
Abstract
Objective:
The aim of the study is to analyze the effects of physical dance training with a virtual game on muscle quality (MQ) of community-dwelling older women.
Materials and Methods:
In total, 46 older women participated in the study and were assigned to either a control group (CG, n = 25, 71 ± 5 years) or training group (TG, n = 21, 69 ± 4 years). The following assessments were performed at baseline and after 12 weeks: quadriceps, ankle plantar flexor, and dorsiflexor isokinetic peak torque (PT) (Biodex System 4 Dynamometer); quadriceps cross-sectional area (CSA) measured using magnetic resonance imaging; intramuscular noncontractile tissue (IMNCT) (Image-Pro Plus 4.5.0.29 for Windows); and MQ (ratio of quadriceps PT to CSA). Each week for 12 weeks, the TG undertook three 40-minute sessions of physical training with the “Dance Central” game for Xbox 360® with Kinect, while the CG was instructed to maintain usual activities of daily living.
Results:
The TG increased quadriceps eccentric PT at 60°/s (P = 0.04) and ankle plantar flexor concentric PT at 60°/s (P = 0.02) when compared with the CG. No significant difference in quadriceps CSA, IMNCT, and MQ was observed.
Conclusion:
Physical dance training with virtual games can increase quadriceps and ankle plantar flexor strength without changing IMNCT and MQ of community-dwelling older women.
Trial number: RBR-8xkwyp (ensaiosclinicos.gov.br—Brazilian Clinical Trials Registry).
Introduction
In Brazil, 7.68% of the population is aged over 65 years. The majority of those aged over 65 years are women, and this group accounts for 4.17% of the general population. 1 The aging process is associated with a decline in muscle strength and mass, which are key aspects of muscle quality (MQ). MQ can be defined as muscle strength per unit of muscle quantity or per unit of muscle cross-sectional area (CSA).2,3 In addition to reduction in muscle mass related to the aging process, there are also changes in tissue quality, including increases in adipose tissue and in water content of skeletal muscle. Characteristics such as muscle architecture and composition, lipid content, and amount of connective tissue may affect muscle strength and are part of MQ. 4
In a 5-year study conducted with 1678 participants, a decrease of 11.1% in MQ of older women, representing 2.22% over a year, was observed. 2 It has been speculated that intramuscular adipose tissue can change MQ and impair muscle strength and functionality more than muscle atrophy. 5 In older people, poor lower limb muscle performance and increased risk of mobility limitations are associated with a high intramuscular adipose tissue level.2,4 This fact is especially important for older women due to a higher prevalence of musculoskeletal diseases, faster muscle loss,6,7 and higher functional limitations than men.8,9 Moreover, skeletal muscle maintenance is crucial to health throughout the lifetime, considering longevity of women. 7
The effects of physical training on intermuscular fat infiltration still need further investigation. High levels of thigh intramuscular adipose tissue seem to impair the adaptive MQ response to training in older adults even after 12 weeks of resistance, endurance, and balance exercises. 10 On the other hand, 12 weeks of aerobic training reduced intramuscular adipose tissue of sedentary older adults, without significant weight loss and with a concomitant increase in skeletal muscle power. 11 Thus, it is not known why intramuscular adipose tissue might impair MQ and the adaptive response to physical exercise in older women.
Dance training tends to increase adherence and encourage socialization and also promotes important improvements in physical fitness, such as balance, muscle strength, and power, mainly among older participants.11,12 It has been reported that exercise with virtual games or exergames (i.e., exercises through videogames) is an alternative to improve physical activity maintenance in older adults.13–15 A supervised dance intervention based on videogame choreography showed 96% adherence among physically older women. 13 In addition, dance training showed improvements in muscle mass of calf muscles, concentric plantar flexion peak torque (PT), dorsiflexion range of motion (ROM), 16 quadriceps eccentric PT and CSA, 15 and hamstring eccentric PT. 17 On the other hand, there were no significant enhancements in CSA of quadriceps and hamstrings after 12 weeks of virtual dance training among fallers and nonfallers. 17
Other studies reported increase in quadriceps and hip muscle strength after community-dwelling older people were subjected to different types of virtual game protocols for 8 to 10 weeks.18,19 Although studies showed exergaming as a possible method to improve musculoskeletal function, the potential reason why some older adults do not show change in MQ after training and the role of intramuscular adipose tissue in this mechanism are not well established. More studies are necessary to determine why intramuscular noncontractile tissue (IMNCT) might affect MQ in older adults.
Therefore, the aim of this study was to analyze the effects of physical dance training with a virtual game on MQ and their individual components, such as quadriceps, ankle plantar flexor, and dorsiflexor PT, quadriceps CSA, and IMNCT, in moderately active, community-dwelling older women. The hypothesis was that physical dance training with a virtual game, performed three times per week for 12 weeks, would be enough to increase the CSA, reduce IMNCT, and improve MQ and quadriceps, ankle plantar flexor, and dorsiflexor PT.
Materials and Methods
Design
This was a longitudinal, nonrandomized controlled study approved by the Research Ethics Committee of the Federal University of Paraná (CAAE 36003814.2.0000.0102) and registered at the Brazilian Clinical Trials Registry (RBR-8xkwyp). All participants signed an informed consent.
Participants
Sample size calculation was based on a distribution assuming 2 independent groups, using the GPower 3.1.9 program considering an effect size of 0.8 (large), an error type I of 0.05, and power analysis of 0.78, which estimated 52 people for the sample size. During the intervention period and postassessment, there was a sample loss of six individuals, which guaranteed the analysis, in a post hoc evaluation, a power equivalent to 0.74 for a sample size of 46.
To recruit participants, informative flyers and verbal invitations were handed out to senior groups and public health care ambulatories in Curitiba, PR, Brazil, and its metropolitan area. Initially, 147 participants were interested to take part in this study, but after the screening assessment, 95 volunteers did not meet eligibility criteria and were excluded. Thus, 52 older women were enrolled in the study and they could choose between participating in the control group (CG; n = 28) or the training group (TG; n = 24), according to their availability to come to the university for a physical dance program three times a week, which was required for the TG. At the end of the 12 weeks, the CG had the opportunity to take part in the training program and they had high adherence to the protocol. During the study period, three participants from the CG and three from the TG withdrew from the study and were excluded due to the following reasons: gave up after allocation (n = 3); hospitalization (n = 1); absence in the training (n = 1); and did not complete assessments (n = 1), as shown in the study flowchart (Fig. 1).
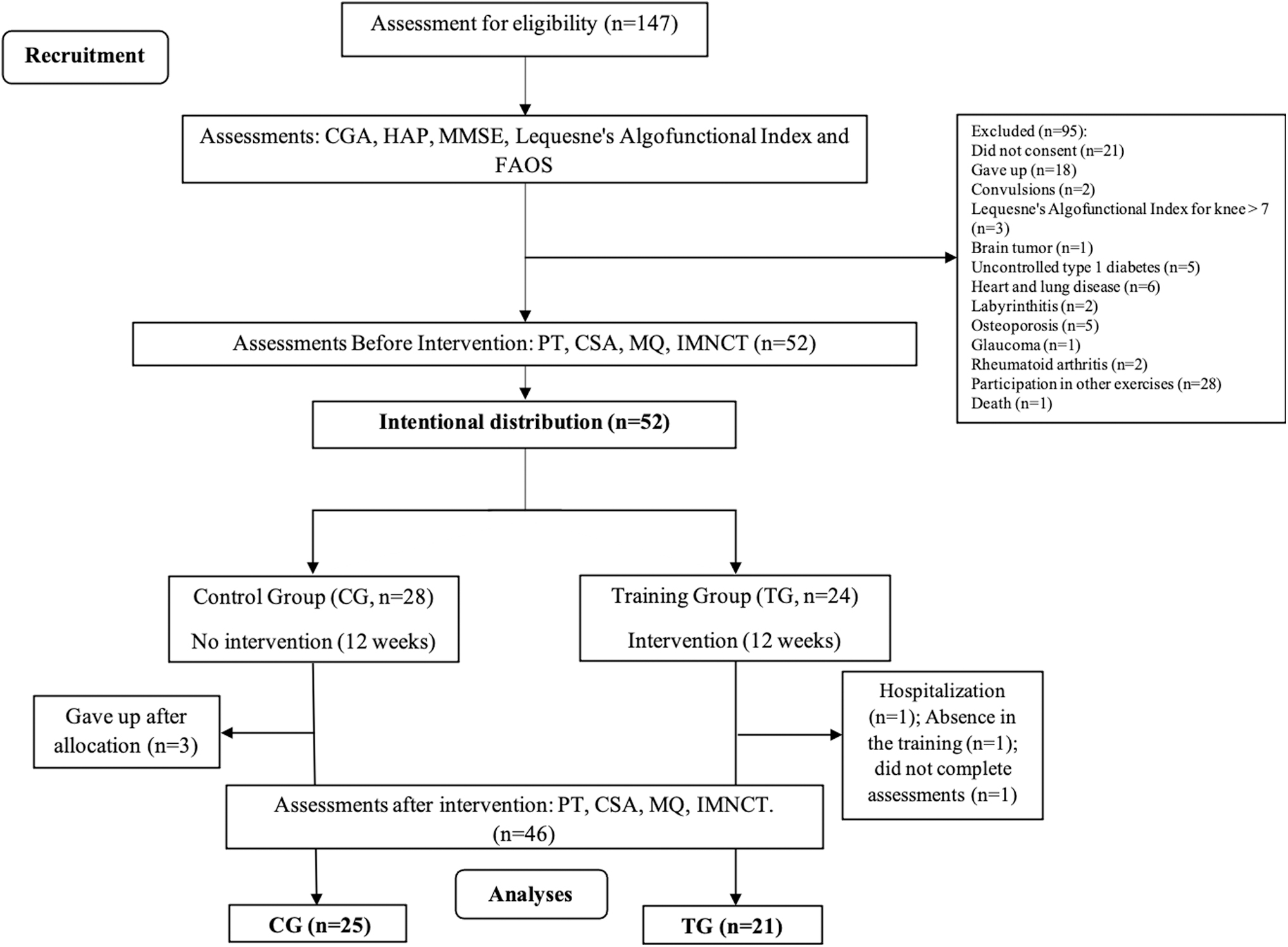
Study design. CGA, comprehensive geriatric assessment; CSA, cross-sectional area; FAOS, Foot and Ankle Outcome Score; HAP, human activity profile; IMNCT, intramuscular noncontractile tissue; MMSE, Mini-Mental State Examination; PT, peak torque; MQ, muscle quality.
The TG performed the physical dance training with virtual games three times a week for 12 weeks, with each session lasting 40 minutes. The CG was not subjected to exergame interventions as they were instructed to maintain normal activities of daily life during the study period. Both groups were assessed at baseline and after 12 weeks.
The inclusion criteria were female; age ≥65 years; cognitive status (Mini-Mental State Examination, score ≥24) 20 ; motor independence (Activities of Daily Living–Katz Index, score >6 21 ; Instrumental Activities of Daily Living–Lawton Scale, 22 score >21); ability to walk independently over a flat course of 10 m, with or without assistive devices 23 ; good functioning of the lower limbs (Lequesne's Algofunctional Index for Hip and Knee, final score <7, 24 and Foot and Ankle Outcome Score [FAOS], score ≥75 points) 25 ; good state of health according to a geriatric medical evaluation; and being at least moderately physically active (human activity profile, score >53). 26 Visual acuity was assessed by a geriatric physician through the Snellen chart and those with a score <20/70 were excluded, but participants could, if necessary, make use of eyeglasses or contact lenses for correction.
The following exclusion criteria were considered: neurological and vestibular disorders; tumors; rheumatic diseases; fractures; fixation or prostheses with metallic or nonmetallic implants; diagnoses of severe insufficiency (heart, respiratory, renal, hepatic, uncontrolled diabetes, and endocrine); and uncontrolled systemic arterial hypertension (blood pressure >140/90 mmHg). Those using drugs such as benzodiazepines and neuroleptics were also excluded since they affect balance. Furthermore, during the study, any of the following led to exclusion: any missed assessment; attending less than 60% of the physical training sessions or three absences in a row; and participant report of pain in any region of the body that would hinder completion of either the exercise sessions or assessments.
Procedures
Assessments before and after training included quadriceps, ankle plantar flexor, and dorsiflexor isokinetic PT and quadriceps analysis of the CSA, IMNCT, and MQ. PT was evaluated by an isokinetic dynamometer (Biodex System 4 Dynamometer; Biodex Medical Systems, Shirley, NY). Concentric and eccentric quadriceps isokinetic PT values were assessed in an ROM of 60° (from 90° of knee flexion to 30° of knee extension), 27 while ankle plantar/dorsiflexor concentric isokinetic PT values were assessed with an ROM of 30° (from 10° of dorsiflexion to 20° of ankle plantar flexion, maintaining a hip flexion of 100° and a knee flexion of 30°). 28 The isokinetic dynamometer assessments were performed at 60°s and 180°/s for both the knee and ankle, with a rest of 2 minutes between trials.
Axial magnetic resonance images were used to measure the quadriceps muscle CSA. Imaging was performed with a Siemens Magnetom Avanto 1.5, weighted imaging in T1, slice thickness of 9 mm, range of 1 mm, with 26 ms of echo time, and repetition time of 430 ms, in a matrix of 256 × 256 pixels. The CSA was measured with reference to the midpoint between the femoral condyle and the anterior superior iliac spine. 29
Image-Pro Plus software (version 4.5.0.29 for Windows) was used to quantify CSA and IMNCT, which automatically calculated the area of images from the sum of pixels, and values were displayed in cm2. The area of quadriceps muscle to be measured was marked before starting the automatic calculation. This procedure was done using the tool, Irregular area of interest (AOI), available in the software, in which muscle was represented by a darker gray tone, while the rest of the intramuscular noncontractile structures were a lighter gray. It was necessary to use the software's mask feature, which allowed separation of specific structures in each image by selecting the most frequent pixel color in each structure, so the program identified only the dark pixels and did not take into account the value of IMNCT and bone. After applying the color mask, according to the structure to be measured, the software automatically identified adjacent pixels of a similar color (gray tone), allowing selection of the total number of pixels. Muscle area delimitation was repeated three times and the average of those values was considered for the analysis.
MQ was estimated only for the quadriceps muscle by the ratio between torque (T) and muscle CSA (MQ = T/CSA).2,3
Interventions
The TG performed the physical dance training with virtual game using the Xbox 360® with Kinect motion sensor and the “Dance Central” game. Group exercises were carried out for a period of 12 weeks, 3 times per week, resulting in 36 training sessions, each with duration of 40 minutes. The 12-week program was determined because changes in muscle strength and mass occur mainly between 6 and 12 weeks.15,16 The dance games were chosen based on the criteria of neuromotor training progression proposed by the American College of Sports Medicine (ACSM), that is, progressive increase in the difficulty of movements. 30 The intervention progression also included the following: from the 7th to 12th week, participants performed the exercises with low lighting, on a 19-m2 polyurethane foam with 5 cm thickness; and from the 10th to 12th week, colorful and flashing lights were added to promote visual input perturbation, as shown in Figure 2. The group training was performed at the university, and the training protocol has been described in detail in previous studies.16,17 All sessions were supervised by physiotherapists and physical trainers.
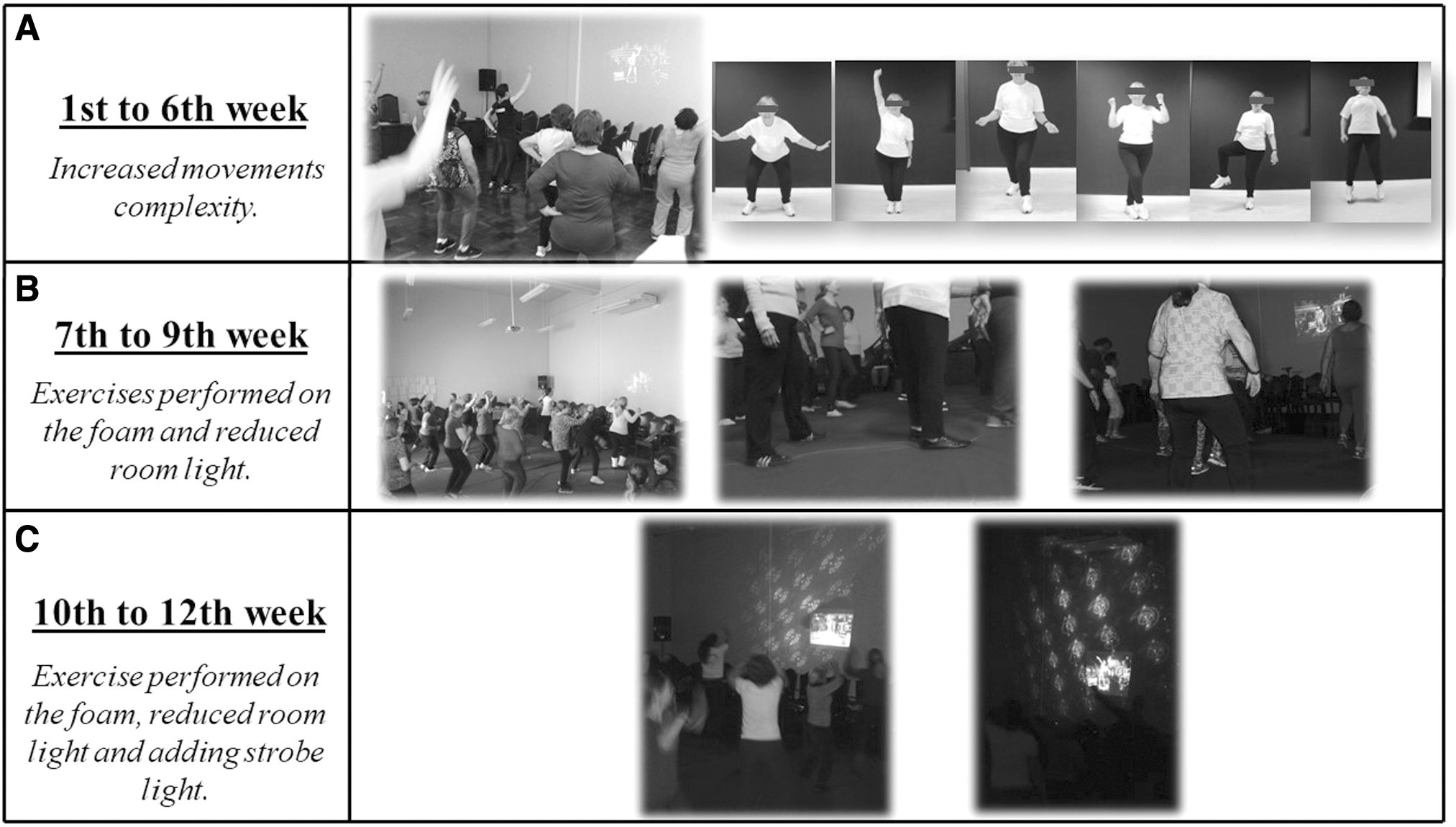
Training progression.
In addition, blood pressure was measured with a sphygmomanometer and a stethoscope (Premium) at the beginning and end of each training session, and training intensity was checked by heart rate (HR) and subjective perception of exertion (SPE). The HR was measured with a heart rate monitor (Polar®), while SPE was analyzed through the Borg Scale (score 6–20). 31 Both were assessed four times in each session: (1) at the beginning of the session; (2) after 10 minutes of warm-up; (3) after 20 minutes of dance training, and (4) after 10 minutes of relaxation, at the end of the session. The training protocol of the TG was designed to maintain exercise intensity at a mild to moderate level.
Statistical analyses
The Shapiro–Wilk test was used for data normality distribution analysis. For sample baseline characteristics, parametric data are presented as mean values (± standard deviation [SDs]) and an independent Student t-test was used for the analysis (height, weight, and body–mass index), while nonparametric data are presented as median values (minimum and maximum) and analyzed using the Mann–Whitney U test.
To compare training effects after 12 experimental weeks, the analysis of variance (ANOVA) mixed model test with 2 factors, group (CG and TG) and time (pre and post), was used, followed by the post hoc Bonferroni test for comparison between groups for parametric data. Only plantar flexion PT at 60°/s was significantly different between groups at baseline (P = 0.02) and was analyzed through ANCOVA, with the pre-experimental period value inserted as the covariable.
The intragroup and between-group effect sizes were also calculated using Cohen's d equation (considering the Pearson correlation coefficient, r) for dependent (d = t dependent √2(1 − r)/n) and independent (d = t independent √n1 + n2/n1*n2) samples.
Only one researcher analyzed the CSA and IMNCT, and the intra-rater intraclass correlation coefficient (ICC) and standard error of measurement (SEM) were calculated using the following equation: SEM = standard deviation*√(1 − ICC). For the CSA, the ICC was 0.999 and SEM 0.02; and for IMNCT values, the ICC was 0.996 and SEM 0.01. A significance level of P < 0.05 was adopted and statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 22.0 for Windows®.
Results
At baseline, groups were different in height (P = 0.03), FAOS pain score (P = 0.03), and plantar flexion PT at 60°/s (P = 0.02), and no other significant difference was observed among other characteristics (Table 1). Participants were classified as physically independent, without cognitive deficits, moderately active, and with little impairment in the lower limbs.
Sample Characterization
Results: mean ± SD; median (min–max).
A-F Lequesne: Algofunctional Lequesne test where 0: no impairment; 1–4: little impairment; and 5–7: moderate impairment.
Different from CG baseline (P < 0.05); independent Student's t-test; Mann–Whitney U test.
BMI, body–mass index; CG, control group; FAOS, Foot and Ankle Outcome Score; HAP, human activity profile; MMSE, Mini-Mental State Examination; SD, standard deviation; TG, training group.
Training effects on muscle strength are presented in Table 3. Greater plantar flexion PT at 60°/s was observed in the TG when compared with CG (P < 0.01; d = 0.69). After 12 training weeks, TG participants also had greater concentric and eccentric quadriceps PT at 180°/s (P = 0.02; d = 0.83 and d = 0.56, respectively), eccentric quadriceps PT at 60°/s (P = 0.01; d = 0.83), and ankle dorsiflexion (P = 0.04; d = 0.49) and plantar flexion (P < 0.01; d = 0.85) PT at 60°/s when compared with the pretraining evaluation.
We did not observe any significant difference between the CG and TG during the experimental period for quadriceps CSA, IMNCT (Table 2), or MQ (Table 4).
Quadriceps Cross-Sectional Area and Intramuscular Noncontractile Tissue
Results: mean ± SD.
Δ, Delta score (post-test data minus pretest data); CSA, cross-sectional area; IMNCT, intramuscular noncontractile tissue; Q, quadriceps muscle.
Concentric and Eccentric Peak Torque Values of Knee Extensors, Ankle Dorsiflexors, and Plantar Flexors
Results: mean ± SD.
Different from TG baseline.
Group versus time interaction (ANCOVA).
CON, concentric; ECC, eccentric; PT, peak torque.
Quadriceps Muscle Quality
Results: mean ± SD.
MQ, muscle quality (peak torque/quadriceps total CSA).
Discussion
The aim of this study was to evaluate MQ, that is, muscle strength per unit of muscle CSA, after a 12-week dance program. The main findings of this study showed an increase in muscle strength and maintenance of CSA without change in IMNCT, which is a positive therapeutic factor to be considered, suggesting that the virtual dance training protocol is capable of maintaining MQ in moderately active older women.
Another study found a decrease in intramuscular adipose tissue and increase in quadriceps CSA after a 12-week aerobic exercise training in sedentary, nonobese older people. In the present study, participants were moderately active and classified as overweight; these findings suggest that sedentary individuals experience more short-term benefits than those who are moderately active. 32
Delmonico et al. 2 further explained that even if muscle mass increases or remains the same, the decline in muscle strength related to aging cannot be prevented. In the current study, we observed only an increase in muscle strength, without any CSA modification, after 12 weeks of training. The lack of changes in MQ may be attributed to the maintenance of quadriceps CSA and muscle strength. Gains in strength without hypertrophy observed in early phases of a training protocol are a result of neural adaptations. 33 Thus, the gain in plantar flexor strength was probably due to neural increments, as a result of an increment of motor unit recruitment and type II fiber activation, and not due to an increase in muscle mass. However, in the present study, electromyographic activity was not assessed.
Studies reported the effects of moderate and vigorous intensity of a 12-week exergame training program. A recent study found an increase in peak torque at 180°/s of knee extensors, knee flexors, and plantar flexors in both groups. 34 In the present study, the training intensity was light to moderate, and we found an increase (17.6%) in the plantar flexor at 60°/s compared with CG. In addition, there was a main time effect in the TG for quadriceps muscle torque and ankle dorsi and plantar flexion PT.
The increase in the lower limb torque, even without external load, may be related to the training progression, which was achieved by adding a mat, that is, participants started dancing on an unstable mat, after the seventh week to increase the complexity of movements. The literature indicates that unstable platforms can stimulate proprioceptive and neural adaptations since muscle tension increases to maintain body balance.35,36 Research reported that training on unstable surfaces can provide greater neural activation of the lower limb muscles and reduce the time to start activation, which could contribute to an increase in muscle strength.36–38
According to Laroche et al., 39 older adults present greater antagonist activation, which might explain the increase in the eccentric torque of quadriceps muscles in the TG since the progression of exercises included squats. Cepeda et al. 40 emphasize that dancing requires a large number of concentric and eccentric contractions, a large number of changes in direction (imposed by the choreography), and a position of semiflexion of the knee.
The large increases in the plantar flexion peak torque can be due to the movements on tiptoes and small jumps performed by the older women while dancing. In addition, the movements were performed on an unstable surface (mat). According to Rossi et al., 38 muscle torque is generated from many joints, mainly the ankle joints, to compensate for large center of mass movements and unpredictable perturbations of balance.
In a 12-year longitudinal study of older women, torque decreased by 24.8% for the plantar flexors and by 3.3% for dorsiflexors. The different values were attributed to muscle architecture. 41 Thus, the hypothesis is that dorsiflexors are less responsive to the aging process and perhaps to physical training as well since in the present study, the plantar flexor torque increased by 17.6%, whereas 6.9% change was observed in the dorsiflexor torque. Eccentric stimulation of the quadriceps while dancing may have contributed to the increase in eccentric torque of quadriceps. Eccentric actions increase the fascicle length more than concentric actions, favoring the increase of eccentric torque. 42
In the same way, researchers who have conducted studies, including physical training with virtual games, for older people observed an increase in muscle strength.18,19 Kim et al. 19 investigated the effects of Xbox training (three times per week for 8 weeks) in older adults, using movements derived from Tai Chi and Yoga. Their evaluation of the maximal voluntary isometric force of hip flexors using a multimodal dynamometer showed that the strength of hip flexors increased by 29.9%. Jorgensen et al. 18 found a higher maximal voluntary contraction strength (18%) of leg extensors among community-dwelling, older adult participants (68% females) who undertook Nintendo® Wii™ training for 10 weeks. In the same way, Gschwind et al. 43 reported a 20% increase in quadriceps strength in older adults after physical training with virtual games, three balance exergames and five strength exercises using ankle cuff weights progressing from 1 to 3 kg. The individuals were encouraged to undertake 60 minutes of strength training and 120 minutes of balance training per week, for 16 weeks, without supervision.
The different gains in quadriceps muscle torque (29.9%, 18%, and 20%) found in those studies18,19,43 compared with our study (7.9% and 6.2% in eccentric and concentric at 180°/s, respectively; and 8.9% in eccentric at 60°/s) can be at least partly attributed to gender since they had mixed-sex samples, while in the current study, we evaluated only older women. According to Cooper et al., 44 changes in the musculoskeletal system are more prominent in middle-aged and older women than in men due to the postmenopausal effects of the decrease in female hormones, which may be the reason for the present findings in muscle strength. In addition, the gain in muscle strength reported in the study by Gschwind et al. 43 may be related to the use of additional load in the training and its longer duration (16 weeks).
Limitations of the study
This study evaluated a highly homogeneous sample of community-dwelling, physically independent older women. The different effects of the aging process on the musculoskeletal system and muscle loss between men and women must be taken into account when interpreting our findings. Thus, extrapolation of the outcomes to other samples such as institutionalized older women and/or men must be done with caution. Future studies are recommended to compare the effects of exergaming on MQ between the sexes. Other limitations of this study are the absence of sample randomization and blinded evaluators.
Conclusion
The dance program with virtual games, performed three times per week for 12 weeks, even without adding load, was enough to increase quadriceps and ankle plantar flexor strength without changing IMNCT and MQ of community-dwelling older women.
Regarding clinical applicability, supervised physical dance training with virtual games should be recommended as a strategy to increase the lower limb force important for functional independence and to prevent falls in older adults.
Footnotes
Authors' Contributions
All authors made substantial contributions to the conception or design of the work; acquisition, analysis, or interpretation of data; drafting the work or critically revising it for important intellectual content; and final approval of the version to be published. The authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors would like to thank the Federal Institute of Paraná (IFPR) and the Brazilian National Research Council (CNPq) for the support to the project coordinated by E.V.R. (CNPq/467987/2014-9) and for the financial support to A.R.S.G. (306179/2016-4). The authors would also like to thank the Clinical Hospital of the Federal University of Paraná (UFPR); the Sector of Legal Sciences of UFPR; the Department of Broadcasting of IFPR for providing rooms for the assessments and training; Professor André L.F. Rodacki (Center of Motor Behavior Studies of UFPR) for the equipment Biodex 4; Dr. André Francisco Gomes (DAPI) for the NMR and Professor Tânia Salvini and Christiane L. Prado-Medeiros (Federal University of São Carlos, UFSCAR) for technical support with the CSA method; the biologist and laboratory technician of the Pontifical Catholic University of Paraná (PUCPR), Seigo Nagashima, and Hilana Rickli Fiuza Martins (UFPR) for assistance with the Image Pro-plus software; Prof. Dr. Vitor Last Pintarelli (UFPR) for carrying out the clinical assessments of the older women; the undergraduate students of the research group (UFPR) for their support during the intervention and assessments, and all the older women who participated in the study. Finally, the authors would like to thank Professors Maria Eliana M. Schieferdecker and Estela Iraci Rabito of the Department of Nutrition of UFPR for their collaboration in this project and the Academic Publishing Advisory Center (![]() ) of the Federal University of Paraná for assistance with English language editing.
) of the Federal University of Paraná for assistance with English language editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financed, in part, by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior–Brasil (CAPES)–Finance Code 001.