
Abstract
Objective:
The purpose of this study is to investigate the effect of Leap Motion Based Exergame Therapy (LMBET) on upper limb gross grip strength (GGS), pinch forces, hand functions, gross motor function, and cognitive functions in patients with cerebral palsy (CP).
Materials and Methods:
Twenty patients with CP (11 hemiplegia and 9 diplegia) were included in the study. Structured Neurodevelopmental Therapy-based hand rehabilitation (SNDTBHR) (first treatment period) was applied a total of 12 sessions, 2 sessions per week (total 6 weeks), and then LMBET (second treatment period) was applied a total of 12 sessions, 2 sessions per week (total 6 weeks). GGS was evaluated by “dynamometer,” pinch strengths were evaluated by “pinch meter,” hand skills were evaluated by “Manual Ability Classification System (MACS)” and “Jebsen-Taylor Hand Function Test (JHFT),” the gross motor level was evaluated by “Gross Motor Function Classification System (GMFCS),” and cognitive functions were evaluated by “Wisconsin Card Sorting Test (WCST).”
Results:
Significant difference was found between LMBET and SNDTBHR on GGF, pinch forces, JHFT, and WCST in favor of LMBET (P < 0.017). There was no significant difference between both MACS and GMFCS measurements (P > 0.05).
Conclusion:
Positive effects of both SNDTBHR and LMBET have been found. However, measurements after LMBET are statistically more significant. Future research should take into account higher patient allocation. Including additional leap motion training to conventional physiotherapy is feasible and might be promising to train cognitive function in children with CP.
Introduction
Cerebral palsy (CP) is defined as a permanent group disorder in the development of movement and posture that causes activity limitations attributed to the nonprogressive disorders occurring in the developing fetal or infant brain. 1 Upper limb functions play an important role in carrying out activities of daily living (ADL) in children with CP. The negatively affected upper limb functions are one of the most important conditions that limit ADL in children with CP. Due to motor dysfunctions caused by CP, it is difficult to perform movements within the normal pattern due to problems in gross and isolated fine grips and restriction in the thumb and other fingers. 2
Cognition and perception are important for the person to interact successfully and purposefully with his environment. While cognition enables the processing, storage, and manipulation of information, perception allows the senses to integrate with meaningful information. 3 Cognitive disorders occur with difficulties in the information processing process, associated with immature brain damage. 4 Recent research has started to examine executive function among children with CP. In one study, children 9–13 years of age with unilateral (n = 14) or bilateral CP (n = 18) were found to have attentional and executive function impairments. 5
Working memory deficits among children with unilateral, bilateral, and ataxic CP have also been shown, with lower working memory skills predicting poorer arithmetic skills.6,7 The Wisconsin Card Sorting Test (WCST) has also been used to examine executive function in children with CP (37 unilateral CP and 15 bilateral CP), and it was found that, compared with typically developing children, children with CP had more difficulty completing the task. Executive functions are the primary control mechanism for purposeful behavior. The main task of this mechanism is to respond to unusual situations. Especially, when alternative movement strategies are required for the compensation of limb weakness, disorders in executive functions cause the rate of gaining independence in ADL to decrease.
Cognitive disorders can delay functional recovery by reducing adherence to treatment and participation in rehabilitation. It also has a significant impact on independence and quality of life.5,8 Studies are showing that virtual reality-based treatments are effective in improving cognitive functions.9,10 Oh et al., demonstrated the effectiveness of virtual reality-based treatment on cognitive functions in patients with stroke. 11 However, we could not find a study investigating the effect of a virtual reality-based treatment on cognitive functions in children with CP in the literature.
There are several treatments known to be effective in CP such as physical therapy, occupational therapy, pharmacological therapy, surgery, and orthotics. Physical therapy plays a central role in disease management through a focus on improving posture, balance, mobility, strength, and function. However, children find physical therapy ordinary and uniform. Neurodevelopmental therapy (NDT), which aims to target central nervous and neuromuscular systems and teaches the brain to improve motor efficiency and achieve maximum functional independence by facilitating controlled movements of motor posture, is one of the most used treatment methods in children with CP.12,13
Leap Motion Based Exergame Therapy (LMBET) is a newly emergent treatment for motor rehabilitation of children with CP. With the development of technology, the use of LMBET in CP rehabilitation is increasing. LMBET is provided through a computer-simulated environment where it interacts with real world-like objects and events through image, sound, smell, and touch. 14 LMBET interventions try to promote neuroplasticity and motor learning through this computer-simulated environment. 15
The aim of this study was to investigate the effect of LMBET on gross grip strength (GGS), pinch strengths, hand functions, gross motor function, and cognitive functions. We hypothesized that LMBET added to routine therapy would be more effective than structured exercises added to routine therapy to train hand function and cognitive functions in children with CP as a therapy.
Materials and Methods
Study design
The study was a repeated measures designed study.
Ethics committee approval and study participation consent
The study was approved by the Institutional Non-Invasive Ethics Committee (Approval date: November 1, 2019 Approval No. 10840098-604.01.01-E.1469). When reporting experiments on human subjects, authors should indicate whether the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Participants
Eligibility criteria
Patients diagnosed with CP, who were diagnosed with health reports and complied with inclusion criteria, were included in the study. At the beginning of the study, 31 patients were included in the study, but according to exclusion criteria, 4 patients with Botulinum toxin (BOTOX) injection, 4 patient having Communication Function Classification Scale (CFCS) level >3, 2 patients with epilepsy, and 1 patient using hand orthosis were excluded from the study. The study was completed with 20 participants. Figure 1 presents the CONSORT flow diagram of patient selection and allocation in this study. The inclusion criteria defined as having been diagnosed with CP in the health committee, being between 8 and 15 years old, having a mental level as “normal” or “mild mental retarded” (in terms of compliance with the exercises), according to Modified Ashworth Scale having upper limb spasticity (0), (1), and (1+), CFCS having level (1), (2), and (3), and accepting to participate in the treatment after reading the consent form of the family. The exclusion criteria defined as BOTOX injection has been made for the hand joint in the last 6 months, having a history of hand surgery, having a diagnosis of epilepsy, using a hand orthosis, any diagnosed cardiac or orthopedic conditions that may impede the treatment and treatment practices, and presence of contractures in the upper limbs.
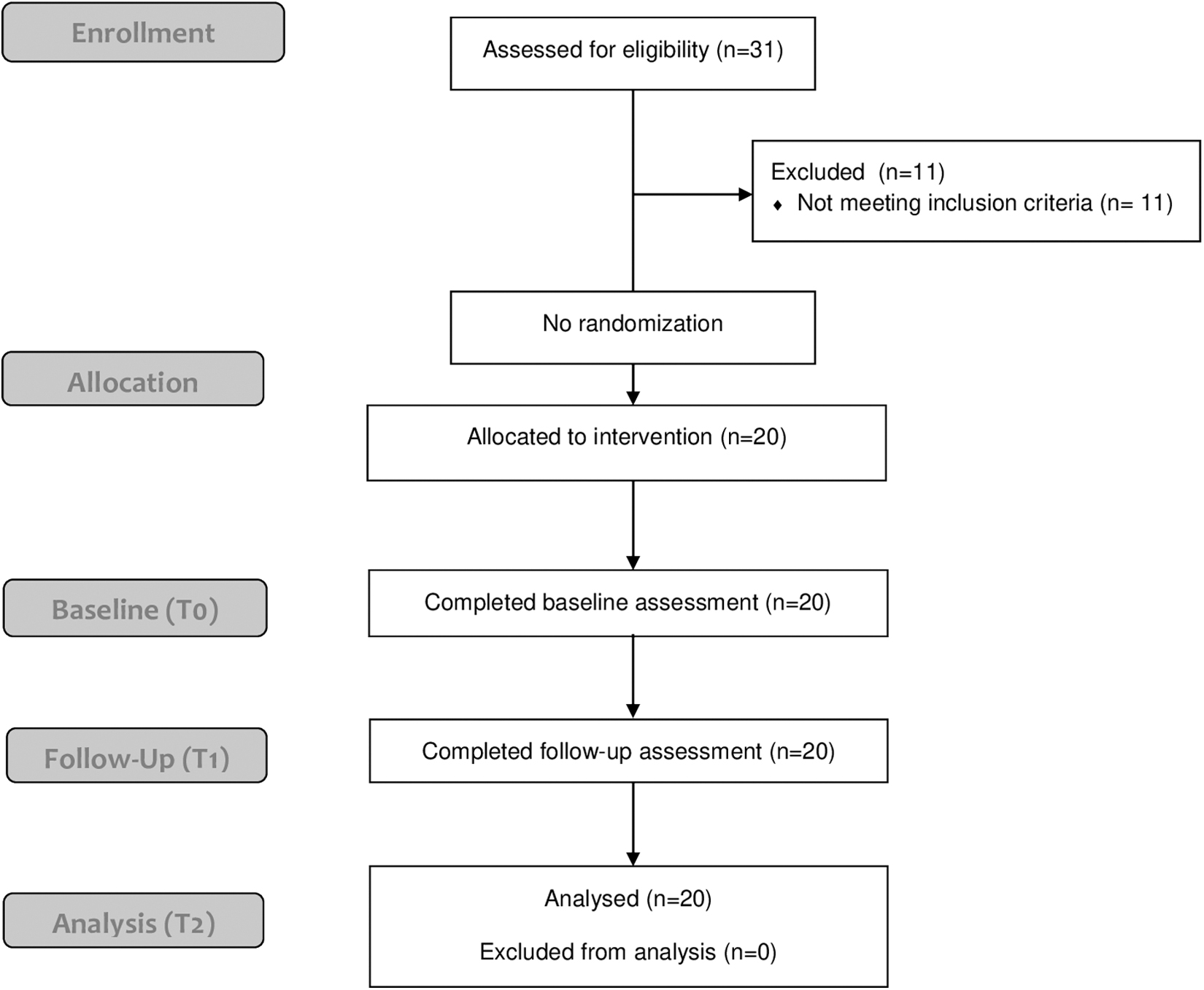
CONSORT flow chart.
Interventions
Twenty patients who met the inclusion criteria were included in the treatment after they were informed. The patients were evaluated at the baseline (T0). They received a total of 12 sessions of Structured Neurodevelopmental Therapy-based hand rehabilitation (SNDTBHR), 2 sessions per week over 6 weeks. Then the second assessments were made (sixth weeks-T1). After the second assessment, they received a total of 12 sessions of LMBET, 2 sessions per week over 6 weeks, in addition to NDT. Then they were evaluated at the end of the study (12th weeks-T2).
SNDTBHR protocol
During the first treatment period, patients were treated with 20 minutes of NDT-oriented exercise, including individual balance, strengthening, walking, gross motor exercises, and 20 minutes of SNDTBHR. SNDTBHR included the exercises such as placing the pegs in the area of the same color, removing the ropes inside the box through the bead, removing the sticks with the pinch grip, picking the soft objects with the pinch grip, and placing the shapes in the appropriate place. The first treatment period, which includes a total of 12 sessions SNDTBHR, continued for 2 sessions per week over 6 weeks.
LMBET treatment protocol
In the second treatment period, patients received NDT-oriented exercise for 20 minutes, including balance, strengthening, walking, and gross motor exercises, in addition to LMBET for 20 minutes. The aim of the developed games was to improve the joint range of motion (ROM), muscle strength, coordination, and fine motor functions of the hand and wrist in patients. Two games called “Fizyosoft CatchAPet” and “Fizyosoft Leapball” were developed using Leap Motion with funding support (supported by The Scientific And Technological Research Council Of Turkey form under 3001-Starting Research and Development Projects Funding Program Project No. 215S191) (Fig. 2). The games were developed for using in LMBET rehabilitation program (Fig. 3). 16

Leap motion application on children with CP. CP, cerebral palsy.
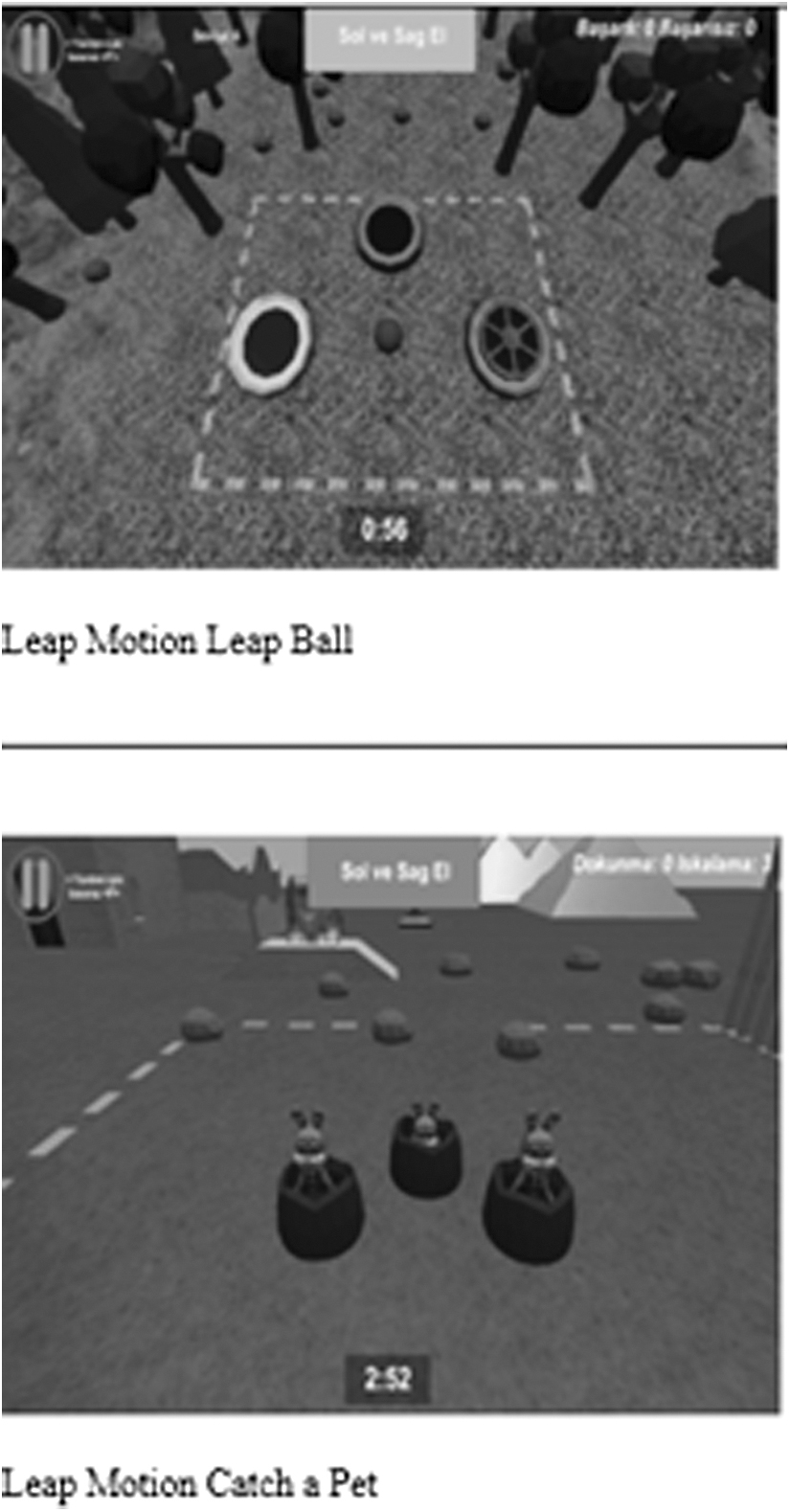
Examples of Leap motion games.
In the Leap Ball game, the balls were asked to be grasped and thrown into the box of the same color. The objective of this game is to prevent complications, to realize the grip in the correct movement pattern, and to ensure correct color matching.
In the Catch a Pet game, it was aimed to touch the moles that come out of five different holes in a certain order by aiming for repeated wrist flexion and extension. In this game, it was aimed to increase the score in the game by shortening the reaction time by predicting which hole the next mole will come out with verbal feedback. Executive functions were also tried to be activated by this way. Both hand rehabilitation programs consisted of regulation of impaired tone, regulation of impaired sensory-perception-motor integrity, facilitation of low-quality ADL, and exercises aimed at activating executive functions.
Measurement
Assessment administration
Assessments were performed at baseline (T0), 6 weeks (T1), and 12 weeks (T2).
Clinical and sociodemographic characteristics
At baseline, name, surname, gender, age, weight, height, body mass index, dominant hemisphere, CP type, affected limb, CFCS, and device information were recorded on the demographic data form.
Outcomes
The primary outcome was to evaluate the performance of hand function with the Jebsen-Taylor Hand Function Test (JHFT).
The secondary outcomes were to evaluate the GGS with “dynamometer,” to evaluate the pinch strengths with “pinch meter,” to evaluate the hand skills with “Manual Ability Classification System (MACS),” to evaluate the gross motor level with “Gross Motor Function Classification System (GMFCS),” and to evaluate the cognitive functions with “WCST.”
Jebson-Taylor hand function test
The Jebsen-Taylor hand function test, including seven subcategories, was used as the inventory against which to measure upper limb function. The Jebson-Taylor hand function test provides objective measurement data on standardized performance, which may be compared with patients' performance, extensively evaluates hand functions generally used in daily living, enables the continuity of ability within individual hand function evaluation ranges to be recorded, and is easily applied in a short period. 17 The test consists of 7 items, including writing a 24-letter sentence, turning over 5 cards, picking up small common objects (2 pennies, 2 bottle caps, and 2 paper clips), simulated feeding using a teaspoon and 5 kidney beans, stacking 4 checkers, picking up and moving 5 large empty tin cans, and then 5 large full cans. 18
Manual Ability Classification System
Manual abilities were assessed according to the MACS, which classifies children's ability to handle objects in everyday activities on a five-level scale: level I—highest ability—the child handles objects easily and successfully; level II—the child handles most objects, but with somewhat reduced quality and/or speed of achievement; level III—the child handles objects with difficulty, needs help to prepare or modify activities; level IV—the child handles a limited selection of easily managed objects in adapted situations, and level V—most limited ability—the child does not handle objects and has severely limited ability to perform even simple actions. 19
Gross Motor Function Classification System
Employing GMFCS as the international standard for classifying the severity of CP, children were categorized preoperatively by gross motor activity as follows: group I—walking without limitations; group II—walking with limitations; group III—walking using a hand-held mobility device; group IV—independent mobility achievable with limitations, may use powered mobility; and group V—no means of independent mobility, transport dependent on the assistance of another. 20
Wisconsin Card Sorting Test
WCST consists of 4 stimulus cards and 128 response cards that depict figures of varying forms (crosses, circles, triangles, or stars), colors (red, blue, yellow, or green), and the number of objects (one, two, three, or four) on them. As the task is usually administered, the four stimulus cards with the following characteristics are placed before the subject in left-to-right order: one red triangle, two green stars, three yellow crosses, and four blue circles. The subject is instructed to sort each response card under one of the stimulus cards, whichever he or she thinks is correct. After each sort, the subject is told whether the sort was right or wrong. The subject must discover the correct matching rule using this feedback (right or wrong). No other instructions are given throughout the test. The instructor begins by responding “right” each time the subject matches for color. This continues until 10 consecutive cards have been sorted by color. The examiner then, without forewarning or comment, changes to “form” as the correct response. After 10 consecutive forms' responses, the principle changes to “number” and so on. The test continues until either the subject has completed 6 categories or all 128 cards have been used. 21
Statistical analysis
The sample size was determined using the G*power sample size calculator. The required sample size was 30 with an 85% power and 15.05% confidence interval (α = 0.05), considering the minimal clinically important difference of 30 points in the JHFT. 18 We aimed to enroll at least 20 participants considering the dropouts.
“SPSS 22.0 (Statistical Package for Social Science) for Windows” program was used for statistical analysis. The normal distribution of variables was examined with the Shapiro–Wilk test. Demographic data were analyzed for descriptive analysis and frequency. The data difference between all evaluations performed at different times was evaluated using the “Friedman Test.” “Bonferroni-corrected Wilcoxon Test” was used as a post hoc test. The significance value was accepted as P ≤ 0.05 for the Friedman Test, and the significance value for the Wilcoxon Test with Bonferroni correction was P ≤ 0.017.
Results
Twenty patients with CP were analyzed in this study. The mean age was 12.50 ± 2.50 years. All sociodemographic and clinical data of the patients are shown in Table 1.
Distribution of Demographic Data
BMI, body mass index; CFCS, Communication Function Classification Scale; CP, cerebral palsy; SD, standard deviation.
Primary outcome
Hand function (JHFT)
There was a significant difference between three measurements in all subparameters (Table 2).
Mean Differences in Follow-Up Evaluations
P ≤ 0.05.
GMFCS, Gross Motor Function Classification System; MACS, Manual Ability Classification System.
Secondary outcome
Hand skills (MACS)
There was no significant difference between three measurements.
Gross motor level (GMFCS)
There was no significant difference between three measurements.
Gross grip force and pinch forces
There was a significant difference between three measurements.
Executive function (WCST)
A significant difference was found between three measurements in some subparameters (Table 2).
When the JHFT results were compared, a statistically significant difference was found in favor of LMBET in all subparameters. When the grip strength results were compared, a statistically significant difference was found in favor of LMBET in all subparameters. When the WCST results were compared, a statistically significant difference was found in favor of LMBET in all subparameters (Table 3).
Post Hoc Analyses
Discussion
The aim of our study was to investigate the effect of LMBET on gross grip force, pinch forces, hand functions, gross motor function, and cognitive functions in patients with CP. CP is the most common cause of motor dysfunction in children, and cognitive impairment occurs in about half of patients with CP. 22 These dysfunctions reduce the level of independence in ADL. Therefore, the treatment of these functions is of great importance in rehabilitation. NDT is the most preferred method in the treatment of CP. LMBET is a treatment method that has been used recently. 23 As a result of the literature review, there is no study investigating the development of both hand functions and cognitive functions. We designed our study in this way because we aimed to run these two functions at the same time and reveal their development.
Piaget's cognitive development includes four stages such as the Sensory-Motor Period, Pre-Process Period, Concrete Process Period, and Abstract Process Period. He argued that the child can create sound concepts in preschool, but his thoughts have flaws such as egocentrism and belief in magic. He also stated that children can perform concrete operations after the age of 7. According to Piaget's theory, cognitive functions such as children, information processing, logic, and memory reach maturity during this period. In light of this information, the age range was determined to be 8–15, while the inclusion criteria of the study were established. 24 Considering that children younger than 8 years cannot be successful in skills that require concrete processing, the minimum age was determined to be 8. López-Vicente et al. have determined the 8–10 age range as a criterion in their study, where they investigated the effect of physical activity on cognitive function. 25 However, there are studies in different age ranges. 22
Innovative computer-based technologies are seen as important support for increasing neuroplasticity during rehabilitation. These technology-based methods enrich the traditional rehabilitation environment by increasing special feedback on results and motor performance. It was shown that increased feedback can modulate sensorimotor cortical activity by facilitating learning in selected brain networks. 26 Virtual reality comes to the fore among technological approaches.27–29 Avcıl et al., in their study, divided the children with CP into two groups and applied videogames to one group and NDT—Bobath to the other group. 30 They found significant changes in the Minnesota Manual Dexterity Test in their upper limb rehabilitation program in children with CP, who performed videogames. Kassee et al., in their study of home-based Nintendo® Wii™ study in children with diplegic CP, found a statistically significant improvement in grip strength. 31 Do et al., in their study, which included bilateral upper limb activities in Nintendo Wii in children with hemiparetic type CP, they found significant changes in the coordination of bilateral hand activities and in the Pediatric Motor Activity Log test in which they evaluated ADL. 32 Maltais et al., in a study that investigated the effect of exercise on cognitive functions in children with CP, it was shown that exercise improved cognitive functions with significant changes in the Stroop Test. 33 Gamito et al. found significant increases in the Wechsler Intelligence Questionnaire in their study where tasks such as shopping, matching numbers, calculating money, and keeping in mind were designed with virtual reality glasses. playing games derived from ADL. 34 In their pilot study, Faria et al. reported a significant improvement in the Fugl-Meyer Scale for upper limb functions, and the Montreal Cognitive Status Scale for cognitive functions as a result of the virtual reality therapy they applied to stroke patients. In this sense, our study shows similar features in the literature. 35 To our knowledge, there are not many studies combining cognitive rehabilitation and motor therapy, and there are also no studies evaluating cognitive functions and hand functions with LMBET in CP. In this sense, our study is the first study in the literature.
Gross gripping force is one of the most frequently used functions in fulfilling needs in ADL. The resting position most commonly seen in spastic type CP includes elbow flexion, forearm pronation, wrist ulnar deviation, thumb adduction, and flexion, and is due to muscle imbalance and/or weakness. This causes rough comprehension and deficiencies in hand skills. 36 Klingels et al. reported that the dynamometer was highly reliable to measure the rough grip force in patients with hemiplegic type CP. 37 In our study, we used hydraulic dynamometers, while evaluating these forces. In the study, an increase was observed only in measurements after LMBET (T2). When the rough grip force and pinch force measurements were compared, it was seen that the significance was in favor of LMBET (T2). We think that this result is due to the long-term isometric contractions in Leap Motion games and the materials we use in NDT-based hand rehabilitation being insufficient in strengthening muscles and hand functions.
Motor, sensory, and cognitive integrity are required for normal development. Fine motor development steps, in which the upper limb development is active, play an important role in the neuromotor development of the child. 38 The use of the hand in ADL is important for the activities to be done independently. Abnormal postures and deformities caused by spasticity restrict upper limb functions, make ADL more difficult, increase the burden of caregivers, 39 and negatively affect the child's participation in family, school, and social activities. 40 The JHFT is often used in clinical practice and research to evaluate hand functions by simulating ADL in children with CP.18,41 At the end of our study, JTHFT results were significant when the third measurement (T2) performed at the end of LMBET treatment was compared with NDT-based hand rehabilitation and the first measurement in all subtests. Acar et al., in their randomized controlled study combining NDT-based upper limb rehabilitation and Nintendo Wii-based Virtual Reality Therapy (VRT) in children with CP, found that the JTHF results in the NDT-VRT group were more important. 42 Shin et al. in their randomized controlled study on stroke patients, applied therapy with a virtual reality-based Smart Glove system that detects and provides all movements of the finger and wrist, and applied occupational therapy, including ADL and strengthening exercises, to the other group. The treatment lasted a total of 4 weeks. They found that the treatment applied with the virtual reality-based Smart Glove system was more significant in the JHFT results in other subtests, except for the subtests of four standard objects, instead of subtests for light and heavy objects. 43 However, we think that the important results of JTHF in all subtests in our study originated from the 6-week duration of our treatment. We also think that the leap motion system is more advantageous than the Smart Glove system, even if it is not wearable.
MACS is often used to classify the manual skill abilities of children with CP and is defined in how children use their affected hands during bimanual activities. 44 In a randomized controlled trial comparing conventional upper limb rehabilitation and Nintendo Wii-based upper limb therapy, Sharan et al. did not find significant changes in MACS scores in both groups. 45 All of the patients in our study ranged between level I and level III. We found no significant difference between treatments in MACS. However, after LMBET treatment, only one patient's MACS level changed from 3 to 2. Our study shows similar results to the studies. We think that the reason why the MACS results in our study were insignificant was that the treatment methods included intense and multiple repetitive exercises focused on comprehension and release. We believe that enriching the treatment program with functional exercises and activities, which will increase the performance of ADL, will create significant differences in MACS results.
Motor dysfunction in children with CP, limited ADL, and low participation in leisure activities causes a decrease in quality of life. 46 The severity of restriction in gross motor skills among children with CP has a wide scale of severity, from assistive devices to the use of battery-powered wheelchairs. 47 GMFCS is a widely used assessment method to be a descriptive layer system in children with CP. 48 Metin Ökmen reported that there was no significant change in GMFCS results in their randomized controlled trial comparing play therapy with NGT-based conventional upper limb therapy with virtual reality-based Play Station. 49 In our study, there was no difference between treatments in the GMFCS scores we used in evaluations. However, between the T1 and T2 measurements, only one child's GMFCS level changed from 3 to 2. We concluded that this result was due to the focus of our study on fine motor activity. The GMFCS level criteria were in a wide range from wheelchair users to the use of assistive devices, assisted walking and walking without support, and exercises were not structured to provide these changes.
The executive functions are the most affected cognitive functions in spastic type CP. 50 The WCST was used to evaluate executive functions in studies in children with CP.51,52 Rand et al., applied a total of 10 sessions over 3 weeks of Virtual Reality (VR) glasses therapy that include games that focus on multitasking and problem solving, browsing products, selecting them, and placing them in a shopping cart in 4 people who lack executive functionality and multitasking. As a result of the study, they reported that VR glasses are an effective intervention tool and errors were reduced in the Multiple Impact Test. 53 Optale et al., investigated the effectiveness of VR-based cognitive rehabilitation and music therapy in older adults with cognitive deficits. They reported that memory, attention span, and executive functions were improved, while visuospatial processing was improved in the VR group. 54 In our study, one of the subparameters of the WCST revealed important changes in the number of completed categories, the total number of errors, the number of persistent errors, the number of nonpenetrating errors, conceptual level responses, and the first response category LMBET (T2). There was no difference in only the perseverative response number subparameter. NDT-based hand rehabilitation did not reveal differences in any subparameters (T1). LMBET has been shown to cause superior differences compared to NDT-based hand rehabilitation. In line with our knowledge, cognitive-oriented studies in CP are mostly done to determine the cognitive level and do not include cognitive treatment. Our study, in line with our knowledge, is the first to investigate the effectiveness of LMBET in cognitive skills in children with CP and reveals its original value in this respect.
In accordance with the rehabilitation regulations in our country, children with disabilities are given two sessions of routine treatment per week free of charge by the state. Since it was not possible for us to eliminate this treatment process provided by the state free of charge, we were able to measure the immediate effects of the structured treatments we added to the routine treatments that were continued before the T0 measurement, in line with the treatment plan of our study. Also, we aimed to see the effects on the same patients due to the difficulty of randomization in CP. Even if the effect of the first treatment continues, when looking at the magnitude of the differences between measurements, it is thought that the immediate effect of LMBET treatment is greater.
The superiority of LMBET over NDT-based hand rehabilitation is remarkable. In our study, it was reported that LMBET can be used as an alternative to NDT-based upper extremity treatments.
The limitations of this study are the lack of clarity on whether the improvement in hand function improves due to NDT or LMBET and whether virtual reality-based Leap Motion increases motivation and desire to work in children, and body functions are not evaluated.
Conclusion
In conclusion, it was concluded that LMBET was effective on the ROM, GGS, pinch forces, and hand skills in cases with CP. It was observed that LMBET and SNDTBHRT did not change the gross motor level in cases with CP, and LMBET was effective on the cognitive functions of the cases with CP. Virtual reality therapy revealed more effective results on motor and cognitive functions compared to Neuro-Developmental Treatment in cases with CP.
Footnotes
Authors' Contributions
Y.Y.: the conception and design of the study, acquisition of data, and analysis and interpretation of data, revising the article critically for important intellectual content, and final approval of the version to be submitted. M.B.: the conception and design of the study, acquisition of data, and analysis and interpretation of data, drafting the article, and final approval of the version to be submitted. D.T.: acquisition of data, revising the article critically for important intellectual content, and final approval of the version to be submitted. Z.C.A.: the conception and design of the study, revising the article critically for important intellectual content, and final approval of the version to be submitted.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.