
Abstract
Objective:
To examine the effectiveness of video-based game exercises and structured closed kinetic chain exercises in individuals with rotator cuff rupture.
Materials and Methods:
Forty-five individuals with rotator cuff rupture were included in this study. Individuals were randomly divided into three groups: a conventional exercise group (CEG), a structured closed kinetic chain exercise group (CKCEG), and a video-based game exercise group (VGEG). Interventions were performed twice a week for 6 weeks. Pain severity; pain threshold; disabilities of the arm, shoulder, and hand questionnaire (DASH); rotator cuff quality of life index (RCQOL); range of motion (ROM); and joint position sense and approximation force of all individuals were evaluated pre- and post-treatment.
Results:
There was a statistically significant difference in all values of the pre- and post-treatment of the groups (P < 0.05). When the differences between the groups were compared, CKCEG and VGEG values were more significant than CEG in all parameters (P < 0.017). Improvements in pain threshold, ROM in shoulder flexion and abduction, DASH score, and all parameters of the RCQOL questionnaire in VGEG were statistically more significant than CKCEG (P < 0.017).
Conclusion:
Individuals with rotator cuff rupture obtained more improvements in primary and secondary outcomes after closed kinetic chain exercise and video-based game exercise, rather than conventional methods. It was considered that video-based game exercise programs would be used in rotator cuff problems.
Introduction
Rotator cuff injuries are the most common cause of shoulder pain. Rotator cuff injuries occur as a result of overuse of the shoulder, deterioration of the shoulder stability, muscle weakness, and trauma. 1 Several physiotherapy methods are used in the treatment of rotator cuff pathologies. These methods include strengthening exercises, stretching exercises, posture and stabilization exercises, manual therapy methods, home exercises, electrotherapy modalities, and hot and cold applications.2,3 In addition to the lack of consensus on the treatment approach to be applied to patients with rotator cuff pathologies, it is also a matter of discussion on how the treatment approach should be. The methods to be applied should be planned according to the patient's condition and the degree of pathology. 4
In the past 20 years, closed kinetic chain exercises have gained importance in the rehabilitation of many musculoskeletal problems and have become one of the most preferred exercises. When the studies on closed kinetic chain exercises are examined, it is seen that most of the studies consist of lower extremity pathologies. Studies involving closed kinetic chain exercises in rotator cuff ruptures are insufficient in the literature, and there is no structured exercise protocol for closed kinetic chain exercises. 5
In the systematic review of Dong et al. on rotator cuff treatment, it was stated that there is no standard exercise protocol in the treatment of rotator cuff injuries. It was demonstrated that nonoperative treatments were effective for rotator cuff injuries. Also, they determined that creating specific exercise programs is needed in rotator cuff injuries. Studies evaluating the treatment of rotator cuff injuries highlight the need for more clinical trials to establish a treatment protocol. 6
Specific exercise protocols based on technology such as video-based exercises started to use with the development of technology rapidly. Currently, technological rehabilitation takes its place under the name of complementary approaches for individuals who need rehabilitation. 7 Motion-sensitive sensors have an important role in the rehabilitation with camera systems without the need for an additional device. Microsoft Kinect and Nintendo® Wii™ are shown as examples of these devices. 8
Video-based game exercise programs are defined as the combination of games and physical movements used for therapeutic purposes and designed to increase the physical activity and functionality of the person. 9 When the literature was examined, it was seen that studies on video-based game exercise programs were mostly conducted in the fields of neurological and pediatric rehabilitation.9,10 However, it has been stated that video-based game exercise programs used in shoulder problems are insufficient in the literature. Also, there is a need for studies on video-based exercise programs in rotator cuff ruptures. 11
This study aims to examine the effects of the structured closed kinetic chain and video-based game exercise program on pain, range of motion (ROM), approximation force, joint position sense, functionality, and quality of life in individuals with rotator cuff partial rupture. In addition, it is aimed to evaluate which treatment program is more effective in the rehabilitation of rotator cuff injuries.
Materials and Methods
Study design
This study is a single-blind randomized trial with participants allocated (1:1:1) to one of three groups. Forty-five individuals with partial rupture of the rotator cuff who met the inclusion criteria of the department of physical therapy of Istanbul Medipol University Hospital were included in the study. The protocol of the study was registered at ClinicalTrials.gov (NCT04426929). This study was performed according to the Declaration of Helsinki regarding the ethical principles for medical research involving human subjects. The study protocol was approved by the noninterventional ethics of Istanbul Medipol University, Turkey (File number: 10840098-604.01.01, No.: 1044). All study participants provided written informed consent.
Individuals were blinded to group assignments and experimenters were not blind to group assignment and outcome assessment. Individuals participating in the study were numbered according to the order in which they applied to the clinic. Then, considering these numbers, randomization was achieved using the “randomizer.org” website. Forty-eight individuals were divided into three groups: conventional exercise group (CEG) (n = 16), video-based game exercise group (VGEG) (n = 16) and closed kinetic chain exercise group (CKCEG) (n = 16).
Participants
Individuals who were between 18 and 60 years of age, with partial rupture of the supraspinatus muscle, not having professional sports history, having pain for >4 weeks, and not having any previous shoulder surgery were included in the study. Exclusion criteria were defined as having cervical neurological findings; having an additional orthopedic problem on the same shoulder; being uncooperative; having neurological, vascular, and cardiac problems that limit function; and having visual problems or sensitivity to light.
Flow of participants
Four of the 54 patients included in the study were excluded because they did not meet the inclusion criteria and 2 refused to participate in the study. Forty-eight individuals were divided into three groups by the randomization method. Three individuals were excluded from the study due to reasons such as COVID-19 and not participating in the exercises during the treatment process. A detailed study flowchart is shown in the consolidated standards of reporting trials flow diagram (Fig. 1).
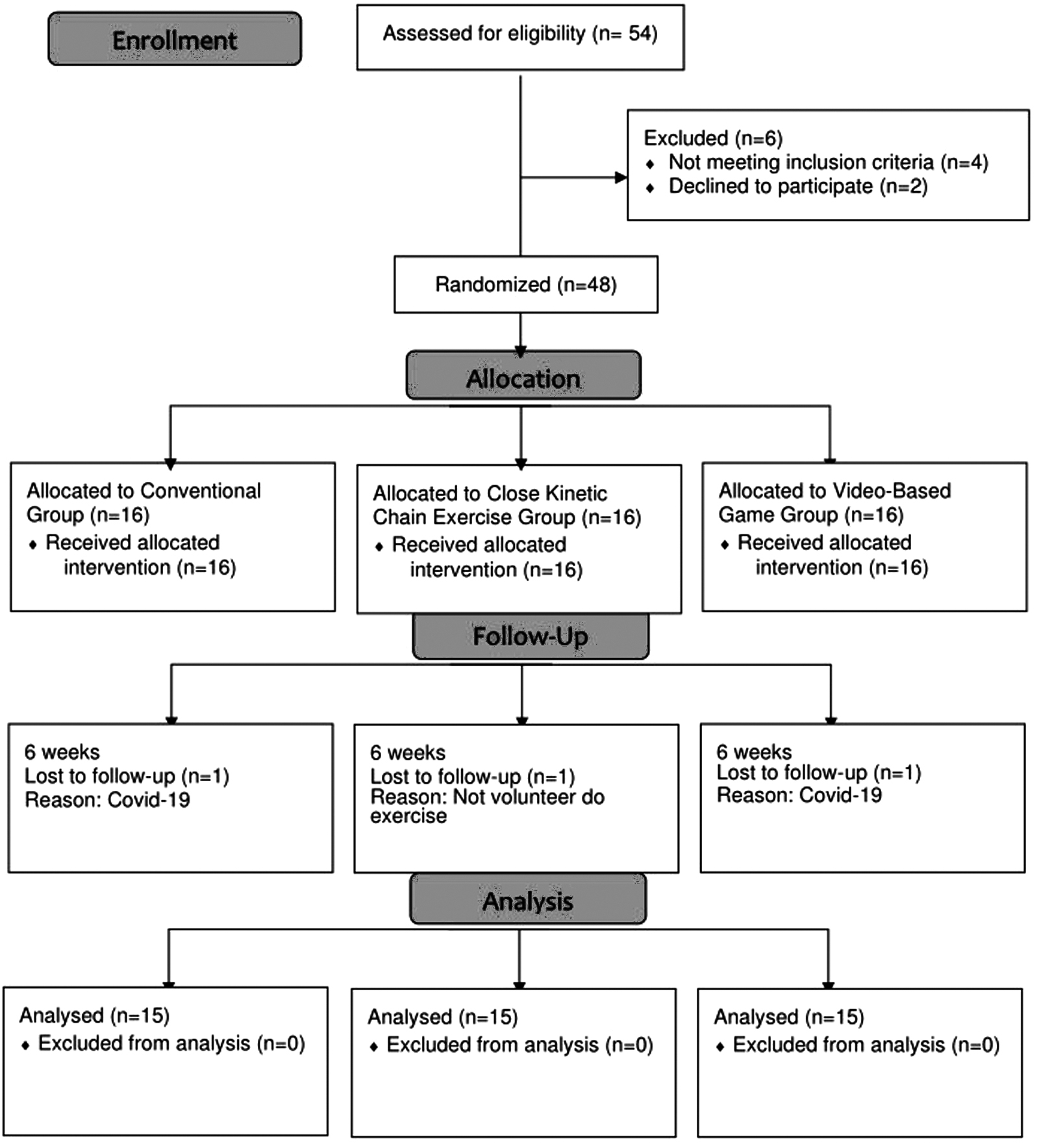
Design and flow of participants through the trial.
Intervention
Conventional exercise group
Wand exercises and shoulder wheel exercises to increase the ROM of the shoulder joint with 10 repetitions were applied in this group. Finger ladder exercises were performed in the abduction and flexion position with five repetitions, holding the endpoint for 5 seconds. Stretching exercises with five repetitions were applied in all directions for the limitation of movement, holding it for 20 seconds at the endpoint. Individuals performed conventional exercises twice a week for 6 weeks.
Structured closed kinetic chain exercise program group
A structured closed kinetic chain exercise program consisting of three phases for the shoulder, progressing from simple to difficult, including closed kinetic chain and proprioceptive exercises was created. Phase-1 exercises were designed to improve joint mobility and stabilization of the individual, phase-2 exercises were designed to increase joint ROM and muscle strength, and phase-3 exercises were designed to improve proprioception and stabilization. This exercise program was performed twice a week for 6 weeks under the supervision of a physiotherapist (Fig. 2).

Closed kinetic chain exercises.
Video-based game exercise group
A video-based game exercise program was applied twice a week for 6 weeks. The therapeutic serious games developed for shoulder rehabilitation were used by Fizyosoft and physiotherapists. “Armrotate” and “Uball” games were used by using Fizyosoft Extremity ROM, and “Balance Surf” and “Balance Adventure” games were used in Fizyosoft Balance System. Each game was of 10 minutes duration, for a total of 40 minutes under the supervision of a physiotherapist. Detailed information about video-based game exercises is shown in Figure 3.

Video-based game exercise. ROM, range of motion.
Outcome measures
Primary outcomes
Pain severity
The visual analog scale (VAS) is a frequently used clinical questionnaire for the assessment of pain severity. Pain levels of individuals are evaluated by choosing numbers between 0 and 10. Zero means no pain, 10 means unbearable pain. 12
Pain threshold
Algometer is a device used to evaluate the pain threshold, thanks to the pressure it applies. While increasing the pressure using the algometer, persons are asked to indicate at the first point where they feel pain or discomfort. The first point of discomfort is defined as the pain threshold of the individual. 13 In this study, the pain threshold was measured using an algometer. The pain threshold of the participants in the study was measured three times and the average was found.
Evaluation of joint ROM and joint position sense
The ROM of the joint and joint position sense of the individuals participating in the study were evaluated using Fizyosoft Extremity ROM (Supplementary Fig. S1). Fizyosoft Extremity ROM is a system developed by physiotherapists for joint ROM and joint position sense measurement. Fizyosoft Extremity ROM is a system that enables objective measurement of joint ROM by detecting reference points during extremity movements with its camera and sensors. In the Fizyosoft Extremity ROM system, the patient is expected to stand in front of the camera and perform the movement that is desired to be measured. In the study, shoulder ROM was evaluated in degrees with Fizyosoft Extremity ROM. 14
In the joint position sense measurement, the subjects were first asked to raise their shoulders to a certain degree, and then to bring them to the same angle with their eyes closed. The difference between shoulder angles was calculated by recording the eyes closed and open angle values.
Evaluation of shoulder approximation force
Fizyosoft Balance System was used to evaluate shoulder approximation force. The individual was asked to put both hands on the balance board and then apply downward force without using bodyweight during this measurement. Measurements were taken in standing and sitting positions (0° and 90°) (Fig. 4).

Fizyosoft balance system.
Secondary outcomes
Evaluation of shoulder functional activities
The disabilities of the arm, shoulder, and hand questionnaire (DASH) is frequently used to evaluate the limitations and functionality of individuals with shoulder problems in upper extremities. The DASH is a questionnaire consisting of 30 questions and 3 sections, used to evaluate parameters such as functional activities, symptoms, social function, work, sleep, and self-confidence of patients. 15
Evaluation of quality of life for the shoulder
The rotator cuff quality of life (RCQOL) is a questionnaire that evaluates the quality of life in rotator cuff pathologies. Since it is a disease-specific questionnaire, it is distinctive in the evaluation of quality of life. It is a questionnaire consisting of 34 questions and 5 subparameters that evaluates the physical symptoms of the disease, work activities, activities of daily living, and social and emotional status. Each question is calculated for 100 points and the total score is expressed as a percentage. 16
Statistical analysis
The sample size was determined using the G*power sample size calculator (G*Power, v.3.0.10). The required sample size was 42 with an 80% power (α = 0.05, β = 0.20) and medium effect size (f = 0.5). 17 “SPSS (Statistical Package for Social Sciences) version 20” program (SPSS, Inc., Chicago, IL) was used in the data analysis of the study. Intragroup and intergroup analyses of data with normal distribution were performed with “one-way analysis of variance (ANOVA).” The “Wilcoxon signed-rank” test was used to compare the pre- and post-treatment results of the groups. Difference analysis between groups was performed using the post hoc test “Tukey HSD.” The significance value was accepted as P < 0.05 for the one-way ANOVA, and the significance value for post hoc test was P < 0.017.
Results
Baseline characteristic
Individuals with a diagnosis of rotator cuff partial rupture were selected among those who applied to the Istanbul Medipol University Hospital. Individuals were divided into three groups such as CEG, structured CKCEG, and VGEG. There were seven men and eight women in the CEG, eight men and seven women in the structured CKCEG, and six men and nine women in the VGEG. The mean age of the CEG was 52.7 years, the mean age of the structured CKCEG was 50.8 years, and the mean age of the VGEG was 47.6 years.
There was no statistical difference between the baseline physical characteristics of the groups (P > 0.05). When the affected shoulder area of the individuals participating in the study is examined, eight of the individuals were right and seven were left in the CEG, seven of the individuals were right and eight were left in the structured CKCEG, and eight of the individuals were right and seven were left involvement in the VGEG (Table 1).
Baseline Characteristics of the Participants
CEG, conventional exercise group; CKCEG, closed kinetic chain exercise group; SD, standard deviation; VGEG, video-based game exercise group.
Effect of intervention
The comparison of pre–post treatment evaluation parameters within group is given in Table 2. When the values of the pre- and post-treatment of all groups in the study were compared, significant improvements were observed in all parameters (P < 0.05). In the comparison of the differences between the groups, CKCEG and VGEG values were more significant than CEG in all parameters (Table 3).
Comparison of the Values Pre- and Post-Treatment Within the Group
DASH, disabilities of the arm, shoulder, and hand questionnaire; ER, external rotation; IR, internal rotation; RCQOL, rotator cuff quality of life index; ROM, range of motion; VAS, visual analog scale.
Intra-Group Differences of Values Pre- and Post-Treatment and Comparison of Differences Between Groups
GI, conventional exercise group; GII, closed kinetic chain exercise group; GIII, video-based game exercise group.
There were no significant differences between CKCEG and VGEG on VAS/resting, VAS/activity, shoulder extension ROM, shoulder internal rotation and external rotation, 0° and 90° shoulder approximation force, shoulder flexion, and abduction position sense (P > 0.017; Table 3). Improvements in pain threshold, ROM in shoulder flexion and abduction, DASH score, and all parameters of the RCQOL questionnaire in VGEG were statistically more significant than CKCEG (P < 0.017; Table 3).
Discussion
A significant difference was found in the pre- and post-treatment values in all parameters of the three groups included in the study. When the difference analysis between the groups was examined, more significant results were obtained in the VGEG and structured CKCEG compared with the CEG in all parameters. When the VGEG and the CKCEG were compared, the pain threshold, functionality, quality of life, shoulder flexion and abduction values of the VGEG were found to be more significant than the CKCEG. In other parameters, the two groups were not superior to each other.
Approximation force measurement in the shoulder rehabilitation
New methods are emerging in the treatment and evaluation parameters with the developing advancement of technology. Fizyosoft Extremity ROM and Fizyosoft Balance System are technological products that provide objective data in the measurement of ROM, joint position sense, and approximation force in the field of physiotherapy. As far as we know, the approximation force measurement used in the study has not been evaluated in shoulder patients before. This study evaluated the shoulder approximation force for the first time, and we believe that it will be a guiding method for future research in the field of shoulder rehabilitation. 18
Video-based game exercise programs in the shoulder
Exergame applications are used in many different disease groups to reduce movement problems and improve balance in individuals with Parkinson to increase upper extremity functionality in hemiplegic patients, and to improve balance performance in geriatric individuals with osteoarthritis.19–21 Although exergame applications applied in neurological and geriatric problems are frequently preferred in the literature, it is emphasized that its use in rotator cuff problems is insufficient. Exergame applications have been preferred in many studies in the literature using technological rehabilitation. 22 Unlike the literature, serious games designed for the individual's specific shoulder problem were preferred in this study.
Pekyavas et al. investigated the effectiveness of exergame applications and home exercise programs on pain, functionality, and scapular dyskinesia in individuals with subacromial impingement syndrome and scapular dyskinesia. 17 It was stated that pain and functionality results in exergame applications were better than those in home exercises. Contrary to that study, this study included serious games that included both open kinetic chain and closed kinetic chain exercises. Visual and sensory feedback in serious games reduced the pain of the individuals and increased their participation in the treatment, making video-based game exercises more effective.
It is considered that closed kinetic chain exercises can be added to the treatment program in addition to open kinetic chain exercises for the rehabilitation of proprioceptive sensation and stabilization problems that are impaired in rotator cuff injuries. Especially in this study, the approximation force and joint position sense values measured at 0° and 90° in the VGEG had better results than those in the CEG.
Studies on orthopedic exergame and serious applications in upper extremity rehabilitation are limited. There are studies on its use mostly in pediatric and neurological rehabilitation.23,24
Jonsdottir et al. reported that hand
Closed kinetic chain exercises in the shoulder
In shoulder pathologies, the kinetic chain should be added to the treatment program as a whole. Closed kinetic chain exercises are important for facilitating cocontraction of the rotator cuff muscles, scapular muscles, and deltoid muscles. 26 It has been reported that exercises given to increase stabilization in individuals with shoulder pathology have a positive effect on pain-related shoulder function, muscle strength, and normal ROM. 27 Therefore, stabilization of the glenohumeral joint and scapulothoracic joint is of great importance in individuals with shoulder pain.
There is no detailed treatment program to increase glenohumeral and scapular stabilization in the literature. In addition, there is no standardized program regarding exercise type, intensity, duration, and frequency in rotator cuff rehabilitation. Unfortunately, studies examining the effectiveness of closed kinetic chain exercises used in shoulder pathologies are limited in the literature.
The stabilization of the shoulder joint is provided by static and dynamic structures. It is known that the structures that provide joint stabilization are related to the proprioceptive system. 28 Dilek et al. reported that stabilization exercises given to individuals with subacromial impingement syndrome improved proprioception. They recommended the application of closed kinetic chain exercises in addition to conventional treatment programs. 29 It was found that glenohumeral and scapular stabilization exercises had positive effects on reducing pain and increasing shoulder stabilization in individuals with shoulder pain. 30
Holmgren et al. emphasized the need for specific exercise programs in rehabilitation programs to increase stabilization in rotator cuff problems. 31 We have seen that closed kinetic chain exercises are more effective than conventional exercise methods in improving shoulder functions since they stimulate proprioceptive mechanisms and increase shoulder stabilization. The results of this study correspond to the studies already mentioned. The closed kinetic chain exercises we used in this study included exercises that were divided into phases and progressed from easy to difficult. We consider that it is important for physiotherapists to use and develop structured closed kinetic chain exercise programs for different shoulder problems, as was the result of this research for shoulder rehabilitation.
Limitations
It was planned to evaluate muscle strength at the beginning of the study, but muscle strength could not be evaluated due to the inability of the patients to tolerate the increase in pain during muscle strength measurement. This is the limitation of the study. Also, other limitations were that the number of participants was low due to the effect of the pandemic and short follow-up duration. In addition, three different protocols were used in this study. The dissimilar feature of the three groups is the types of exercises they contain.
CEG includes open kinetic exercises, the CKCEG includes closed kinetic chain exercises, and the VGEG includes exercises performed in both closed and open kinetic positions. Although they seem like different exercise types, all three groups are effective methods in shoulder rehabilitation.
Conclusions
Studies investigating the effectiveness of closed kinetic chain exercises and video-based game exercises for the shoulder are limited. In this study, individuals with rotator cuff rupture obtained more improvements in pain, pain threshold, ROM, functionality, joint position sense, and approximation force after closed kinetic chain exercise and video-based game exercise, rather than conventional methods. The VGEG is more effective than the CEG since the games are task oriented and the shoulder is exercised at different angles.
It has been shown that video-based game exercise programs can be used not only in neurological and pediatric diseases but also in rotator cuff rupture. Moreover, there are no previous studies evaluating shoulder approximation force in shoulder rehabilitation. We anticipate that Fizyosoft Balance System would be a new method in the evaluation of shoulder approximation strength in future studies.
Footnotes
Authors' Contributions
B.M. contributed to conceptualization, methodology, investigation, and writing
Acknowledgments
This study was published as a doctoral thesis numbered 676411 under the Council of Higher Education/Turkey (original name of the thesis is “Rotator cuff lezyonunda yapılandırılmış kapalı kinetik zincir ve video bazlı oyun egzersiz programının etkinliğinin araştırılması”). There is no disclaimer.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the project number “2020–13” within the scope of the Istanbul Medipol University Individual Research Project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.