
Abstract
Objective:
Modern board and card game-based cognitive interventions and gamification practices showed effectiveness in boosting executive functions and decreasing behavioral problems in children. However, the combination of both game-based methods has not been tested. Therefore, the main aim of this study was to test the effectiveness of gamification in modern board and card game-based cognitive interventions in Spanish schoolchildren at risk of social exclusion.
Materials and Methods:
In this multicenter single-blind study with a quasi-experimental design, 176 schoolers (6–13 years old) were assigned to a gamified group (with a narrative context and a rewarding system) and 107 to a nongamified group (with no narrative context or rewarding system). The interventions were implemented in regular classes. Behavioral executive dysfunction was assessed using the Behavior Rating Inventory of Executive Function, Second Revision (BRIEF-2) (Teacher form), pre- and postintervention.
Results:
We found significant time effects in all BRIEF-2 domains with small and medium effect sizes (d = −0.35 to d = −0.62). The nongamified group showed significantly higher decreases in all measures than those who used gamification.
Conclusions:
It is possible that playing for the joy of playing in the nongamified group was enough motivation to focus on the task, while adding gamification elements did not favor greater effectiveness of the program.
Introduction
According to European standards, 1 people with incomes below 60% of the national median equivalent household income, or with several deprivations, or low work intensity could be regarded as at risk of poverty or social exclusion. This condition is rising in Europe, especially in children. 1 The social exclusion condition has several psychological consequences relevant to child development. Children at risk of poverty or social exclusion are more likely to suffer mental health problems 2 and show hampered intellectual development.3,4 Studying how to intervene to prevent the detrimental effects of social exclusion conditions should be a priority issue.
Regarding intellectual or cognitive development, Haft and Hoeft 4 considered executive functions to be cognitive processes deeply affected by the condition of social exclusion. Executive functions allow us to control, direct, and coordinate other cognitive processes to complete the objectives and tasks required. 5 Some authors attempted to classify executive functions and proposed that executive functions could be cool or hot.6–8 Cool executive functions are activated in decontextualized situations, while hot executive functions are engaged when emotional and motivational elements could influence our behaviors. 9
Therefore, executive functions imply regulation at the cognitive level and refer to the control and regulation of emotional responses and behaviors too. 10 In childhood, preserved executive functions are predictors of better academic achievement, quality of life, and health, while executive dysfunction is related to many disorders, especially in children and adolescents.6,11,12 Hence, stimulation of executive functions in children at risk of social exclusion may imply some benefits in their lives.3,13
Cognitive training consists of repetitive performance of a set of standardized and systematic tasks that are designed to improve or maintain a set of cognitive functions that have been trained and other related tasks that have not been specifically trained.14–16 Board games allow us to perform these tasks using a playful approach. Playing while performing cognitive tasks could be more motivating because it activates the brain's reward system.17,18 Hence, from a psychobiological perspective, including game elements in cognitive interventions aimed at children at risk of social exclusion could be beneficial.
Some studies have found that experts playing traditional board games, such as chess or shogi, demonstrated better cognitive skills than amateur players or nongamers.19–25 Deliberate practice is needed to master them. 26 Besides, using traditional board games as cognitive training could improve some of the cognitive processes trained, showing a low to moderate near-transfer effect.27,28 Moreover, the use of traditional board games can modify brain structures. 29 Far-transfer effects have also been found, but with more inconsistent results with small effect sizes.30–32 Hence, some studies from different perspectives show that playing traditional board games helps develop cognitive benefits in children or adult populations.
Nowadays, board and card gaming experiences are not limited to traditional games. Compared with the traditional ones, modern board and card games33–35 (1) present more quantity, are newer, and have more diversity of mechanics; (2) are more esthetic and more thematic; and (3) some of them rely specifically on one cognitive process to play the game, similar to traditional psychological tests. These distinguishing characteristics should make modern board and card games more attractive to most people, including children. 36 Thus, modern board games should be an excellent way to intervene, especially in at-risk populations, because most games need social contact and promote prosocial behaviors and socialization. 37
Some studies have shown the efficacy of modern board and card games in cognitive training in older people38–42 and others in children.43,44 A modern board game-based intervention in children with attention-deficit/hyperactivity disorder resulted in linguistic short-term memory improvements in the experimental group compared with a wait-list group. 44 Moreover, children who played showed fewer behavior problems than children who did not play. 44
Thus, besides cognitive enhancement, modern board games have been associated with behavior improvements that could be significant in children at risk of social exclusion. These games could not be considered serious games. Designers create serious games with two goals in mind 45 : to entertain and to achieve an educational/health goal. All the studies mentioned above38–44 used board games for players to have fun. Therefore, games designed with no therapeutic/learning intention seem to be effective in diminishing executive dysfunction and related behavioral outcomes.
Some researchers showed that gamifying cognitive interventions focused on executive functions could improve the program's effectiveness.46,47 Gamification is known as the use of game elements in a nongame context.48,49 Gamification could effectively improve learning outcomes in children through the involvement of key brain regions related to engaging in any task, resulting in greater motivation and adherence to the program.49–51
Both playful methodologies (board and card games and gamification) seem to increase the motivation of participants, escalating their interaction with the learning environment, to finally modify behavior and cognition.52,53 However, as far as we know, no previous study has tested whether gamification could enhance the effects of a cognitive intervention based on modern board and card games. Combining two playful experiences would be better than applying only one.
Thus, the study's main objective was to test the effectiveness of adding gamification elements, such as narrative and rewarding systems, to a cognitive intervention based on modern board games to reduce difficulties in executive function behaviors (executive dysfunction) in school-age children at risk of social exclusion. We developed the research with two groups that carried out the same intervention with commercialized modern board games, one without gamification (experimental group) and the other without it (control group). Hence, the hypotheses of the present study were that (1) both groups would obtain lower scores in executive behavior dysfunctions after the intervention and (2) children in the gamified group would show a greater decrease in executive dysfunctions than those in the nongamified group.
Methods
Overview
The present study was interprofessional. The research team collaborated with a socio-community association led by the second author, who usually works with people at risk of social exclusion. The second author and four schools agreed to perform a modern board and card game school intervention in their classes. They decided to gamify the board and card game intervention only in two schools. The other two schools implemented the board and card game intervention without any kind of gamification.
Students who attended the four schools came from neighborhoods that met standard criteria of risk of social exclusion: elevated unemployment rates, school dropouts, and deficits in housing and public spaces.1,54,55 Then, the research team was contacted. As the intervention procedure was decided before the research team joined, a randomization procedure was not possible. Therefore, the present study was a natural experiment 56 with a multicenter, single-blind quasi-experimental design.57,58 Other gamification studies in the classroom have used this kind of experimental method. 59
Participants
A total of 339 school-age children were recruited from the four schools. However, the final analyses were performed on 283 participants (Fig. 1). Children were between the ages of 6 and 13 (mean = 8.93, standard deviation = 1.90, and 48.1% female) and primary education students (from first to sixth grade). The main inclusion criterion was attending one of the four schools implied in the research. The study's exclusion criteria were (1) families not signing the informed consent and (2) children showing linguistic problems in following instructions of the games. No participant met the exclusion criteria. The allocation for both groups of schools can be seen in Figure 1.
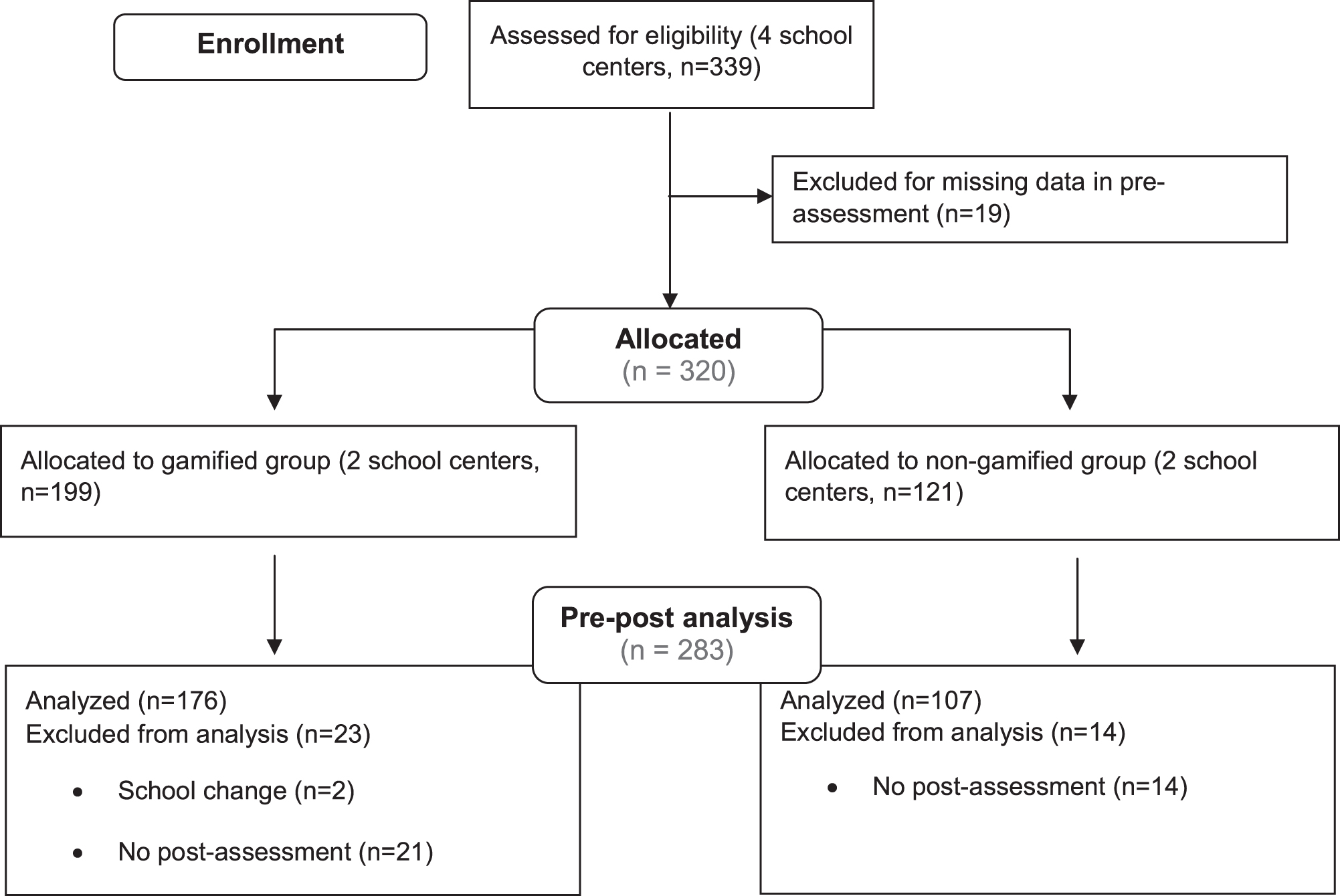
Flowchart. Note: we allocated the schools, not the participants.
We did not calculate the sample size because it was a natural experiment.
Outcome measures
Traditionally, executive functioning has been assessed using performance-based measures, although behavior-based measures have been developed. 60 Behavior-based measures seem to be helpful in recording the real difficulties of children in their environment. 61 Some studies have found that behavior-based measures of executive dysfunction are better predictors of conduct and disruptive problems than performance-based measures.17,62,63
In the present study, executive dysfunction was assessed with the Spanish version of the behavior-based measure, Behavior Rating Inventory of Executive Function, Second Revision (BRIEF-210,64) Teacher form. The research team selected the Teacher form because previous studies found that the correlations between BRIEF-2's scales and performance-based measures of executive functions were stronger compared with the Parent form. 61 The BRIEF-2 Teacher form comprises nine scales. The scales are classified into three indexes to measure the behavioral manifestations of executive functions (behavior regulation, emotion regulation, and cognitive regulation), a global executive composite, and three validity scales (infrequency, negativity, and inconsistency).
Behavior regulation provides information about the child's degree of difficulty in regulating and effectively monitoring behaviors and comprises the inhibition and self-supervision scales. Emotion regulation measures the child's degree of difficulty in regulating emotional responses, especially in changing situations, and comprises the flexibility and emotional control scales. Cognitive regulation assesses the degree of difficulty of the child to control and manage cognitive processes and solve problems effectively, comprising the initiative, work memory, planning and organization, task supervision, and organization of materials scales.
All factors must be interpreted in the same way: the higher the scores, the greater the deficits in that executive function behavior. The scale measure of the answers consisted of 3 Likert points (from 1 never to 3 frequent). We used both raw and transformed scores (T scores) to perform the analyses. T scores allowed the evaluated child to be compared with a normative sample of the general population of the same age and sex. Previous studies have found good validity and reliability scores of this measure.10,64
To assess the teacher's adherence to the intervention, we designed an ad hoc 3-item scale about the game sessions and the teacher's guide along with each session. The three questions were “Did the teacher use worksheets following the instructions?” “Did the game sessions follow the same structure?” “In general, did the teacher adhere to the implementation of the intervention?” These were answered by monitors from the local socio-community care association that helped teachers during the research. The answers were measured using a 4-point Likert scale, from 1 none/never to 4 hard/always.
We performed psychometric analyses to test its validity and reliability within the same data. Factor analysis showed that only one factor was retained according to the Kaiser criteria. The factor was labeled as teacher's adherence. Saturation ranged from 0.94 to 0.97. The scale showed a good reliability value (Cronbach's α = 0.95).
Intervention
Both interventions lasted from March 2019 to June 2019. Teachers performed a one-hour cognitive intervention session with the modern board and card games every week with their students (four players per game). The 2 groups played the same 12 different modern board games. Participants played each game three times. Several games were expected to train the same executive functions (Supplementary Data). To improve cognitive intervention effects, 6 we stepped the games according to their difficulty and duration (shorter games first). We explain the games in Supplementary Table S1.
Teachers guided the training with three worksheets that raised questions about the gaming experience in both groups. The worksheets (1) helped students to focus their attention on the task before setting up each game; (2) facilitated participants to resolve a complex task autonomously; and (3) promoted students’ reflection about their behavior and emotions during the game session.
The gamified group used a gamified scoring system. Each score was linked to a different badge with esthetics related to the world of board and card games. When students increased their scores, they received a better badge because of their higher level. They could improve their scores by using the worksheets in the game sessions, explaining a game to another group in the same class, explaining a game to students of another course, and participating in board and card game competitions. The gamified intervention also included a fantastic narrative. In contrast, students in the nongamified group played the same games without any narrative or reward.
Procedure
The flowchart of the study can be seen in Supplementary Figure S1. The present study was carried out following the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. All the methodologies were approved (code CEIC-2063) by the Clinical Research Ethics Committee associated with the University of Lleida and were strictly followed by the research team.
In February, the teachers of all school centers received the same 4–5 hours of training about neuroeducation and how to apply the board and card games to homogenize the intervention. Teachers from the gamified group also received specific resources from the socio-community care association that coordinated the project to provide a fantastic narrative and reward system that will playfully contextualize the program. The teachers of each course were responsible for collecting the informed consent from families.
In the preassessment, teachers registered some sociodemographic data and completed the BRIEF-2 Teacher form. The evaluation phase of the preintervention study was carried out from February to March 2019. After the evaluation, teachers implemented the intervention in regular classes (1 hour per week) from March to June 2019, aided by monitors of the local socio-community care association and coordinated by the second author. When the board and card game-based training was finished, the same teachers reassessed the executive function behaviors after the intervention. Finally, the monitors who observed and occasionally helped teachers in their performance of the game sessions evaluated teacher adherence to application of the cognitive intervention.
Statistical analysis
We analyzed baseline equality using the chi-squared test for categorical variables and independent t-test for continuous variables. We tested differences between the gamified group and nongamified group with a mixed-model analysis. The within-subjects factor was the phase of the study (time of assessment: pretest and post-test). The between-subjects factor was the training condition (gamified or nongamified) to assess intervention effects.
We controlled variables that could influence these results (teacher adherence to the intervention, the validity scales of BRIEF-2, and age). In the mixed-model analysis, we also assigned identification code (Id) and school as clusters (Random coefficients: Intercept | id, Intercept | school). We used the d-value for effect size calculation.65,66 Bonferroni correction was applied to reduce type 1 error in multiple testing. To prove the robustness of the intervention effects, we performed a sensitivity analysis (intention to treat), controlling missing data. We filled the missing values in post-assessment with their pre-assessment results (simple imputation method), and we compared these results with results obtained from the complete-case analysis.67–69 Moreover, to assess clinical improvement after the game-based interventions, we also analyzed the T scores obtained before and after the intervention in both groups for the BRIEF-2 clinical criteria to get percentages of improvement (unchanged and deteriorated after interventions).
Results
Intervention compliance and attrition analysis
Nineteen participants were excluded during the pre-assessment because of missing data. The percentage of excluded participants was similar in both groups [χ 2 (1,339) = 1.02, P = 0.32].
We found no differences between groups in the participants who dropped out [χ 2 (1,320) = 0.00, P = 0.99]. The sample of students who participated in the complete study was similar in age and gender to those who dropped out [tage(55.22) = 0.26, P = 0.79, d = 0.04; and χ2 age(1,320) = 0.47, P = 0.49]. However, we found significant differences in teachers’ adherence to program implementation [t(39.28) = −4.67, P = 0.00, d = 0.96]. Participants who did not finish the experiment had a teacher who showed lower adherence to implementation of the intervention compared with participants who completed the experiment.
Pretest comparison
As shown in Table 1, we found some significant differences between groups in executive function behaviors.
Demographic Characteristics and Baseline Outcome Levels of the Sample According to the Experimental Condition
Bold indicates significant results.
Higher scores are interpreted as higher executive dysfunction.
M, mean; SD, standard deviation.
Pre–post comparisons
We found significant within-subjects effects (time) in all executive function behaviors with small and medium effect sizes (Table 2).
Mixed Model Analysis of Pre–Post Comparisons from the Behavior Rating Inventory of Executive Function, Second Revision
Pre–post comparison in behavioral executive dysfunction measures.
Note: Means and SEs are after controlling the effects of BRIEF's validity scales, age, and teacher's adherence to the intervention. *P < 0.05; **P ≤ 0.01; and ***P < 0.001; 0.2 < d < 0.4 = small effect size; 0.5 < d < 0.7 = medium effect size; d > 0.8 = large effect size.
Higher scores are interpreted as higher executive dysfunction.
BRIEF-2, Behavior Rating Inventory of Executive Function, Second Revision; SE, standard error.
Regarding the between-subjects effect, we only found significant results by group for emotional control [Femotional control(1,276) = 6.77, P = 0.01, d = −0.33]. The nongamified group showed lower scores than the gamified group with a small effect size.
The group and time interactions revealed significant results in all executive function behaviors [from Fself-monitor(1,281) = 18.95, P = 0.00, d = −0.53; to Fcognitive regulation index(1,281) = 79.40, P = 0.00, d = −0.77]. We found greater decreases after the intervention in the nongamified group than in the gamified group, with medium (11 of 13 variables) and large effect sizes (2 of 13 variables; Table 2). All results remained significant after Bonferroni correction (See Figure 2).

Panel
Sensitivity analysis (intention to treat) of missing data using a simple imputation method reproduced the same result pattern obtained in the pre–post comparison from complete cases. We only found differences between the main analysis and sensitivity analysis in emotional control. The main results showed a significant group interaction in emotional control, but sensitivity analysis did not find this significance. Hence, the results found could be considered robust (Supplementary Table S2).
We replicated the analyses with T scores to focus on the BRIEF-2 clinical criteria (Table 3). In line with previous results, we found significant interactions between group and clinical changes in all measures (from x2self-monitor = 7.53, P < 0.05; to x2cognitive regulation index = 34.88, P = 0.00). The percentage of improvement represents those participants whose preintervention scores were potentially clinical (T > 64) or slightly elevated (T > 59) and slightly elevated or normal (T < 59) after the intervention. The nongamified group showed a higher percentage of clinical improvement than the gamified group on all scales.
Rates of Clinical Improvement from Pre- to Post-assessments for the Behavior Rating Inventory of Executive Function, Second Revision
P < 0.05; **P ≤ 0.01; and ***P < 0.001.
Higher scores are interpreted as higher executive dysfunction.
Discussion
The purpose of this study was to test the effect of gamification in a cognitive school intervention with modern board and card games to improve behavioral, real-world executive functioning in children at risk of social exclusion. As we hypothesized, the results showed significantly reduced behavioral problems associated with executive functions from the preintervention phase to the postintervention stage.
However, these reductions were mainly explained by results of the nongamified group. These results were interpreted as far transfer 16 from game performance tasks to their executive function behaviors, although to generalize these results, it would be convenient to have performance measures to know what near and far transfers may result from this type of intervention.
Nevertheless, the gamified group benefited less from the intervention than the nongamified group. Hence, our second hypothesis was rejected. It is possible that adding more guiding elements to the game could be seen by students as an imposition instead of an extra reward. Previous studies recommended that adults have to avoid an authority position, and it is suggested that they should offer the freedom of action to the child. 70 Thus, as children were already playing modern board and card games, adding more gaming elements through gamification could make children feel that adults were restricting the experience of the pleasure of playing.
These results align with past studies, which pointed out that children who expected a tangible prize when they played showed significant decreases in their intrinsic learning motivation.71,72 Therefore, effective game-based learning implies maintaining children's freedom, curiosity, and natural enjoyment in playing to learn from their interests. 70
However, some alternative explanations could be proposed. First, the game elements used in the gamified group might not be adequate for this sample. Past studies pointed out that the use of scoring systems could be related to a decrease in the free-choice behavior, considered by some subjects as the less exciting characteristic of the games. 73 Future studies must address game elements that could be better when using board and card game interventions and gamification. Furthermore, psychological (e.g., temperament 74 ) or external factors (e.g., changes in teaching staff and differences in executive function levels within the playgroup) could have influenced the results.
Limitations and future directions
One relevant limitation of the study is that it has been carried out as a natural experiment with a pseudo-experimental methodology without randomization. This type of assignment could cause the appearance of differences in the baseline characteristics between the intervention groups. However, the different statistical analyses performed pointed to the robustness of the results. Moreover, the lack of a passive control group limits the findings due to maturation.
We also assessed executive dysfunction with a behavior-based scale. Performance tasks and behavior-based measures of executive functions could assess different underlying mental constructs. 60 Future studies could include performance tasks in addition to behavioral ones.
Future studies could also assess possible transfer from the cognitive intervention to other personal, educative, and social variables. For example, truancy is a critical educational obstacle in the schools where the study was performed. Socioeconomic difficulties could be a risk factor that could explain this absenteeism.75–77 In this line, executive functions have also been related to specific academic skills such as mathematics and reading.5,78–81 Future studies could assess possible far transfer to these abilities.
Clinical and educational implications
Before the game-based intervention, both groups showed T scores with clinical significance in much of the behavioral executive dysfunction domains. As expected,3,13 participants seemed to have difficulties in executive behaviors that have been associated with a situation of risk of social exclusion. These deficits decreased after the intervention with modern board games, especially in the nongamified group. Results suggest that implementing a modern board and card game cognitive school intervention could alleviate clinical problems in behavioral executive functions to reach normative scores in children at risk of social exclusion.
Effect sizes obtained in all behavioral executive dysfunctions after the game school intervention in both groups (except emotional control) could be considered as desired effects from an educational intervention in a real school context (d > 0.4). 82 Therefore, it is very likely that the present intervention has led to tangible benefits beyond the own normative development of children and the effects of teachers themselves in a real school context. 82
Conclusions
A modern board and card game-based cognitive school intervention seems to effectively reduce problems in behavioral executive functions in children at risk of social exclusion. The reduction of behavioral executive dysfunction was quantitative and qualitative because we found changes with clinical significance. Moreover, children who played without gamification elements showed further decreases in deficits in executive function behaviors than the gamified group. Playing for the pleasure of playing could be by itself a sufficient reason for enjoyment and effort in the task.
Any underlying research materials related to the present article (e.g., data) can be accessed under request.
Footnotes
Author Disclosure Statement
This work is part of an Industrial Doctorate with Mercurio Distribuciones, supported by the Plan of Industrial Doctorates of the Secretariat of Universities and Research of the Department of Business and Knowledge of the Generalitat de Catalunya, the Comissionat per a Universitats i Recerca del DIUE. The authors received financial and resource support from Mercurio Distribuciones (board and card games editorial). Mercurio Distribuciones provided the board and card games used in cognitive interventions.
The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Funding Information
This work was supported by the Plan of Industrial Doctorates of the Secretariat of Universities and Research of the Department of Business and Knowledge of the Generalitat de Catalunya, the Comissionat per a Universitats i Recerca del DIUE; the Agència de Gestió d'Ajuts Universitaris i de Recerca de la Generalitat de Catalunya (2017SGR1577); the Center for Biomedical Research Network on Mental Health (CIBERSAM), Instituto de Salud Carlos III; and the Spanish Ministry of Science, Innovation and Universities (MICIU/FEDER; project RTI2018-099800-B-I00).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.