
Abstract
Studies have shown that leisure activities, such as tabletop games, not only increase social interactions and reduce depression among older adults, but also help improve their cognitive function. However, the effects of tabletop games on cognition in older adults are yet to be comprehensively analyzed. The purpose of this study was to review and examine the effects of tabletop games on cognition in older adults. This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Articles were searched in seven electronic databases from their inception to December 2020. A total of 3946 studies were retrieved, among which 11 studies were systematically reviewed and 10 were meta-analyzed. In older adults with intact cognition, tabletop games had positive effects on their global cognition (standardized mean differences [SMD] = 1.36, 95% confidence intervals [CI]: 0.37–2.34, P < 0.001) and executive function (SMD = 0.47, 95% CI: 0.12–0.83, P < 0.001). In older adults with cognitive impairment, significant differences were found in global cognition (SMD = 0.53, 95% CI: 0.09–0.98, P = 0.02). Tabletop games had the characteristics of cognitive training and interpersonal interactions. After receiving tabletop game interventions, the cognitive functioning in older adults with intact cognition and those with mild cognitive impairment or dementia was improved. For older adults, in addition to improving cognitive functioning, tabletop games also increased their social participation and interactions.
Systematic Review Registration:
This review has been registered in the PROSPERO (CRD42021254085).
Introduction
The older population accounted for 13.5% of the world's total population in 2021. 1 It was estimated that the older population will account for 16% of the total population in the world by 2050, 2 indicating that the world population is rapidly aging. When aging, physical functions, memory, and cognitive functions decline. 3 Because of the enormous financial and human cost of decline in cognitive processes on the individuals, families, and societies, nonpharmacological preventions such as tabletop game playing are gaining increasing attention to prevent, delay, or improve cognitive decline, which leads to better performance in the activities of daily living.4,5
Cognitive training is often customized for specific tasks; it is difficult for people who are not interested or have insufficient resources to participate. 6 Previous studies showed that leisure activities, such as gardening, art activities, and playing tabletop games, not only increase social interactions and reduce depression in older adults but also improve their cognitive functions.7,8 For example, playing tabletop games involves not only understanding rules of the game but also interpersonal interactions, which evolves intellectual stimulation leading to improvement in cognitive functions.6,9,10 Tabletop games, one of cognitive leisure activities, 6 are usually played on a table without other electronic equipment. 4 Some tabletop games are played on a board, such as Go game or chess, by following rules to move game pieces. 11 Others can be played without a board such as Mahjong and card games.6,12
Some tabletop games can be played with many players, and others can be played with a single player. 13 Because of its competitive nature and the requirement of using skills of concentration, memory, verbal fluency, planning, and calculation to reactive neural circuits in an aged brain, tabletop game playing as cognitive stimulation is effective in improving cognitive functions and interpersonal interactions.4,14
Recently, more and more studies have examined the impacts of tabletop games on cognitive functions in older adults.14–16 Although previous systematic reviews or cohort studies showed that leisure activities were beneficial to the cognition of older adults,7,8 the effects of tabletop games on cognition in older adults are yet to be comprehensively reviewed. The purpose of this study was to systematically review and examine the effects of tabletop games on global cognition and on domain-specific cognitive functions of attention, memory, executive function, and verbal fluency in older adults.
Materials and Methods
This review was reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement. 17
Data search and study selection
A literature search for studies published in peer-reviewed journals in the English or Chinese language was conducted using the electronic databases of Airiti Library, Cochrane Library (CENTRAL), Cumulative Index to Nursing and Allied Health Literature with Full Text, Embase, MEDLINE Complete, PubMed, and Web of Science. The date interval selected was from the inception of the databases to December 2020. The keywords and MeSH terms combined for the literature search were as follows: tabletop game (board game OR card game OR checkers OR chess OR Go game OR Mahjong OR Monopoly OR poker OR puzzle OR tabletop game), older adults (aged OR elder* OR geriatr* OR old OR older adult OR older people OR older person OR senior), and cognition (attention OR cognition OR cognitive function OR executive function OR memory OR verbal fluency).
A manual search of the reference list of studies that met final eligibility was performed to retrieve additional eligible studies.
The inclusion criteria were as follows: (1) the study sample involved adults with an average age of older than 65 years, (2) the study implemented tabletop games as an intervention, (3) the study assessed cognitive functions as outcomes, and (4) the study included pre/post comparative tests. The exclusion criteria were as follows: (1) abstracts, case reports, conference proceedings, nonpeer-reviewed studies, protocols, and review articles, and (2) studies involving tabletop games combined with other treatments as interventions.
Quality appraisal, data extraction, and data synthesis
Two reviewers independently screened the titles and abstracts to exclude ineligible studies. They then reviewed full texts of the remaining articles based on the inclusion and exclusion criteria. If consensus could not be reached after discussion, a third reviewer was consulted. Reasons for excluding studies were documented at each step (title, abstract, and full-text review) and presented in a flowchart that was created according to the PRISMA requirements. Data extraction was based on the standardized data extraction tools suggested by Cochrane Collaboration. 18 For each included study, information such as the author's name, year of publication, study design, number and characteristics of participants, measurements, interventions, and findings on cognition was extracted. All reviewers checked the correctness of the extracted data.
The methodological quality of each individual study was assessed using the Cochrane risk-of-bias tool for randomized trials version 2 (RoB 2.0) and Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I).19,20 The randomized controlled trials (RCTs) were rated as having low, some concerns, or high risk of bias for each criterion of the randomization process, deviations from protocol, missing outcome data, measurement of the outcome, and selective reporting. Non-RCTs were rated as having low, moderate, serious, or critical risk of bias for each criterion of confounding, participant selection, classification of interventions, deviations from intended interventions, missing data, outcome measurements, and selection of the reported result. If there were questions about the eligibility of the study, the corresponding author was contacted for further information.
Statistical analysis
The meta-analysis was conducted using Review Manager version 5.4 (Cochrane Collaboration, Oxford, United Kingdom). The evaluation for the degree of heterogeneity was conducted using Cochran's Q test and I2 statistics. 21 When Q < 0.1, it represents the existence of heterogeneity; when I2 = 25%, 50%, and 75%, it represents low, moderate, and high heterogeneity, respectively. 21 If the heterogeneity existed, the random-effects model was used; otherwise, the fixed-effects model was adopted. 21 Because all outcome parameters were continuous variables, the results were presented as mean differences with standard deviations as well as standardized mean differences (SMD) with 95% confidence intervals (CI). When the P-value was less than 0.05, it was considered a significant difference.
Sensitivity analyses were used to find the sources of heterogeneity by removing the study with the largest effect size. Because of the difference in populations (older adults with intact cognition and those with cognitive impairment), a subgroup analysis was conducted to detect the difference. Egger's regression test was performed in the Comprehensive Meta-Analysis version 2 (Biostat, Inc., Englewood, NJ) to assess publication bias across the studies. 22
Results
Identification of studies
A total of 3946 studies were identified. After removing the duplicates, 3248 studies were found to be relevant. Their titles and abstracts were checked and resulted in 83 full texts for eligibility screening. Finally, 11 studies were included in the systematic review, and 10 of them were included in the meta-analysis (Fig. 1).
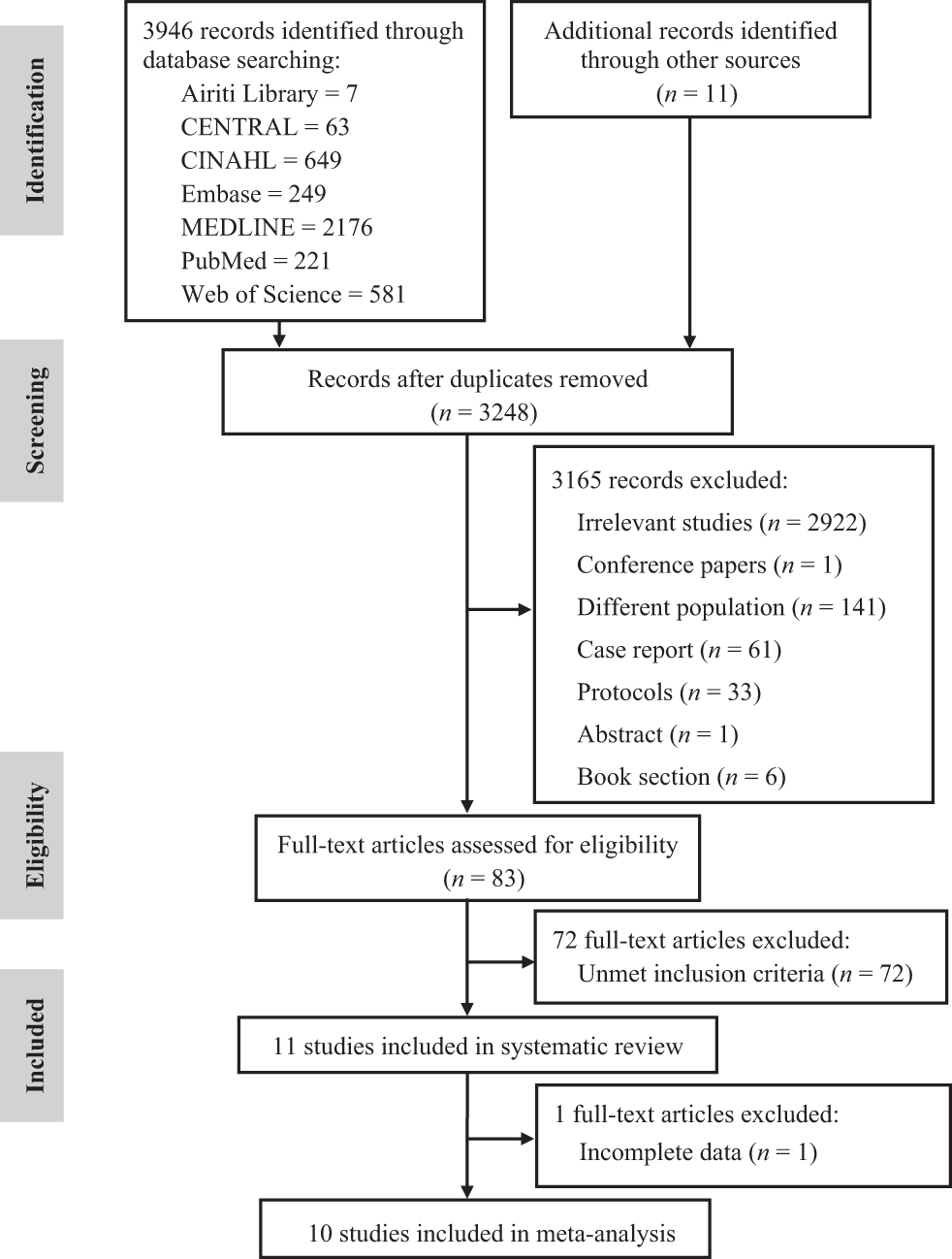
Article selection flow diagram.
Methodological quality of the studies
Among the 11 included articles, eight studies were RCTs and three were quasi-experimental (QE) studies. To assess methodological quality, the RoB 2.0 was used for RCTs and the ROBINS-I for QE studies. Most of the RCTs were considered having some concerns on overall risks (n = 6), one was considered having an overall low risk of bias, 14 and the other was considered having an overall high risk of bias. 23 All of the QE studies had an overall moderate risk of bias (Table 1).
Methodological Quality of the Included Studies
Cochrane risk-of-bias tool for randomized trials version 2 (RoB 2). Low, low risk of bias; High, high risk of bias.
Risk of bias in nonrandomized studies of interventions (ROBINS-I). Low, low risk of bias; Moderate, moderate risk of bias; Serious, serious risk of bias; Critical, critical risk of bias; NI, no information.
Sensitivity analysis and publication bias
The results of meta-analyses were presented within four cognitive outcomes: (1) global cognition, (2) executive function, (3) short-term and working memory, and (4) verbal fluency. After sensitivity analyses, the heterogeneity among the studies could not be ruled out. There was high heterogeneity in the outcome of global cognition (I 2 = 82%, P < 0.001) and moderate heterogeneity in the outcome of short-term and working memory (I 2 = 37%, P = 0.14). The results of Egger's test showed publication bias in the outcome of global cognition (P = 0.029). While differentiating older adults with intact cognition and those with cognitive impairment, the results of subgroup analyses showed that publication bias only occurred in studies involving older adults with intact cognition (P = 0.034).
Characteristics of studies and participants
Among the 11 articles included for the systematic review, three were QE studies4,15,24 and the others were RCTs (n = 8) (Table 2). The studies were published between 2014 and 2020, and they were conducted in the following countries: China,5,6 Indonesia, 15 Ireland, 25 Japan,10,16,26 Myanmar, 23 Spain, 14 and Taiwan.4,24 The minimum number of participants in these studies was 17 older adults 14 and the maximum was 110 older adults. 6 The mean age of the participants ranged from 67.8 ± 8.45 to 89.1 ± 5.4. 16 Among the 11 studies, four studies involved older adults with cognitive impairments,5,6,15,16 and the rest of the studies recruited older adults with intact cognition. Regarding the study settings, six studies were conducted in communities,10,15,23–26 four studies in long-term care facilities,5,6,14,16 and one study in a daycare center. 4 The majority of studies (n = 9) had more females than males, and two studies had more males than females15,23 (Table 2).
Characteristics of the Included Studies
5TSTS, 5 times sit to stand; A, active control; BBS, Berg Balance Scale; Borg CR-10, Borg Category Ratio scale; CBT, Corsi block-tapping test; CG, control group; COWAT, Controlled Oral Word Association Test; CPM, Raven's Coloured Progressive Matrices; CVFT, Category Verbal Fluency Test; FAQ, Functional Activities Questionnaire; FDT, Five-Digits Test; FES-I, Falls Efficacy Scale International; F-FDG-PET, Fluorine-18 fluorodeoxyglucose positron emission tomography; GDS-SF, Geriatric Depression Scale Short Form; HGS, hand grip strength; IG, intervention group; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; MoCA-B, Beijing version of the Montreal Cognitive Assessment; MoCA-Ina, Indonesian version of Montreal Cognitive Assessment; MoCA-J, Japanese version of the Montreal Cognitive Assessment; QE, quasi-experimental; RCT, randomized controlled trial; SF, semantic fluency; STT, Shape Trail Test; TMT, Trail Making Test; TUG, Timed Up and Go; TUG-cog, Timed Up and Go test Cognition; U, usual care; WAFF, Visual Focused Attention Test; WAIS-III, Wechsler Adult Intelligence Scale-third edition; WAIS-IV, Wechsler Adult Intelligence Scale-fourth edition; WHOQOL-Brief, World Health Organization Quality of Life Questionnaire-Brief version; WMS-III, Wechsler Memory Scale-third edition; WMS-R, Wechsler Memory Scale-Revised.
Tabletop game program features
Some studies used multiple tabletop games as interventions,4,14,23 and others used a single abstract strategy game: Mahjong,5,6,24 Go game,10,16,26 chess, 15 or a crossword puzzle. 25 Each intervention session ranged from 30 minutes 23 to 90 minutes4,14 with a mode of 60 minutes (n = 6). The frequency for implementing interventions ranged from once a week4,10,16,26 to seven times per week,15,25 with once a week (n = 4) and three times per week (n = 4) as the most frequent choices. The overall duration of the interventions ranged from 5 weeks 14 to 15 weeks, 16 with a mode of 12 weeks (n = 6) (Table 2).
Outcome variables and measurements
The scales used to measure cognitive functions were as follows: (1) Montreal Cognitive Assessment4,5,15,16,23 for global cognition, (2) Trail Making Test5,10,14 for executive function, (3) the digit span test from Wechsler Adult Intelligence Scale-III and Wechsler Memory Scales6,10,16,26 for short-term and working memory, and (4) verbal fluency tests from Controlled Oral Word Association Test6,10,25 for verbal fluency (Table 2).
Effects of tabletop games on cognition
Because the authors in 1 of the 11 studies 24 did not provide the required data, that study was not included in the meta-analysis. Among the 10 studies included in the meta-analysis, 8 studies were RCTs, and 2 were QE studies. Subgroup analyses were conducted by stratifying participants according to their cognitive conditions (intact cognition and cognitive impairment).
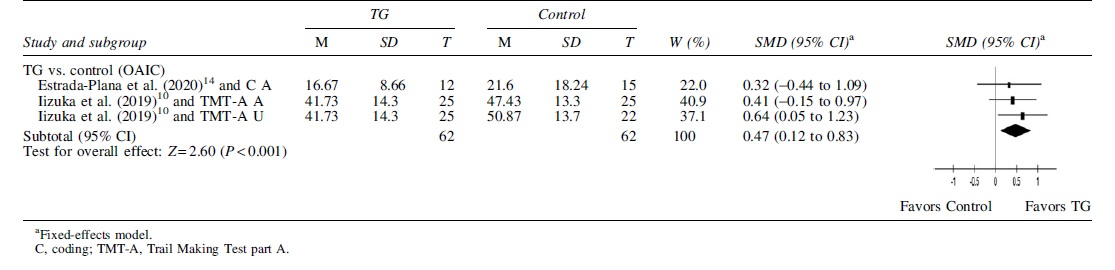
In older adults with intact cognition, tabletop games had positive effects on their global cognition (SMD = 1.36, 95% CI: 0.37–2.34, P < 0.001) (Table 3) and executive function (SMD = 0.47, 95% CI: 0.12–0.83, P < 0.001) (Table 4). In older adults with cognitive impairment, significant differences were found in global cognition (SMD = 0.53, 95% CI: 0.09–0.98, P = 0.02) (Table 3). No significant differences were found in short-term and working memory (Table 5) and verbal fluency (Table 6).
Effects of Tabletop Games on Global Cognition

Effects of Tabletop Games on Executive Function
Effects of Tabletop Games on Short-Term and Working Memory

Effects of Tabletop Games on Verbal Fluency

Discussion
On average, the tabletop game intervention period was 12 weeks, the frequency was one to three times a week, and each session was 60 minutes long in this review. Four of the included studies were conducted in long-term care facilities, and three of them involved older adults with cognitive impairment. After tabletop game interventions, the improvement of cognitive and executive functions in older adults living in long-term care facilities could be seen in these studies. Compared with community-dwelling older adults, older adults in long-term care facilities were usually prone to malnutrition, and cognitive and physical decline. 27
In addition to physical health, older adults in long-term care facilities also had problems such as depression and lack of social interactions. 28 The problem of sedentary lifestyles or lack of activity was also common in older adults living in long-term care facilities. 27 It is generally believed that sedentary lifestyles are not good for cognitive functioning; engaging in cognitive activities can help reduce the risk of dementia. 29 If sedentary lifestyles are unavoidable, tabletop games are an alternative intervention method for older adults in long-term care facilities.
The World Health Organization guidelines suggested cognitive training and social activities to help reduce the risk of cognitive decline and dementia. 30 Tabletop games have the characteristics of cognitive training and interpersonal interactions. 10 Playing tabletop games promotes exposure to taking initiatives, planning, and adaptation to winning or losing, which prevents cognitive decline or dementia. In addition, tabletop games can be played with family members or friends and they bring immediate pleasure to participants, which promotes social interaction. Therefore, compared with cognitive training, cognitive leisure activities such as playing tabletop games are usually pleasurable methods to preserve cognition and to prevent cognitive decline or dementia and they can arouse people's interest and participation. 6
Mahjong is a famous and popular social entertaining tabletop game in Asian countries, especially in Chinese communities.6,16 Besides the feature of entertainment, Mahjong also has cultural characteristics. 31 Many Chinese people have been exposed to Mahjong since childhood.31,32 In China, Mahjong is a symbol of friendship that friends are often invited to play Mahjong in the Chinese New Year.32,33 In the selection of tabletop games, the rules of Go game are simple and easy for a beginner to get started. 16 Because Mahjong has many rules and complex combinations and is played among four players, it may be difficult for a beginner. 16 In this review, some studies selected participants who have experience in playing Mahjong but had not played Mahjong in the past 3–6 months.5,6
Other studies chose a variety of tabletop games as interventions,4,14 with the level of difficulty in game rules ranging between Go game and Mahjong. As can be seen, if tabletop games with complex game rules are chosen, participants may need to have previous experience or seek for professional coaching. For tabletop games with simpler rules, prior experience may not be required. In line with previous studies,34,35 more and regular tabletop game playing was associated with higher cognitive functions, which triggered more human interaction and memory access leading to increased intellectual stimulation and cognitive development for older adults. 10
Improvements in global cognition were seen after tabletop game interventions in older adults with mild cognitive impairment or dementia in four of the included studies,5,6,16 suggesting that even older adults with declined cognition can learn and master the rules of tabletop games, thereby gaining improved cognitive functioning. 16 The meta-analysis results showed that tabletop game interventions could improve the global cognition of older adults regardless of their cognitive conditions. Unlike cognitive training, tabletop games are difficult to specify precisely which cognitive domain is to be trained, and so, a measure of overall cognitive function may be more appropriate. 6 The improvement in overall cognitive function by tabletop games may be related to cognitive reserve. 4
The cognitive reserve hypothesis is that dealing with complex and challenging issues and stimulated by life experiences and social activities could enhance cognition to maintain a relatively good cognitive function in aging and disease. 36 Executing tabletop games requires decision-making and social interaction skills, which in turn enhance cognitive reserve.4,10 The results of this systematic review and meta-analysis suggested that mental exercise in the form of playing tabletop games might increase cognitive function.
As for older adults with intact cognition, playing tabletop games improved executive functions. To win in a competition, participants need to concentrate and choose a strategy. These complex behaviors not only improve memory but also executive functions. 5 When participating in multiplayer games, interpersonal interactions are increased, which help enhance executive functions. 37 Moreover, the flexibility of hand functions is related to the executive function. 38 If the execution of tabletop games involves the flexibility of hand functions, it may also help improve the executive functions of older adults. 5
Relevance to clinical practice
Different types of tabletop games have different cognitive training effects. Most tabletop games are beneficial for improving global cognition and some competitive tabletop games may be better for improving executive function. Playing tabletop games requires concentration and ability of choosing game strategies. For the complex tabletop games, it is better that the players have relevant experience. Participating in multiplayer tabletop games enhances social interaction. Training skills of decision-making and social interaction increases cognitive reserve to maintain relatively good cognitive function, which has a positive effect on preventing cognitive impairment. Accordingly, older adults receiving cognitive stimulations by participating in multiplayer tabletop games and tabletop games with competitive components may improve their cognitive function. Whether older adults have a cognitive impairment or are living in long-term care facilities, tabletop games can be an intervention to improve their cognitive functioning.
Limitations
This review only included studies published in the English or Chinese language; therefore, information bias may occur. Some studies in the meta-analyses showed moderate to high heterogeneity, which may affect the interpretation of the results. Because some studies used a variety of tabletop games as the intervention, it may not be possible to confirm that the results are representative of the intervention benefits of each type of tabletop games. Furthermore, because most of the studies had a higher proportion of women than men, gender imbalance may lead to discrepancies in the results. Finally, publication bias was shown within the outcome of global cognition in older adults with intact cognition; therefore, this result must be interpreted with caution.
Conclusion
Most of the previous systematic reviews explored the relationship between leisure activities and cognition in older adults. This article is the first to discuss the effects of tabletop games on cognitive functioning in older adults. Tabletop games have the characteristics of cognitive training and interpersonal interaction enhancement. Compared with traditional cognitive training, tabletop games are more interesting and attract older adults to participate. Both older adults with intact cognition and those with mild cognitive impairment or dementia achieved cognitive improvements after receiving tabletop game interventions. Playing tabletop games can increase interpersonal interactions in addition to improving cognitive functions.
Footnotes
Authors' Contributions
All authors meet the criteria for authorship, have approved the final article, and all those entitled to authorship are listed as authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported partially by the Kaohsiung Medical University Research Center Grant (KMU-TC109B07). The funding source supported the study financially and was not involved in the study design, data collection, analysis and interpretation of data, writing of the report, and in the decision to submit the article for publication.