
Abstract
Objective:
To verify if individuals’ poststroke and healthy controls would improve their performance in reaction and movement times practicing a serious game task using the upper limb movements.
Materials and Methods:
We evaluated 30 individuals poststroke and 30 healthy controls, matched for age and sex. We used the “Association Game for Rehabilitation” (AGaR) where participants played by matching a pair of images whose meanings were similar. Hand movements were captured by a Kinect system and poststroke participants used their nonparetic upper limb. Reaction time and movement times (time to select an image and movement time to the target) were measured. Data were analyzed using multiple analysis of variance.
Results:
Performance improved for both groups across all variables with better performance in movement times than reaction time only for poststroke individuals.
Conclusions:
Upper limb movements using nonimmersive serious games enhanced motor performance in reaction and movement times for healthy controls and individuals poststroke.
ReBEC Trial Registration: RBR-4m4pk; Registeted on 08/24/2018.
Introduction
Stroke is a major cause of disability and death worldwide. 1 Individuals poststroke have sensorimotor deficits that result in decreased ability to perform everyday activities such as writing, walking, and driving. 2 In particular, upper limb deficits including weakness in both arms, wrist and hand, 3 apraxia (difficulty planning movements), muscle tone, subluxation, contracture, swelling, and pain2,3 interfere with upper limb recovery. These upper limb limitations are a major contributor to the loss of independence poststroke. 4
Rehabilitation requires a thorough understanding of each persons’ health condition to provide a good quality of life.3–5 Virtual reality (VR) and serious games using computer-based programs and algorithms allow for rehabilitation to simulate interaction with real objects and events. VR has been shown to improve body function structures of poststroke individuals’ upper limb.2–6 It has been reported that coupling VR with therapy may be more beneficial than use alone.2–7
Some promising studies used commercial videogames owing to their low cost, easy availability, and portability. 8 They reported cognitive 9 and motor 10 improvements in individuals poststroke. However, an important question is whether gains may be greater with customized games, also called serious games. 11 This assumption is supported by evidence that device adaptation 12 and specific modifications to games especially developed for rehabilitation 8 have shown promising results.
In this study, a serious game “AGaR—Association Game for Rehabilitation” 13 was developed in a nonimmersive VR environment and used to promote movement for the nonparetic upper limb (less affected upper extremity) of individuals poststroke. According to the study of Bustren et al., 14 the nonparetic upper limb presents important movement deficits and it is necessary to undergo rehabilitation therapy for both upper limbs in poststroke individual.
Thus, the purpose of the study was to verify if individuals’ poststroke and healthy controls (age and gender matched) would improve their performance in reaction and movement time practicing a serious game task using the upper limb movements (i.e., the serious game presents images that should be matched with the target image using the upper limb movement). Therefore, we used a short-term motor learning protocol where participants using their upper limb had the opportunity to practice the “AGaR game” in familiarization phase (to understand the task) and then went to an acquisition phase (task practice with different association images).
Moreover, to verify transfer of performance all participants execute the same game but with small changes (first transference phase—changing the task order; and second transference phase changing the target image). We hypothesized that all participants would improve their performance in reaction and movement times with practice during acquisition and transfer but considering the poststroke individuals’ difficulty, even in the nonparetic upper limb, the control group will present better improvement in all protocol.
Materials and Methods
Ethics
This study was approved by the Ethics Committee from University of São Paulo (CAAE: 86130818.5.0000.5390 and No: 2.593.750) and was conducted in accordance with the Declaration of Helsinki. All the participants signed an informed consent.
Participants
Participants had a chronic (>1 year) ischemic poststroke and formerly participated in a rehabilitation group at Santa Casa de Diadema (an association for neurological rehabilitation).
Inclusion criteria were as follows: (1) diagnosis of poststroke for more than 1 year; (2) 30 years old or older; and (3) absence of surgeries or application of Botox on the evaluated upper limb in the last 6 months. Participants were excluded if they were not able to understand and perform the task (screened with three trials).
Instruments
The Kinect sensor was used as the natural user interface to acquire the movement data while participants interacted with the Association Game for Rehabilitation (AGaR). 13 A computer with an Intel® Core™ i7 processor, 8.0 GB RAM with Windows 8, 64 bits and NVIDIA GeForce GT 430 graphics card interfaced the hardware and software. The objective of the AGaR was to match a pair of images whose meaning is similar or complementary and in the end of each trial the game provides three dependent variables (reaction time, selection movement time, and target movement time). The main scenario (Fig. 1) has a central image as a target and four selectable images in the top. Three of these images are wrong and only one is correct. The correct image is randomly positioned among the four positions before each trial.

Task presentation—at the top are four images (airplane, boat, car, and train). The target is represented in the middle by a “road.” Thus, the correct task is to get the car image using the virtual hand (colored hand in the screen) and link it with the road.
Task execution
The game cursor is represented by an open and multicolor hand (Fig. 1) and it follows the movement of the player's hand in front of Kinect sensor. The game's starting point is a red solid bar, which turns yellow as the player's waving hand is detected (Fig. 1A). The bar turns green as the investigator selects the go signal (Fig. 1B). The player moves their hand to the correct image (Fig. 1C) and drags the image to overlay the central image (Fig. 1D).
Game mechanics: if the combination of images is a hit (correct), a sound is emitted, the target image is outlined in green (Fig. 1D) and the game moves to the next round. Otherwise, if the combination is an error, a different sound is emitted, the target is outlined in red, and the selected image returns to the initial position. The participant must match the images to move on to the next trial. The game ends when all the rounds determined by the protocol are performed.
Data collected
At the end of each trial the following data are stored (one reaction time and two movements time):
Reaction time: interval of time between start signal (green) and movement. Selection movement time (movement time to select an image): how long the participant took between the start cue to the selection of an image. Target movement time (movement time for the target): how long the participant took to move the selected image from its initial position to the target image.
Participant characterization and preliminary familiarization
Cognition was assessed with the Mini-Mental State Examination (MMSE) 15 and stroke severity with Orpington Prognostic Scale (OPS). 16 After the assessment, the participants were seated in a comfortable chair 2 m away from the computer screen. Before starting the experiment, the procedure was explained verbally: the subject was instructed to be seated on the chair and raise their preferred upper limb (i.e., the poststroke participants used the nonparetic upper limb) until the Kinect sensor recognized their arm. This allowed them to understand how the games represented their hand as an avatar on the computer screen.
Game protocol
The protocol was divided into three phases: familiarization, acquisition, and transfer.
Phase 1: Familiarization (three trials)
The participants practiced three trials to ensure that they understood how their movements were represented in the game. The sequence of trials used three different tasks with four images and a target image to match as follows—Task A: the target image is a road and the possible images to select are a car (the correct answer), a train, a ship, or an airplane; Task B: the target image is an aquarium and the possible images to select are a fish (the correct answer), a horse, a dog, or a bird; Task C: the target image is a football field and the possible images to select are a ball (the correct answer), a book, a lampshade, or a fan. Thus, during familiarization, participants experience all three possible tasks (A, B, and C).
Phase 2: Acquisition (21 trials)
During the practice execution, participants played the same game and sequence as in the familiarization phase; however, this time with different sequences of tasks repeated (i.e., ABC, ABC…). Each sequence was played seven times, for a total of 21 trials.
Phase 3: Transfer (12 trials)
Transfer (12 trials) was divided into two transfers to provide only one modification of the task characteristic at a time. Transfer test is used to assess the capacity to maintain the same performance acquired with practice when changing something in the task (i.e., similar task with just a small change).17,18 Thus, we used Transfer 1 (changing the sequence of task order)—the same task from acquisition and familiarization was used but with a different sequence, the participant had to practice each task twice in a row sequence (AA, BB, CC), totaling six trials; and Transfer 2 (changing the image)—the sequences from Transfer 1 was repeated again (AA, BB, CC) totaling six trials, but the correct images were changed (i.e., correct answer for the targets were changed). For Task A, instead of a car, there was a motorcycle; for the Task B, a different species of fish was used; and for the Task C, instead of a ball, there was a soccer stand (Fig. 2).

Study design. Color images are available online.
Data analysis
Disregarding the three attempts at the familiarization phase, there were 33 attempts for the experiment. The attempts were divided into four blocks in the acquisition phase (first block with means of six trials and other blocks with means of five trials), one block in transfer phase 1 (means of six trials), and one block in transfer phase 2 (means of six trials). The dependent variables used for the analysis were as follows: (1) the reaction time (time between the start button turns green and the participant's movement), (2) selection movement time (time between the start of the movement and the arrival in the selected object), and (3) target movement time (time between object selection and arrival at the target). The dependent variables were the time in milliseconds in each attempt divided into six blocks as explained before.
Multiple analysis of variance (MANOVA; between group evaluation) was used with repeated measures to compare the six blocks. The least significance difference was used as a post hoc test. Partial eta squared (
Results
Sixty participants completed the study. The experimental group had 30 poststroke participants from 33 to 74 years old, both sexes. The control group had 30 healthy subjects, matched for age and gender (Table 1).
Characteristics of the Sample
Data are presented as mean (SD) and [minimum–maximum] followed by the P-value of the Student's t-test for continuous variables; and for categorical variables, data were presented as relative (%) and absolute (n) values, compared with chi-square test with post-Bonferroni test (for intra- and intergroup comparison).
Intragroup comparison with <0.05.
Intergroup comparison with <0.05
SD, standard deviation.
The healthy controls had higher cognition and education. The participants’ characteristics are given in Table 1.
Results of the nonimmersive VR task
The MANOVAs showed a significant effect for Blocks (Wilks’ lambda = 0.452; F15,39 = 3.15; P = 0.002;
Reaction time
Individuals poststroke had a slower reaction time performance and greater variability than healthy controls (main effect for Group: F1, 58 = 4.56; P = 0.037;
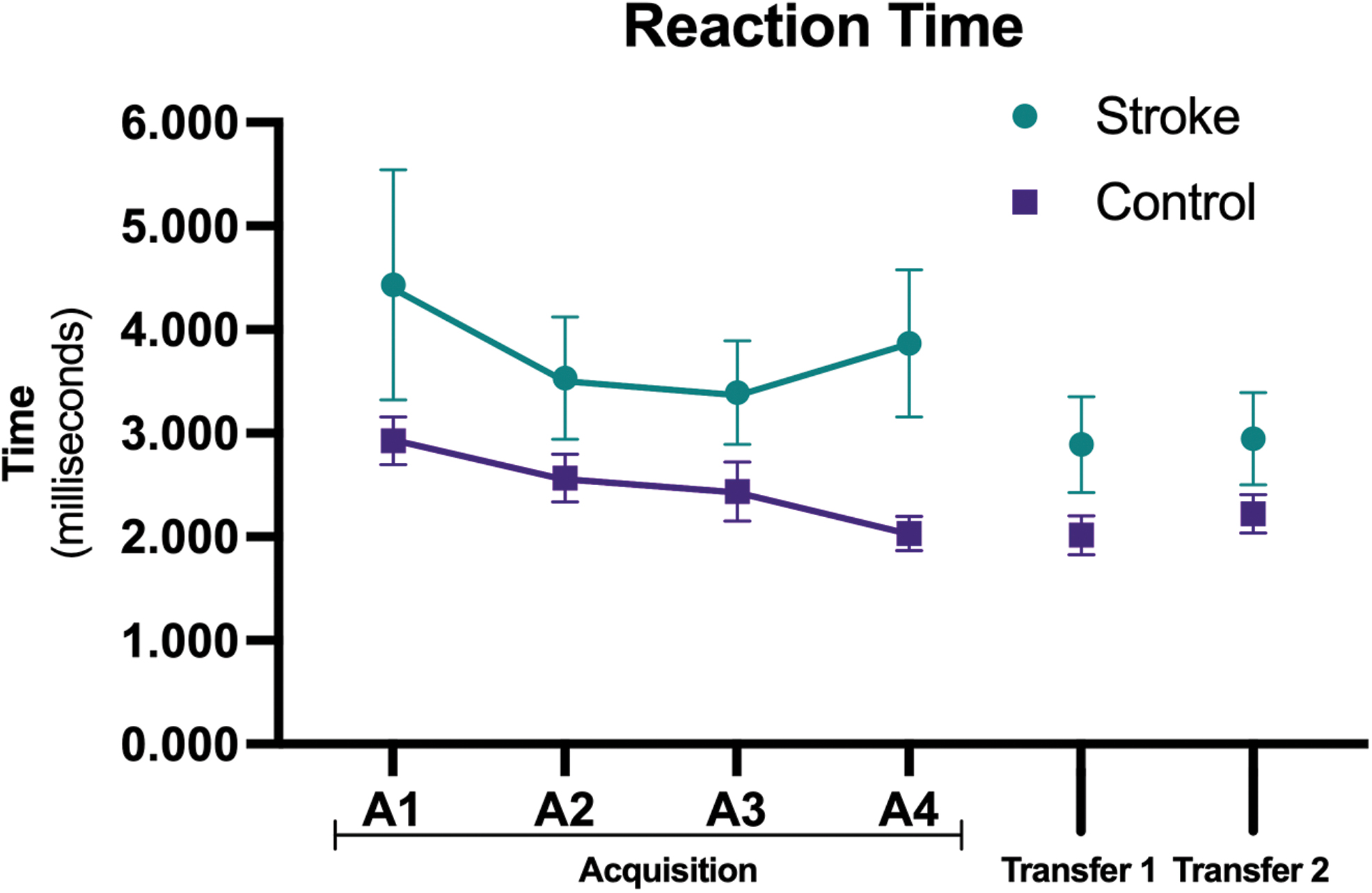
Reaction time (mean and standard error), for both groups in the six blocks of practice of the task. Color images are available online.
Selection movement time (image)
Individuals poststroke had a longer selection movement time performance than healthy controls (main effect for Groups: F1, 53 = 10.6; P = 0.002;

Selection time to select image (mean and standard error), for both groups in the six blocks of practice of the task. Color images are available online.
Target movement time (t)
Individuals poststroke had a longer target movement time performance than healthy controls (main effect for Group: F1, 53 = 7.87; P = 0.007;
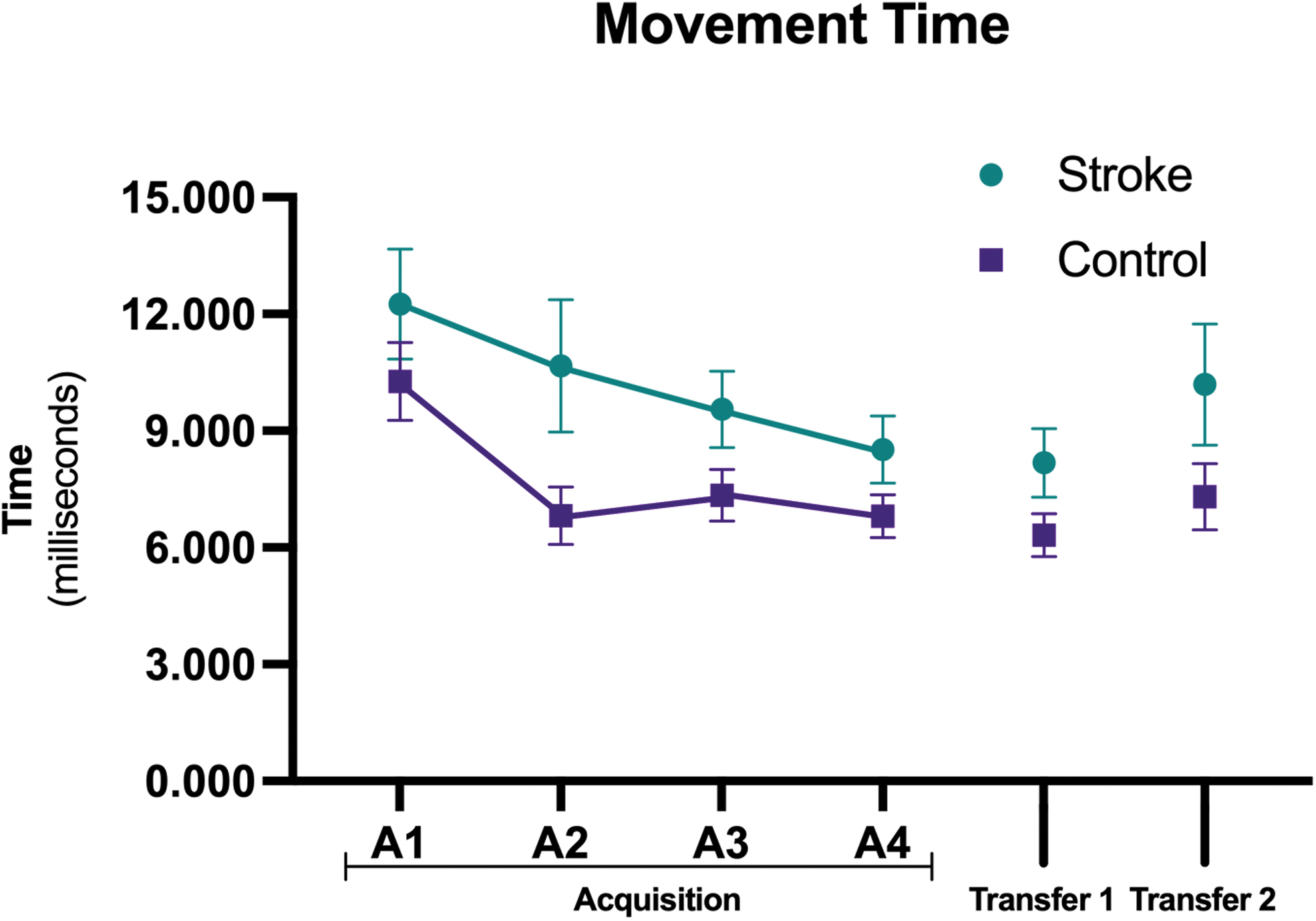
Movement time for target (mean and standard error), for both groups in the six blocks of practice of the task. Color images are available online.
It is important to emphasize that regression analysis did not find any factor (age, Orpington scale score, affected upper limb, and MMSE) that had influenced the performance improvement during the practice, in the three dependent variables evaluated (reaction time, selection movement time, and target movement time).
Discussion
This study evaluated the improvement of performance in reaction and movement times with the practice of a nonimmersive serious game in poststroke individuals and healthy age- and gender-matched controls. Our hypothesis was partially supported: both groups improved performance in the game on most variables during acquisition with maintenance of performance to transfer phases and the healthy controls performed better than the poststroke group.
Poststroke individuals presented functional impairment that affects their day-to-day function 20 and several limitations in muscle control and movement to execute function tasks.21,22 Those difficulties could be responsible for the poor performance in reaction and movement times practice when compared with the control group.
Considering that our protocol used acquisition and retention phases and analyzed three performance variables (reaction time, selection movement time, and target movement time) in a serious game developed for this proposal, our results showed poststroke individuals improved during the acquisition phase (from A1 to A4) in movement time variables (selection and target movement times), but not for reaction time (Fig. 3). Probably the high variability during practice in reaction time was responsible for the lack of improvement in individuals with poststroke during acquisition. According to Hammerbeck et al. 23 that analyzed individuals with poststroke during a task of reaching objects at different speed, the improvements in performance were achieved by reducing variability.
We can speculate that lack of tactile feedback in our study (because of the virtual environment) decreased the perception of the beginning of the movement, 24 which coupled with the small amount of practice, 25 could be responsible for the high variability and lack of improvement in the reaction time performance. On the contrary, reaction time was the only variable that individuals poststroke presented difference with improvement of performance from acquisition to both transfer phase (Transfer 1 with the same task but with different sequence and Transfer 2—with target changed). Probably participants poststroke had to organize their practice during acquisition in reaction time with high difficulty (high variability) and this difficulty did not allow improvement in acquisition but provide capacity to adapt and present better performance in transfer phases.
Individuals with poststroke and control participants presented the same pattern of performance in their movement times (selection movement time and target movement time). Both groups improved in acquisition phase and maintenance performance to Transfers 1 and 2. Probably their improvement during practice in acquisition provided capacity to finish the task faster and with enough learning to transfer the task. It is important to emphasize that although the participants in the poststroke group had significantly less education and worse cognition (Table 1), they still improved during practice, with pattern of performance similar to the control group.
Although the different possibilities of technology-based interventions focused on techniques to stimulate upper extremity recovery after stroke 26 and the benefits in the use of VR to promote engagement, real-time multisensory feedback, task variation, objective progression, and task-oriented repetitive training elicits motor learning,27–29 our finding has clinical relevance for the use of nonimmersive serious games to improve reaction and movement times in poststroke individuals.
We propose two hypotheses for this performance improvement in individuals poststroke: (1) Easy task considering the patterns of movement: considering that independent variables used, such as MMSE, stroke severity with OPS (that verify upper limb motor deficit, proprioception, balance and cognition) age, and affected upper limb (right or left) did not influence the performance improvement in reaction and movement times (Fig. 5), we may conclude that the task did not need a high motor and cognitive ability, mainly using the nonparetic upper limb. Moreover, the game uses a task that requires proximal patterns of movement (e.g., the participants used their arm to control the task), there was no need of distal and fine movement (use of finger movement) and the possibility to use proximal movement promotes benefits to adapt to the task.
According to Debaere et al., 30 difficulty in the task that need to use touching with the fingers (task with aiming at a real object) will decrease peak acceleration and promote more final error in the target position and increased time to complete the task. Thus, the VR task used without a real object target facilitated the improvement of performance. Probable new technologies that allow grab, press, and hold objects using virtual environment will provide different and important results and should be scrutinized in the future. (2) Task repetition and familiarity: The AGaR software provided a task that can be repeated several times. Therefore, the possibility to repeat the same task and create familiarity with the computer game provided improvement for both groups in their movement times.
According to Foreman and Engsberg, 31 increasing familiarity with the computer games system can improve performance significantly in individuals poststroke. Moreover, individuals poststroke who received repetitive task training may be more likely to improve upper limb function after treatment and sustain these improvements after treatment than patients receiving usual care. 32 Although the existing suggestion that thousands of repetitions are required to retrain the brain to acquire a new motor skill after poststroke, 33 we believe that during an easy task with proximal movements, as AGaR software used, just 30 repeated movements were enough to promote short-term performance improvement in movement times.
Limitations and future studies
One of the limitations of this study was that the data were not extrapolated to function in daily life activities, and we used only one game to verify the performance on reaction and movement times. A second limitation is that we did not analyze specific patterns of movement during practice (i.e., kinetic or kinematic analysis of movement could provide interesting results). A third limitation is that we organized a short-term protocol in a cross-sectional study with only 1 day of practice and those results can be considered as an indication of positive use of VR but cannot be generalized as a training protocol, a long-term protocol with two intervention group should be organized in the future to support the use of serious game for rehabilitation.
Thus, we can conclude that using an associating task in a nonimmersive serious game, participants poststroke improved their performance in reaction time (transfer phase) and movement times (acquisition and transfer) but did not perform as well as the control group.
Footnotes
Authors’ Contribution
F.A.A.C.G. and W.S.S. collected patient data and drafted the article. T.D.S. performed the statistical analyses, interpreted the data, and revised the article critically for intellectual content. T.B.C., M.M., and F.M.F. drafted the article. F.N., A.F., and R.V.A. developed the game used and revised the article. S.B. and J.E.D. revised the article critically for intellectual content. C.B.M.M. and F.H.M. coordinated the study, drafted the article, and revised the article critically for intellectual content. All authors read and approved the final version of the article.
Data Availability
Research data are made available by the authors to assist in scientific development. It can be obtained from Talita Dias da Silva: write at talita.dias@unifesp.br
Author Disclosure Statement
All authors report no conflict of interest. All authors were responsible for the content and writing of this article.
Funding Information
T.D.S. was supported by Fundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP)—Finance Code: 2016/08358-0. C.B.M.M. was supported by the FAPESP 2017/24991-7, and Conselho Nacional de Desenvolvimento Científico e Tecnológico—Finance Code 442456/2016-6.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.