 explained that the experimenters checked data from computers for training compliance, but the subsequent analysis was not detailed.
Drop-out rates were reported in eight RCTs.38,41,43,45–49 The minimum rate was obtained by Perrot et al. 43 as none of their participants dropped out. At the opposite end, Söderqvist et al. 41 had the highest drop-out percentage, namely 22.2%, where only 41 of the 52 participants allocated to experimental or control groups were included in the final analysis. The causes of the drop-out were not always explained; the most common reasons were the absence of the post-test evaluation 45 or not being able to complete the intervention or a minimum of sessions.38,41,48
Main outcomes
The analyzed studies provided information regarding the impact of playing videogames on a number of outcomes related to physical, mental health, and cognitive function (Table 1). Physical health was represented by measures, including anthropometrics (body mass index [BMI], visceral fat, and body fat percentage), physical fitness (cardiorespiratory fitness, muscular strength and power, speed and agility and muscular flexibility), and motor skills (static and dynamic balance, motor proficiency). Mental health comprised anxiety, depression, and psychological wellness variables. Finally, cognitive function was evaluated by a wide range of indicators and instruments where attention, executive functions (working memory and inhibition among others), memory, and scholastics skills (mainly math and language) were the most commonly assessed aspects.
Physical health
Anthropometrics
Three RCTs38,39,42 assessed the effects of active videogame interventions on anthropometric measurements in study groups. Silva et al. 38 demonstrated waist circumference benefits only in the intervention group and greater visceral fat level benefits in the experimental compared with the control group. Dickinson and Place 39 revealed BMI benefits in both the intervention and the control group, but intergroup comparison showed no significant difference in this parameter after the intervention. Wing-Chung et al. 42 reported no benefits of a 12-weeks videogaming program on BMI nor body fat percentage.
Physical fitness
Five RCTs38,39,50,51,53 reported endpoints related to physical fitness when using exergaming. The four studies that covered variables in terms of cardiorespiratory fitness showed significant benefits, in this capacity itself38,39,51 or by changes in the heart rate.50,51
Findings associated with muscular strength and power were recorded in three trials.38,39,53 Silva et al. 38 observed lower limb power, trunk strength improvement in the intervention compared with the control group, and static arm strength improvement in both groups. Dickinson and Place 39 described lower limb power and trunk strength improvements favoring the intervention over the control group. Furthermore, Hsu 53 found that both videogame and physical education groups improved the lower limb muscle strength, but the sedentary group did not.
Speed and agility were assessed in two investigations.38,39 Both of them noted improvements in these variables. The same two trials also looked at muscular flexibility outcomes, with divergent results. While Silva et al. 38 identified improvements in this fitness dimension, the investigation by Dickinson and Place 39 evidenced the opposite effect, that is, improvement in the control group (physical education only) compared with the experimental group (physical education+videogames).
Motor skills
Six RCTs38,42,43,47,52,53 evaluated the effects of active videogame interventions on motor skills. Static balance was measured in four studies.38,42,52,53 Two of them52,53 found benefits, whereas the other two38,42 revealed a lack of significant differences for the control and experimental groups.
Dynamic balance was assessed in three investigations.38,43,53 Both Silva et al. 38 and Perrot et al. 43 yielded significant, positive effects on this outcome in favor of the experimental group.
Three studies38,42,47 evaluated other motor proficiency dimensions using subtests of the Bruininks–Oseretsky (apart from the balance subtest previously reported). Silva et al. 38 recorded benefits in response speed in the intervention group, but no intergroup significant differences were evident after intervention completion. After the intervention, participants in the RCT by Wuang et al. 47 manifested improvement in motor proficiency, visual-integrative abilities, and sensory-integrative functioning due to the exergaming intervention compared with standard occupational therapy and control group. Contrarily, Wing-Chung et al. 42 detected no significant differences between experimental and control groups in motor proficiency.
Mental health
One RCT 49 explored the effects of a videogame intervention on participants' mental health: anxiety, depression, and psychological wellness. The results revealed a significant anxiety reduction (improvement) in the computerized cognitive-behavioral therapy group compared with the usual psychiatric treatment.
Another trial 41 implemented an intensive computerized cognitive training program and observed no significant training-related changes in scores on the Strength and Difficulties questionnaire used to measure child behavior.
Cognitive function
Nine RCTs40,41,43–48,54 measured outcomes related to cognitive function. Siberski et al. 48 detailed improvement on 6 out of 15 cognitive function variables in the intervention group, whereas placebo and waitlist control groups exhibited benefits in 4 of 15 cognitive function parameters. However, after the intervention, there was an absence of significant differences between all groups regarding cognitive function outcomes. Rezaiyan et al. 54 noted significant benefits in attention for the experimental group, and Van der Molen et al. 45 did so in verbal short-term memory. Jansen et al. 44 reported benefits in math skills in favor of the experimental group due to the intervention.
In contrast, Söderqvist et al. 41 showed a significant improvement in language comprehension in favor of the intervention group compared with control at 5 weeks, yet only for female participants. At the end of the intervention, Standen et al. 40 observed that the experimental group surpassed the placebo group in three cognitive outcomes: Picture Guess Test, Picture Completion, and game score. Perrot et al. 43 noted an absence of a statistically significant intervention effect for improving visuospatial short-term working memory and selective attention. Bennett et al., 46 demonstrated that the intervention yielded a significant benefit to cognitive variables for the experimental group; however, only the experimental group exhibited a significant improvement in the visuospatial working memory experimental group compared with controls after the intervention period.
Finally, Wuang et al. 47 detected significant improvements in motor proficiency, visual-integrative abilities, and sensory-integrative functioning that favored the experimental group compared with controls after 24 weeks of intervention.
Discussion
The purpose of this research was to conduct a systematic review aimed at describing the effects reported in the existent RCTs that have used videogaming as an intervention strategy for improving the physical and mental health and cognitive function in people with ID. The information provided in this study could be useful for health professionals and researchers whose goal is to design rehabilitation programs to enhance the physical and mental health and the cognitive function of this population.
The obtained results indicated the existence of a considerable number of RCTs, although they presented a medium methodological quality. Blinding of participants, therapist, and assessors, along with allocation concealment and an intention-to-treat analysis of the results, deserve greater attention in future research on the topic. Yet despite these procedural issues, some of the findings derived from the analysis of these studies deserve further discussion since they provide valuable information.
For instance, it is noteworthy that not only playing exergames but also undergoing targeted computerized cognitive training programs based on executing tasks in a game environment, proved to be helpful for those with ID. Nevertheless, it should be noted that adherence rates were not consistently recorded across the studies; and although among the RCTs that registered drop-out rates, these have been low, less than half of the reviewed trials provided drop-out data.
On top of that, no information was shown regarding cost-effectiveness, and just two of the investigations46,47 offered details regarding the strategies to ensure fidelity of the intervention. This is an important point to consider since identifying treatment fidelity is essential to interpreting the results and whether the interventions produced the intended outcomes. 55 Altogether, these findings indicate the need for further research that properly addresses the feasibility of videogaming interventions on individuals with ID.
It is also remarkable that a number of RCTs analyzed the impact of playing active videogames on the physical health of both children and/or adolescents and adults with ID. Five investigations38,39,50,51,53 explored the effectiveness of exergaming on physical fitness, which is deemed an essential factor for increasing survival in those with ID. 56 However, only three trials38,39,42 were focused on body composition, a remarkable health-related fitness dimension. 57 This lack of research could be due to the fact that exercise programs aimed to reduce body weight in persons with ID are difficult to implement. 58 Besides, it seems that comprehensive interventions combining diet, exercise, and behavior change techniques must be carried out in this population for achieving positive BMI changes. 59
Despite this observation, two studies38,39 revealed positive body composition outcomes, and another research 42 indicated no marked effect on body composition after implementing an exergaming intervention. This is an interesting finding, as not all the studies that have proposed exercise interventions in people with ID have found significant improvements on this marker of health. 5 The results of the aforementioned two trials38,39 lend force to the previously suggested idea regarding the value of exergaming (i.e., sports-related and dancing games bundled with the Nintendo Wii gaming system utilized in both investigations), as a viable alternative for alleviating the growing rates of obesity in this population. 60
In this line, exergaming showed a positive effect on important health-related fitness dimensions such as cardiorespiratory function38,39,50,51 and muscular strength.38,39,53 These yields imply that playing active videogames can be a valuable resource for promoting an active lifestyle among those with ID, as it has been already observed in other populations. 61
In parallel, this review intended to show the existing scientific evidence regarding the impact of videogaming on mental health and cognitive function. With respect to the first facet, it was noticed that computerized cognitive-behavioral therapy showed to be effective on mental health outcomes, including depression or anxiety, in adults with ID. 49 This finding is consistent with prior observations suggesting the beneficial effects of videogaming on adults' mental health, 62 and remarks the potential interest of computer-based cognitive training programs for individuals with ID. Nevertheless, it must be pointed out that only two articles41,49 addressed the topic of mental health, implying that further studies are required to confirm the efficacy of this therapy.
Opposite to the lack of research on mental health, nine articles40,41,43–48,54 analyzing the impact of videogaming on cognitive function were found. On one side, seven of these investigations40,41,44–46,48,54 conducted computerized adaptive training and subsequently reported significant beneficial effects on different cognitive domains such as recognition, visual working memory, visual motor integration, and attention, mostly in adults with ID. On the other side, the other two studies43,47 were based on exergames. Although Perrot et al. 43 detected no changes in cognitive outcomes after a 12-week Wii™-based program for adults with DS, participants with DS 7–12 years of age who underwent a 24-week Wii-based training intervention exhibited improved visual-integrative abilities and sensory-integrative functions. 47
These results are in line with previous observations suggesting that videogaming is positively associated with cognitive performance in select cognitive domains. 63 Although other investigations have informed about the influence of exercise on the cognitive function of those with ID, 64 it seems that more research is needed on this topic. Thus, the findings described in this study help to increase the existing scientific evidence in this regard.
In the present review, we found six studies38,42,43,47,52,53 analyzing the influence of exergaming on motor skills, with the majority focused on the youth population in particular.38,42,47,52,53 This is a key issue because motor skills are an outcome that is not usually included when performing RCTs with people with ID, especially in children, who must be the target group for these efforts. 65
It should also be noted that we included balance as a motor skill, hence the number of RCTs reported. Notably, the impact of exergaming on balance was mixed,38,42,43,52,53 indicating that this might not be the best rehabilitation approach for this outcome. However, it is vital to remark that evidence regarding the effects of exercise interventions on balance in individuals with ID remains inconclusive.66,67 Thus, it seems that the influence of playing active videogames on balance is not so different from what has been described in other systematic reviews on this topic. On a final note, our findings suggest the need for further studies addressing the impact of exergaming on the motor skills of adults with ID since the available scientific evidence has been mainly targeting children. 68
In this piece of research, studies including both adult and young populations mostly with mild-to-moderate ID were reviewed. Although ID causes were not always reported, three exergaming interventions38,47,52 focused on young people with DS were found. This is a fact of particular concern since the population with DS has shown a high obesity prevalence, 69 but according to previous findings 70 and our results, exercise-based programs seem to be insufficient to achieve weight or fat loss.
In closing, practitioners working with persons with ID should be aware that active videogames might be an interesting option for increasing their fitness levels, while targeted computerized cognitive training based on performing tasks in a game environment may positively affect their cognitive function.
Nonetheless, practitioners seeking to use these approaches must notice the importance of the appropriate staff to maximize its benefit. Hence, it is recommended the supervision and support of staff (i.e., teachers, therapists, caregivers) who can provide the encouragement and motivation needed for continued effort during playing and individualized instructions fitted to the person's ability to play the videogame. When the individual with ID is performing challenging moves in the context of exergaming, these professionals are ready to intervene at once when their aid might be needed.
The main strength of this research lies in its originality since it provides a critical analysis of the highest methodological quality evidence about the effectiveness of videogaming on those with ID. Nevertheless, there are also methodological weaknesses that should be acknowledged. First, in some studies, the sample size was small, and the participants' profiles (especially age range, ID cause, and severity) varied among the analyzed investigations. Thus, the heterogeneity of the data did not make it possible to perform a meta-analysis and prevents the generalization of the reported findings to all people with ID. Second, the reviewed trials were predominantly focused on fitness and motor skills, with few studies addressing the significance of playing active videogames on important health outcomes such as body composition.
On top of that, only five RCTs detailed data on adherence rate and were not entirely comparable among trials due to divergences in the reporting method for this outcome, while information regarding drop-outs was not always available. This combination of findings implies that it was impossible to properly discuss the interventions' feasibility. In addition, there are limitations related to the language restrictions and the publication bias, which may have conditioned the results of this review.
Further research with greater training intensity is warranted to show whether active videogames provide additional physical and mental health benefits in this population. Likewise, more studies are required to elucidate the impact of playing exergames in the cognitive function of those with ID. Eventually, the scant information on the effects of videogames on psychological factors, behavioral change, and quality of life must be considered by future researchers in the field of ID.
Conclusion
Videogaming is a useful therapy for improving physical and mental health in people with ID. Exergaming seems to be an interesting physical intervention for increasing fitness and motor skill levels, whereas sedentary videogaming has shown potential for stimulating cognitive function. Further research to analyze its feasibility and its impact on body composition is needed.
Footnotes
Authors' Contributions
J.R.M.M. and C.A.P. worked on the concept and design of the study. D.S.-I., O.M.-Q., and J.R.M.M. took part in the acquisition of data. D.S.-I. and O.M.-Q. did the analysis of data. D.S.-I., O.M.-Q., and C.A.P. did the interpretation of data. D.S.-I., O.M.-Q., and C.A.P. did the critical review. C.A.P. coordinated the article preparation. All authors were involved in drafting the article, have read and approved the last version to be published, while they also agree with the order of presentation of the authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.