
Abstract
Objective:
Assess the effect of nonimmersive virtual reality (VR) training as complementary rehabilitation on body oscillation in children with cerebral palsy (CP) while standing on different bases of support and surfaces.
Materials and Methods:
Twenty-three children with unilateral CP randomly allocated to an intervention group (IG, n = 12) or control group (CG, n = 11). The IG underwent two weekly 50-minute sessions of VR training over 8 weeks, associated with conventional therapy, while the CG was submitted to two 45-minute sessions of conventional neurodevelopmental-based physiotherapy a week over the same time period. Participants were evaluated on a force platform under control conditions (CCs) (rigid surface, feet parallel); semitandem stance; flexible surface (FS) with feet parallel; and flexible surface in a semitandem (FSST) stance. The effect of the group and time factors on the center of pressure oscillation variables was analyzed by repeated-measures analysis of variance (ANOVA), with significance set at 0.05.
Results:
The main effect observed was for time on the FS, with a decline in the amplitude of mediolateral (ML Amp) (P = 0.01) and mediolateral root mean square (P = 0.01) after intervention. In the IG, ML Amp also declined after intervention under CCs (P = 0.02) and total velocity increased for FSST (P = 0.04). The percentage change was significant only in the IG.
Conclusion:
VR training as complementary rehabilitation can help improve body oscillation in children with CP and mild functional impairment. Nonimmersive VR can be considered a complementary tool for the physical rehabilitation of children with CP. This study was registered with the Brazilian Clinical Trials Registry (RBR-3zty4w).
Introduction
Children with cerebral palsy (CP) may exhibit postural control deficits, which can be defined as the skill required to maintain the alignment of body segments and body oscillation in semistatic postures or dynamic control of movements.1,2 The lower levels of postural control in this population are due to possible primary deficits in the visual, somatosensory, and vestibular systems. 3 This reduction in postural control impacts anticipatory postural adjustments, movement strategies with greater energy expenditure, and difficulties in maintaining balance in routine activities.4,5
These difficulties may be exacerbated in challenging conditions or settings6,7 such as different bases of support (BoS) 8 and support surfaces.9,10 Changes in the angle of orientation and positioning of the feet can generate postural instability, as the relationship between body segments and weight bearing on the lower limbs is modified. 8 The semitandem (ST) position, for example, is challenging as close positioning between the feet increases the demand for neuromuscular control to maintain body oscillation. 11 Different conditions of support surfaces, such as texture, density, and instability, can increase postural sway. 9 Thus, it is important to evaluate outcomes that reflect the possible different demands imposed on postural control.
Considering these deficits, especially under more complex conditions, sensory motor interventions have been proposed as a means of generating different postural demands and specific adaptive actions.12,13 Conventional therapy, consisting of strengthening, stretching, balance exercises, and principles of neurodevelopmental therapy, is one of the most used therapies in children with CP.5,14 Current literature demonstrates that regardless of the technique used, it is important that some principles are present in the treatment, such as goal-directed training, strengthening and mobility training, and task-specific training. 15
Virtual reality (VR) stands out as one of the main therapies that meet these principles.13,16,17 Nonimmersive VR therapy, in addition to being able to encompass the main principles of motor learning, stimulates physical and cognitive functions, with a high level of feedback and motivation. 18 Studies have demonstrated that VR training changes individuals' ability to perform functional activities and improves their balance.19,20 It can also help activate specific cortical areas such as the motor cortex, causing persistent hemodynamic changes even after completing virtual environment activities, which may be indicative of motor learning. 21
Although research has shown the positive effects of VR training on postural control and dynamic balance when evaluated using clinical scales, 17 few studies have investigated body oscillation using more precise methods, such as a force platform.22,23 Sajan et al. 23 found that although dynamic balance improved in children with CP after a VR intervention, center of pressure (CoP) oscillation velocity did not differ between the intervention and control groups. The authors postulated that the lack of change in body oscillation may have been due to the fact that the activities performed were less complex and primarily involved the upper extremities. Finally, Park et al. 22 observed significant differences in postural control after 4 weeks of VR-based rehabilitation. However, the treatment and assessments were conducted while participants were sitting, which requires different postural control mechanisms than those used when standing.
The abovementioned aspects raise the question of whether the effect of VR might be more evident in more specific complex activities that challenge body oscillation, such as different BoS stability conditions. This is based on the fact that functional and dynamic balances are trained during VR interventions 21 using multisensory stimuli, which cause the body to move in different directions at varying speeds, constantly challenging the limitations of the BoS. These limitations represent how much of the challenging activity a child can perform without falling. Thus, the aim of the present study was to assess the effect of nonimmersive VR training as complementary rehabilitation on body oscillation in children with unilateral Gross Motor Function Classification System (GMFCS) I CP while standing on different BoS and surfaces.
The decision to study a GMFCS I population is justified because although these individuals have the necessary motor skills to perform well at home, in school, and in their communities, they have a limited repertoire of movements that are typically uncoordinated and performed at slower speeds, 24 making them less physically active. 25 In addition, physiotherapy services for these children are generally limited, since they are believed to have reached a plateau in their gross motor skills. However, despite reaching a plateau, balance and coordination difficulties persist and may even deteriorate during adolescence, which justifies interventions with this population.26,27
The hypothesis of this study is that the multisensory stimuli provided by nonimmersive VR intervention will improve body oscillation, particularly under less stable conditions, such as adding foam to the BoS and changing the stance to ST.
Materials and Methods
Study design
This was a randomized controlled trial. The clinical protocol was in line with Consolidated Standards of Reporting Trials (CONSORT) recommendations 28 and registered with the Brazilian Clinical Trials Registry (http://apps.who.int/trialsearch/Trial2.aspx?TrialID=RBR-3zty4w).
The parents or legal guardians provided written informed consent, authorizing the children to take part in the experiment. The study was conducted in accordance with the current version of the Declaration of Helsinki and approved by the Human Research Ethics Committee of Federal University of Sao Carlos, Sao Carlos, Brazil (CAAE: 72770817.5.0000.5504 and protocol no. 2.353.422).
Randomization and blinding
The participants were randomly allocated to the groups (control or intervention) using a randomization list kept by a member of the research group who was not involved in any other stage of the study. Following initial assessments, the participants received and opened the sealed opaque envelopes indicating which group they had been assigned to. The assessor responsible for evaluating postural oscillations was blind to the participants' data and group allocation.
Participants
All participants were recruited from rehabilitation centers specializing in the treatment of children with disabilities, in the state of São Paulo (Brazil).
The sample size calculation was performed using the G-Power 3.1.5 software, and an effect size of 0.8 was considered with a power of 80%, and a significance of 5%, a priori. The sample size calculation resulted in 24 children (12/group). Twenty-three of the 49 children of both sexes invited to take part in the study agreed to participate and were randomly distributed to an intervention group (IG-11) and control group (CG-12). Both groups exhibited similar baseline demographic and clinical characteristics.
Greater details on the recruitment process are shown in the flowchart of the different stages of the study (Fig. 1).
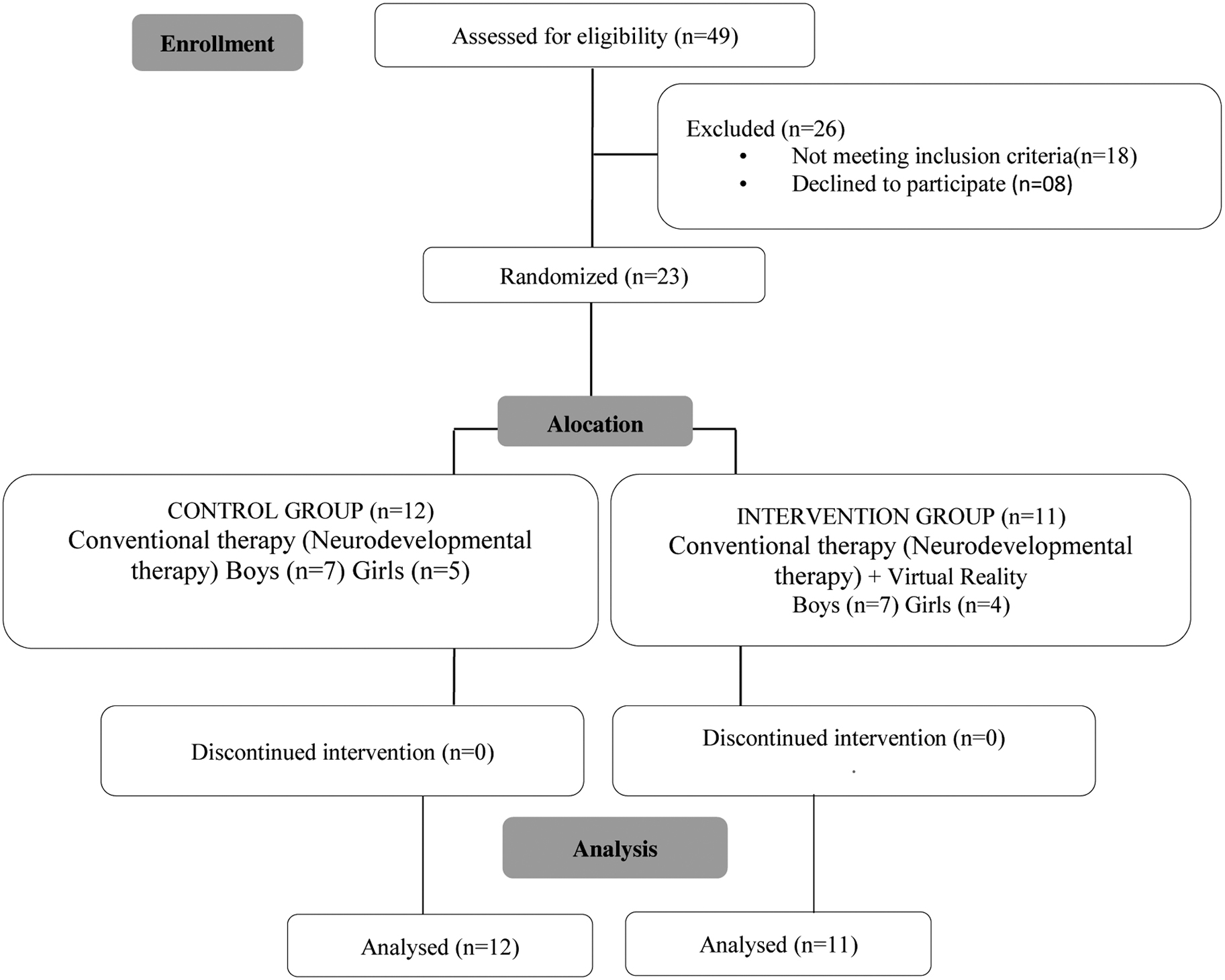
Flowchart of the study stages.
The children were selected based on the following inclusion criteria: (1) age between 5 and 12 years; (2) ability to understand verbal commands and interact with the proposed games; (3) ability to remain standing independently in a ST stance for 30 seconds; (4) GMFCS I; and (5) children with expected body weight and height for their age.
Exclusion criteria were as follows: (1) muscle shortening, pain or discomfort that would prevent them from completing the protocols; (2) application of neurochemical blocks in the 6 months before the study; (3) orthopedic surgeries in the last year; (4) presence of untreated sensory deficits (visual and/or hearing); (5) any degree of cardiorespiratory impairment reported by the parents/legal guardians; and (6) regular contact with game consoles such as Playstation 3, Nintendo® Wii™, and Xbox® 360° Kinect.
Participants were excluded if they missed more than three sessions without prior notification or justification; however, this was not necessary, and none of the children withdrew during the study.
Assessment procedures
The outcomes were assessed preintervention and 8 weeks after intervention.
The tests were performed by two physical therapists, with experience in pediatric neurology and in the evaluation with the force platform. The tests were applied in a randomized manner, by means of a lottery carried out previously. All test procedures were performed on the same day. A break of at least 2 minutes was made between each attempt to assess postural control. If the child showed signs of fatigue, a longer time of rest was provided.
The assessment of postural sway using the force platform has been validated for use in children with CP, and has good feasibility.29,30 Participants were instructed to stand barefoot on a force platform and the desired foot position was marked for each individual to standardize the stance adopted. The assessment conditions for body oscillation were as follows:
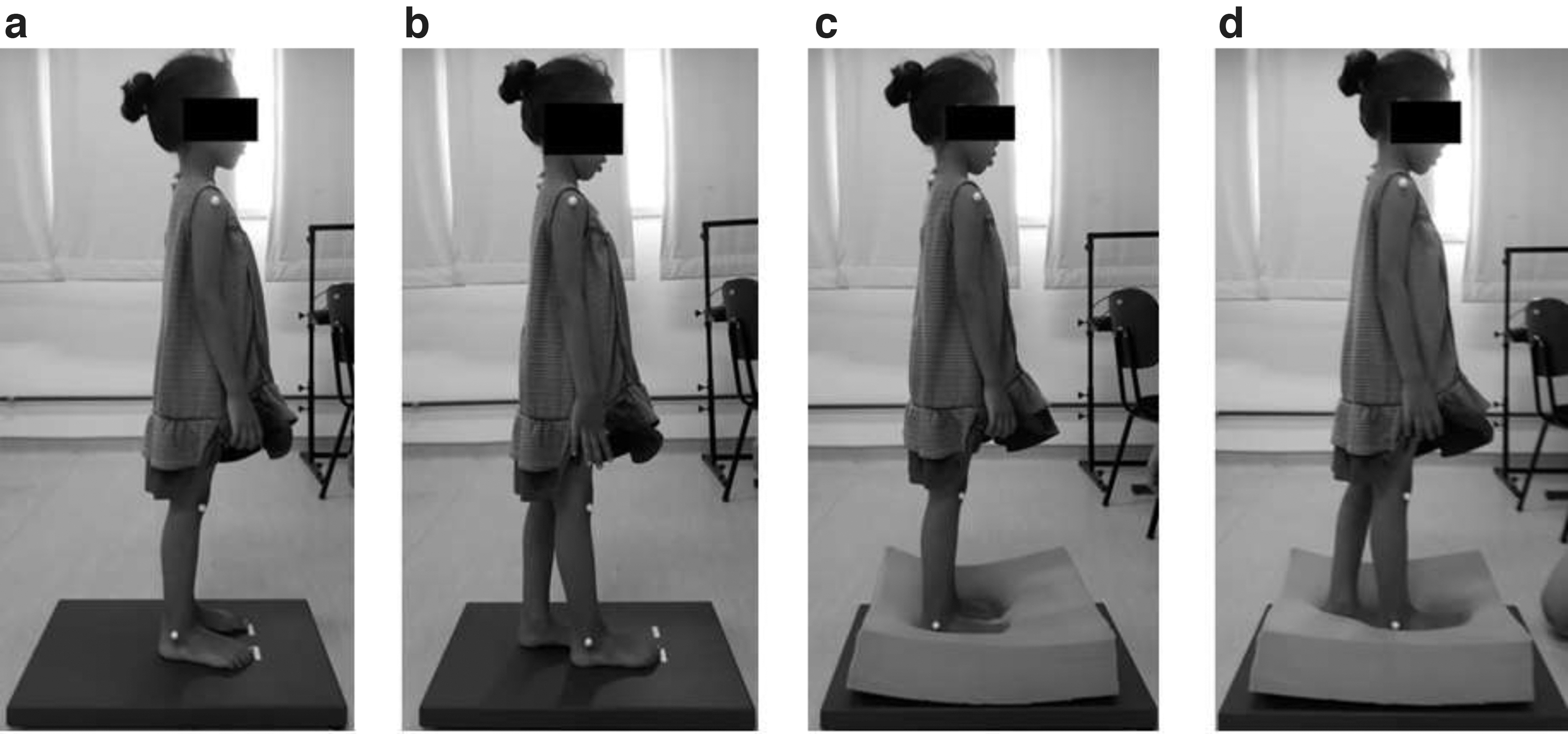
Control condition (CC): performed on a rigid surface (the force platform itself) with the feet parallel and in line with the hips (Fig. 2a). Feet in an ST stance: first metatarsophalangeal joint of the nondominant foot aligned with the medial longitudinal arch of the dominant foot on a rigid surface (Fig. 2b). Flexible surface (FS): foam placed on the platform, feet parallel, and in line with the hips (Fig. 2c). FS (foam on the platform) and feet in an ST (FSST) stance (Fig. 2d).
Body oscillation assessment on a force platform under the CC
For all the conditions assessed, the children were instructed to remain as still as possible for 30 seconds, 6 focusing on a point at eye level, 1 m away. 31 Five attempts were made for each condition, with the first disregarded as familiarization and the last due to possible fatigue during assessment. Three valid attempts were considered and the average of these was used for analysis. 32
The reassessment was performed exactly 1 week after the end of the last intervention session, to prevent the child from performing poorly due to being tired, if the assessment was performed on the same day as the last session.
Data collection
The data obtained on the force platform were normalized based on the height of each child in centimeters. 33 The variables calculated were as follows:
Amplitude of anterior–posterior (AP Amp) and mediolateral (ML Amp) displacement (cm): distance between the maximum and minimum CoP displacement in each direction. 31
Anterior–posterior root mean square (AP RMS) and mediolateral root mean square (ML RMS) of CoP displacement (cm): dispersion of CoP displacement from the average position over a time period. 34
Average total velocity of CoP oscillation (cm/s): calculated by dividing CoP excursion by the test time, indicating how fast postural responses were.31,35
Total area of CoP oscillation (cm2): calculated by dividing displacement data for total oscillation by the total time of the attempt, generating an ellipse from CoP dispersion measurements.
Intervention procedures
Intervention group
The intervention was carried out over 8 consecutive weeks19,26,36 and consisted of 2 weekly 45-minute individual sessions, totaling 16 sessions and 12 hours of training. We chose this additional dose of VR therapy because it was feasible for parents and therapists, given the weekly duration. Furthermore, studies demonstrate that this dose of VR therapy is sufficient to establish improvements in the functional balance of children with CP.5,37
The children continued to take part in the conventional interventions they were already involved in. Therefore, in the experimental group, 50 minutes of neurodevelopmental therapy plus 45 minutes of VR therapy were performed weekly (on separate days).
Given that the participants could not have had previous contact with VR games, all the children in the experimental group began the intervention with basic-level games for familiarization purposes. Familiarization was performed using two beginner-level Kinect Adventures games for the first 2 weeks (four sessions):
River Rush—player avatars have to navigate a raft through rapids and avoid a series of obstacles.
Reflex Ridge—players race through hazardous rollercoaster-like tracks on platforms while avoiding obstacles.
In the weeks following familiarization, dynamic sports games were used in a VR environment:
Athletics: 100-m stationary run.
Long jump: once participants gain momentum with the stationary run, they perform a vertical jump as high as possible and land in the same place, flexing their ankles, knees, and hips to absorb the impact, and then return to an upright position.
Javelin throw: participants execute a stationary run to gain momentum and throw the javelin as far as possible. The virtual javelin throw requires trunk, pelvis, and hip rotation in addition to training dynamic balance.
Figure 3 illustrates the child's positioning during VR games.

Child's positioning during virtual reality games.
The order in which the games were applied during the intervention was randomized for each individual to prevent him or her from becoming habituated as much as possible. The games were initially set to beginner level and the complexity increased based on the scores obtained.
The entire intervention was supervised by a physical therapist specializing in pediatric neurology. During the sessions, the therapist provided instructions on how to perform the movements, and standardized feedback.
Control group
The children in the control group underwent conventional physiotherapy, based on the concept of neurodevelopmental therapy, 38 twice a week at 50 minutes per session. It was applied by the senior physical therapists at the clinics that already treated the children, and the content of the sessions was not determined by the researchers of the present study.
Although these professionals did not receive specific training or an established protocol to follow, they had some form of training in the neurodevelopmental approach. Data were obtained on the type of intervention performed, duration, and frequency.
Statistical analysis
The descriptive statistics used were mean and standard deviation. Parametric tests were applied based on the data normality and homoscedasticity indicated by the Shapiro–Wilk and Levene's tests.
Repeated-measures analysis of variance (ANOVA) was applied for comparisons and interactions between the groups (control and intervention) and time (pre and post) for each base of support and FS assessed. The Bonferroni correction was used for multiple comparisons.
The percentage variation was calculated in both groups for all the variables, using the formula ([POST-PRE]/PRE*100). The T-test was used to identify possible differences, considering normal data distribution. Cohen's d was used to test the practical relevance of the percentage variation. 39
Significance was set at P ≤ 0.05 and the theoretical assumptions for the specific analyses were taken into account.
Results
The CG and IG had similar baseline clinical and demographic characteristics, as indicated in the results presented in Table 1.
Clinical and Anthropometric Characteristics of the Intervention and Control Groups
Means ± standard deviations, except for the sex of the children (percentage). For statistical analysis, the T-test or Mann–Whitney test was applied for parametric and nonparametric data, respectively, except for sex.
BMI, body mass index.
An effect was observed for time (pre- and postintervention) for the variables and conditions FS— ML amplitude (F1,21 = 6.743; P = 0.01) and FS—ML RMS (F1,21 = 7.104; P = 0.01), with a postintervention decline in postural oscillation. The remaining conditions and variables showed no main effect between participants, and a main effect was not observed between groups for any of the variables.
There was significant interaction for the following conditions and variables: a decline under the CC— ML amplitude (F1,21 = 5.948 P = 0.02) in the IG after intervention, and a postintervention increase in average total velocity for the FSST stance (F1,21 = 4.653 P = 0.04) in the IG.
The percentage change was significant only in the IG. From pre- to postintervention, there was a 13.01% decrease in ML amplitude (t19 = 2.911, P < 0.01) and 11.65% for ML RMS (t20 = 2.20, P = 0.03) under the CCs. Average total velocity increased significantly by 9.92% (t19 = 2.14, P < 0.05) for the FS and ST conditions. A large effect size was observed for the three variables (Table 2).
Descriptive and Statistical Results for the Group and Time Effects and Group-Time Interactions for the Body Oscillation Variables of Children with Cerebral Palsy Under Different Base of Support and Flexible Surface Conditions
Bold values p < 0.05.
Significance of *P < 0.05. Effect of Group*Time interaction = Δ. Positive % change values indicate an increase, and negative values a decrease in the variable. Significant intergroup difference = •.
AP, anterior–posterior; ML, mediolateral; PWR, power; RMS, root mean square; ST, ST, semitandem.
Discussion
The aim of the present study was to assess the effect of nonimmersive VR training as complementary rehabilitation in children with CP while standing on different BoS and surfaces. The hypotheses were confirmed because changes were observed in body oscillation in the intervention group for the least and most complex tasks, feet parallel on a rigid surface and an ST stance on an FS, respectively.
A positive effect was observed for the multisensory stimuli provided by the VR-based intervention, evident in the decreased ML amplitude of CoP oscillation under the CCs and greater total average velocity for FSST. There are indications that impairments in the postural control systems of the participants while standing were minimized by the training performed. Body oscillation deficits are common in children with CP, 34 even when considered mild, since it may be more difficult to revert ML and AP oscillation over short time periods.40,41 The findings of lower ML amplitude and higher average velocity after training suggest that these difficulties may be mitigated by VR intervention combined with conventional therapy.
The changes in postural oscillation on both the rigid and FS may have occurred due to the task-oriented approach used, with VR games that constantly challenged the limitations of the BoS and provided a large number of task repetitions. 13 The games used trained movements such as squatting, jumping, and ML displacement and may have improved postural control in the ML direction, as demonstrated in the results. The games require the children to move their bodies in the frontal, sagittal, and transverse planes, constantly changing the direction of weight shifting and generating somatosensory stimuli capable of triggering tactile receptors and proprioceptors. 34 Rapid changes in the direction of movement in response to visual and auditory information from the games and feedback from the body travel to the sensory motor cortex and down the spine, where the necessary postural adjustments are made to maintain dynamic stability. 34
Task-specific training is considered an important pillar of intervention for children with CP, regardless of the therapy technique used.15,42 This type of approach is based on the practice of real-life activities, using self-generated movements, with less emphasis on remediation or “normalization” of movement components. 43 Based on the Dynamical Systems Theory, this type of treatment assumes that the interaction between the child, the task, and the environment results in efficient solutions for functioning, through spontaneous self-organization and the interaction of subsystems to achieve a functional goal. 44 In this way, the plasticity generated from the experience is modulated through the child's attention when performing the task, which generates positive results, such as those presented in this study.15,42,45
Another noteworthy aspect is the ability to manipulate the support surface by adding foam. It is well known that sensory manipulation can increase body oscillation, 46 especially in children with neurological deficits such as CP. 47 The foam altered the sensory inputs on the soles of the feet, increasing the need for additional sensory information to effectively control posture, such as the visual or vestibular systems, which tend to counteract body oscillations and maintain balance. 48 Thus, the 13.01% reduction in body oscillation and 11.65% in variability after VR training in the present study were an important gain for the participants.
The VR games used, such as athletics, long jump, and javelin throw, may have helped the children achieve better postintervention control of their bodies under the instability caused by the foam. It is important to note that squatting requires synergy between the muscles of the legs and pelvis, 49 which also act to maintain postural control while standing. 50 As such, the dynamics of the tasks performed in the virtual environment may have enabled more integrated functional training, facilitating selective motor control via muscle synergy during the specific tasks of squatting, jumping, and standing.
VR games may have favored the processing and integration of multisensory information, especially because they require players to respond to visual and auditory cues, instantly reproducing movements of the avatar on the screen to achieve the goal of each task.13,19 It can also be inferred that training involving weight shifts, changes in trunk, leg, and head positions, in association with the pace and speed of the game, may have favored the use of proprioceptive and vestibular information with consequent activation and control of antigravity muscles, thereby improving automatic posture control. The results therefore support the idea that the multisensory information provided by VR games/consoles may help modify movement patterns in children with CP,51–53 causing dynamic changes in the flow of sensory information,34,54 which could favor postural control gains.
Also, although we did not use foam as part of the intervention, children with CP were able to transfer the skills acquired during the intervention to assess the outcome of oscillation with foam. This result can be explained by the principles of motor learning. Motor learning occurs through relatively permanent internal changes, due to experience and practice of activities, resulting in the acquisition, retention, and transfer of motor skills. 55 Studies show that children with CP are able to transfer their learning acquired when performing task-oriented therapy.
Duff and Gordon 56 observed that after training children with CP to reach objects, they were able to adapt to the task of carrying heavier objects, developing an effective motor program. Rieckmann and Bäckman 57 verified motor learning through neuroimaging examinations, detecting activation in the cortical areas and brain activity in different brain areas after practice. Thus, the results of our study indicate that skills acquired in the VR environment can be transferred to the real environment. 58
The average total velocity of CoP oscillation only increased in the IG when sensory manipulation was applied, that is, with participants standing on a foam surface in an ST stance. Integrating sensory information helps control body oscillations, and postural control tends to oscillate more under conflicting sources of sensory information. 48 The postintervention increase in total average velocity may have occurred as a strategy adopted by the children under highly demanding task conditions. Virtual training may have released degrees of freedom, which precedes the emergence of a more controlled and coordinated control pattern. The release of degrees of freedom is considered an exploration of movement possibilities, aimed at successfully adapting to the proposed task. 59
It is important to underscore that the improved postural control in the experimental group may also be related to the greater dose of the rehabilitation therapy applied, since these children underwent VR training in conjunction with conventional therapy. Indeed, larger therapy loads can provide greater gains in the development of motor skills. 15 The results of the present study show that VR training can be used as a complementary tool with conventional therapy and is an effective and easy method for increasing the amount of therapy that children with CP receive. 60 These results are in agreement with other findings in the literature, which reinforce that the virtual game, applied in addition to standard physical therapy, is beneficial in activities involving balance in children with CP, compared with standard therapy.61,62
The VR approach is appealing to children and can help improve development by providing more intense therapy without increasing costs and time demands for families.
Study limitations
Study limitations include the lack of follow-up measures due to the distance from specialist centers and the fact that the conventional interventions were performed by individual rehabilitation centers. In addition, despite the statistical significance and large effect sizes in the present study, future controlled trials with a larger number of children could help interpret the findings in terms of the effects of VR on children with CP.
Conclusion
Training using specific activities with a high number of repetitions in an appealing environment in the form of nonimmersive VR games could help improve specific body oscillation parameters in children with unilateral spastic CP and mild functional impairment. These findings contribute to guiding clinical therapy in terms of the potential of nonimmersive VR as a complementary tool in the physical rehabilitation of children with CP.
Footnotes
Authors' Contributions
N.A.C.F.R., J.L.B.A., and A.C.d.C. conceived of the presented idea. J.L.B.A., C.R.G.L., and B.N.V. collected the data. J.L.B.A., C.R.G.L., and B.N.V. collected the clinical data. A.F.R.K. performed the data analysis and statistics. All the authors contributed to the interpretation of the results. All the authors drafted the article. All the authors discussed the results and contributed to the final article.
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the grant, Coordination of Superior Level Staff Improvement—CAPES (PhD Scholarship); and by the grant, São Paulo Research Foundation—FAPESP (Grant Nos.: 2016/10396-7 and 2020/02818-4).