
Abstract
Objective:
The use of virtual reality (VR) has been increasing worldwide, as devices are becoming more sophisticated and provide an escape from reality during the COVID-19 lockdown. This recent rise in the use of VR leads to new side effects being reported, such as dissociative symptoms that may or may not constitute a mental health concern. This retrospective study investigated the prevalence and intensity of dissociative symptoms in VR users, as well as some potential predisposing conditions that may trigger them, and their impact on the subjects' wellbeing.
Materials and Methods:
We conducted a survey (n = 358) that was posted on VR Facebook groups. This survey was approved by the University of Lisbon Medical Faculty's IRB, and comprised a modified version of the Clinician-Administered Dissociative State Scale (CADSS) and questions regarding potential risk factors known to induce dissociative disorders or experiences.
Results:
Data analysis revealed that 83.9% participants reported dissociative symptoms, with varying intensity according to CADSS (
Conclusion:
In conclusion, this study revealed that although VR can induce dissociative experiences, they seem to be short lasting and nonthreatening to the individual's wellbeing and might be predicted or attenuated by managing other known risk factors for dissociative phenomena.
Introduction
In the last decades, the development of new sophisticated technologies has changed the way media are consumed, from photo, film, and videogames, to the advent of virtual reality (VR) in the 1960s. The three-dimensional aspect of VR sets it apart from older technologies and allows for a heightened sense of immersion and presence. 1
Immersion usually refers to the objective ability of a system to provide sensorimotor stimuli that make the experience feel realistic. 2 High levels of immersion can be obtained with a high-resolution head-mounted display with full real-time motion capture, a wide field of view, and auditory and haptic feedback. 3 On the other hand, presence is the subjective experience of being in one place or environment, while being physically situated in another and it is, therefore, influenced by the level of immersion. 4
These qualities make users feel like they can navigate within new believable realities, making VR the next big disruptive technology in all kinds of fields, including health care. In fact, VR research is thriving in areas like pain management and a wide range of anxiety disorders (such as panic disorder or post traumatic stress disorder) and phobias.
Even though the most prominent quality of VR is its immersive potential, it is known that highly absorbing virtual experiences can lead to a sense of detachment from the “real” world and a consequential increase in depressive feelings. 5
In fact, the human mind defines what is real and what is not based on sensory evidence. VR blurs that evidence, since the visual and auditory sensory inputs that it provides are not met with the corresponding external sensory inputs, such as touch. Therefore, as both realities get mixed, VR users experience “consensual hallucinations” 6 that sometimes culminate in significant dissociative symptoms, such as prolonged difficulty in readjusting to the real world and a feeling that the outside world is not real, upon completion of a VR session. 7 This feeling of detachment from the real world, as if one is in a dream, is scientifically known as “Derealization” (DR).
Simultaneously, the use of virtual avatars whose hands or other body parts look different from the real ones, but move in synchrony with them (through the use of sensors and motion capture) makes for a very realistic “perceptual correlation,” that can induce a postsimulation feeling that a person's body is not his/her own anymore, or certain body parts do not feel his/hers. 8 This feeling of detachment from one's body is known as “Depersonalization” (DP).
VR's ability to alter body perception has been used before to help decrease neuropathic pain in patients with spinal cord injury, 9 or even stimulate mirror neurons that enhance the rehabilitation of stroke patients with hemiparesis. 10
Nonetheless, despite the possible advantages of dissociative phenomena in the treatment of some diseases, DP and DR symptoms are not innocuous when it comes to a person's mental health.
While epidemiological surveys demonstrate that transient symptoms of DP/DR (such as daydreaming) are common in the general population, 1%–2% of people reveal significant clinical manifestations that may integrate the diagnosis of Depersonalization/Derealization Disorder. 11 When these symptoms become frequent or intense, they can cause significant distress and impairment in social, occupational, or other important areas of functioning, as well as a variable degree of anxiety and depressive symptoms motivated by the patients' feeling that they are “going crazy” or experiencing irreversible brain damage. 12
Having highlighted the potentially harmful effects of depersonalization and derealization symptoms to a person's mental wellbeing, and knowing that, conceptually, VR has the power to induce those symptoms, it is natural to wonder whether VR is really safe for the use of the general population, especially for people who have known risk factors for DP/DR disorder, such as a history of certain psychiatric and neurological disorders, substance abuse, traumatic childhood events, and avoidant coping strategies. 13
Notwithstanding, to our knowledge, there is only one study to date that directly tested VR's dissociative potential, with results showing an increase in symptoms of DP/DR following VR exposure, especially in those with initial higher levels of dissociative symptoms and a tendency toward immersion or absorption. 13
Therefore, the present study aimed to broaden the research around this matter, by answering three different questions:
What is the prevalence and intensity of dissociative symptoms induced by VR? How do individual and gameplay-related variables affect the extent of those symptoms? What impact do the symptoms have on the subjects' mental wellbeing—are they anxiogenic? How long do they usually last?
These data could be helpful in assessing the safety of the growing VR use among the population.
Methods
This study was based on an online survey that was posted on five public VR Facebook groups, with a total of 324,000 members. Potential applicants were not told that the survey concerned dissociative symptoms before starting it, and were not offered any monetary incentive.
The ideal sample size was estimated at 300–400 participants, with a confidence level of 95% and a significance level of 5%. The survey was closed once it registered a total of 358 answers. Of the 358 participants who completed the survey, 19 (5.3%) were excluded due to incoherencies in their answers, and 5 (1.4%) for failing to provide informed consent, resulting in a total of 334 participants.
Data collection
The questionnaire was divided in three sections to answer each of the abovementioned three questions.
Section 1 (Q2–Q9) included nine questions that concerned gameplay-related and individual variables that could predispose to dissociative experiences (predictor variables), namely:
Gameplay-related variables: time spent playing VR; using apps that include fake hands or hand tracking; degree of immersion/presence;
Individual variables: history of psychiatric and neurological disorders, traumatic childhood events, previous dissociative experiences; substance use and self-reported avoidant coping strategies.
Section 2 (Q10–Q28) comprised the 19 subject-rated questions from the Clinician-Administered Dissociative State Scale (CADSS), 14 which was used to assess the prevalence and degree of VR-induced dissociative symptoms.
These questions regard various types of sensations that can be experienced in dissociative states, and the answers range from 0 (not at all) to 4 (extremely). The total score is calculated by the sum of all 19 answers, ranging between 0 and 76 points. The full survey can be found in the “Supplementary Material” section.
Section 3 (Q29–Q31) had the purpose of assessing if the symptoms were anxiogenic and how long they lasted, to calculate the real impact of the dissociative symptoms on the subjects' lives.
The full survey can be found in the “Supplementary Material” section.
Data analysis
Prevalence and intensity of dissociation symptoms
The total CADSS score was obtained by the sum of each of the 19 items from Section 2.
A descriptive statistical analysis was performed to determine the prevalence of dissociative symptoms among VR users (score ≥1), as well as the extent of those symptoms (given by the score's mean and standard deviation).
Predictor variables
The correlations between each of the predictor variables assessed on Section 1 (gameplay-related and individual) and the total CADSS score were determined using independent-samples t-test (for nominal variables) and Spearman's correlation coefficient (for ordinal variables). Significance was set at the ≤0.05 level.
Impact on mental wellbeing
A descriptive statistical analysis was performed to assess the duration and anxiogenic potential of the dissociative symptoms (assessed on Section 3). Independent-samples t-test was used to assess the association between anxiety symptoms and CADSS score. Spearman's coefficient was used to assess the correlation between the duration of symptoms and CADSS score. We also performed a Likelihood Ratio Chi-Square test to look for an association between symptom duration and anxiety symptoms.
Results
Prevalence and intensity of dissociation symptoms
A total of 280 participants reported some kind of VR-induced dissociative symptoms (score ≥1), adding up to a prevalence of 83.9%. Nonetheless, most of them reported a mild degree of those symptoms, having achieved relatively low CADSS scores, although with some variability (
A visual representation of frequency distribution is displayed on the histogram in Figure 1.
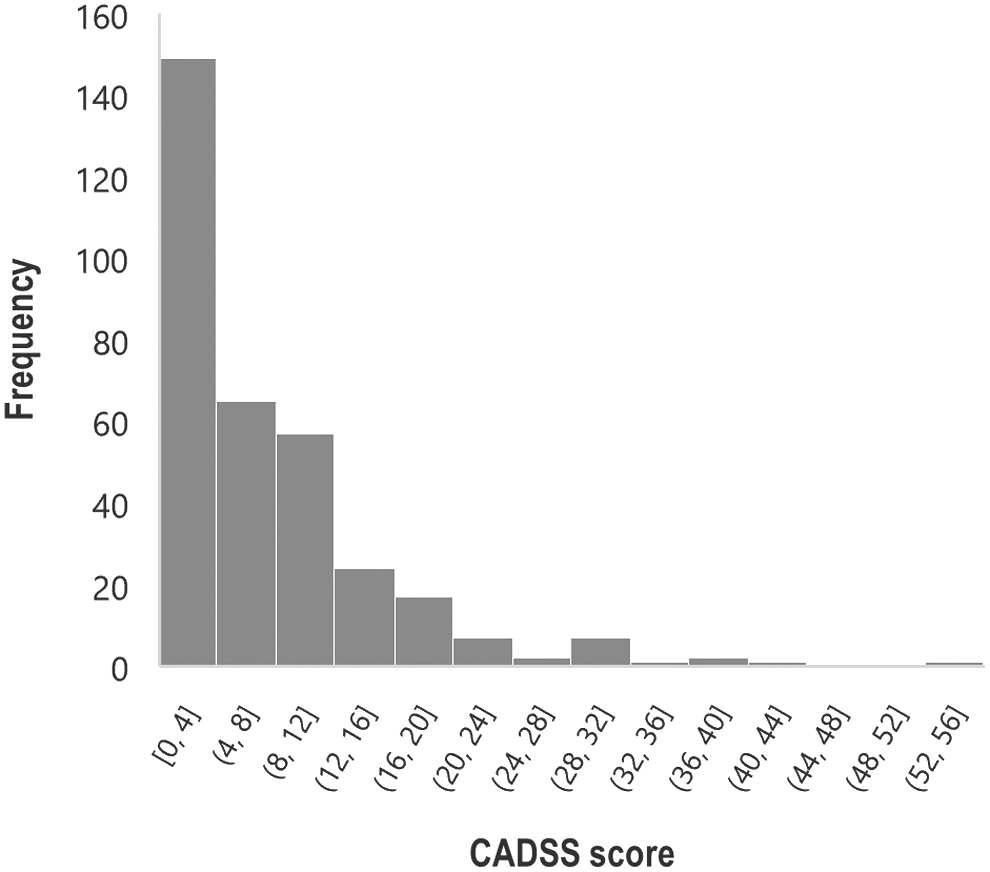
Frequency distribution of CADSS score. CADSS, Clinician-Administered Dissociative State Scale.
Correlation between predictor variables and CADSS score
Participants who reported playing more than 1 hour per session or using apps where they have virtual hands or hand tracking, showed significantly higher CADSS scores, as well as those who reported previous dissociative experiences, traumatic childhood events, avoidant coping strategies, or history of psychiatric disorders, particularly Generalized Anxiety Disorder.
On the other hand, no significant correlation was found between CADSS score and the frequency of VR use, the level of immersion, substance use, and history of neurological disorders.
Independent-samples t-test and Spearman's correlation results are presented in Tables 1 and 2, respectively.
Predictor Variables—Independent-Samples t-Test Results
Present.
Absent.
SD, standard deviation.
Predictor Variables—Spearman's Correlation Test Results
VR, virtual reality.
Impact on mental wellbeing
Only 14.2% of participants categorized the dissociative symptoms as anxiogenic (Fig. 2). Those participants revealed a significantly higher CADSS score (15.74 ± 11.83), when compared with the others (9.39 ± 7.14) (t = 4.115, P < 0.001).
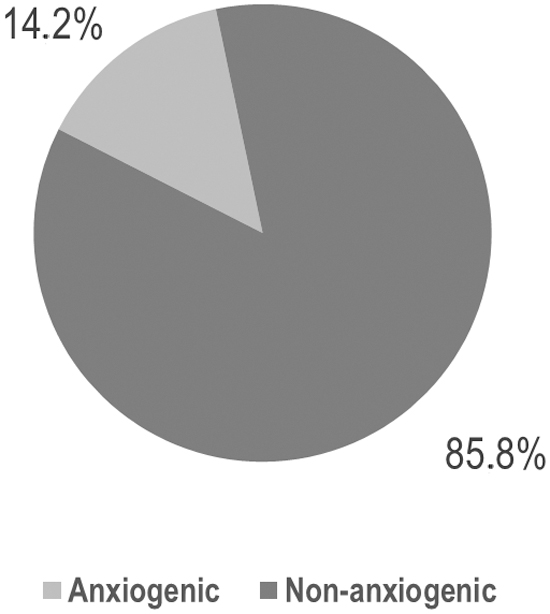
Frequency distribution of symptom-induced anxiety.
In accordance, most participants reported a relatively short symptom duration, with 77.4% of the answers pointing toward “minutes.” Only 0.5% of participants reported long-lasting symptoms (“months”). Frequency distribution is displayed in Figure 3.
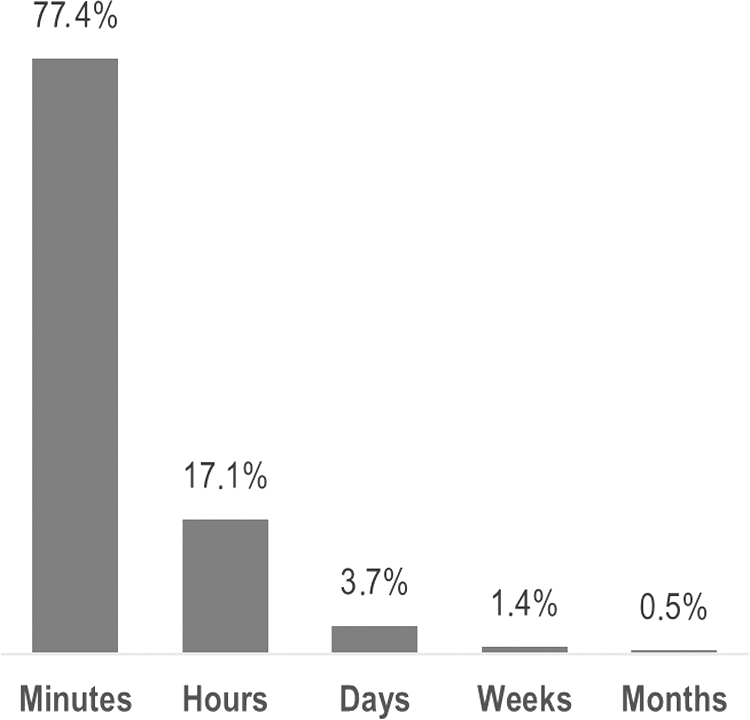
Frequency distribution of symptom duration.
The participants who reported longer symptom duration also revealed significantly higher dissociation scores (rs = 0.150, P = 0.014, n = 217) and anxiety symptoms (G 2 [4, n = 217] = 14.261, P = 0.007.).
Discussion
VR is a rapidly evolving technology that created new horizons for human perception and new ways to challenge our beliefs of what reality is.
Dissociative experiences are a natural aftermath of the increasingly blurred limits between reality and fiction, and they may have unpredictable effects on the users' mental health, calling into question the safety of these devices for the use of the general population.
Therefore, this study had the purpose of testing that safety, under three scopes: determining how prevalent and intense the dissociative symptoms are; studying which variables can trigger or enhance them; and investigating how they affect the users' mental wellbeing.
Prevalence and intensity of VR dissociative symptoms
In line with the initial hypothesis and previous literature, 13 we found a high prevalence of dissociative symptoms among VR users. Even though most participants revealed a relatively low intensity of symptoms, there was still a high variability and range of symptoms among users, which needs to be considered when questioning the safety of VR for the global population.
This variability could be partially explained by the gameplay and individual variables that we studied, and that could help discriminate which players are more susceptible to dissociative experiences.
How gameplay variables impact dissociation
Although most participants revealed a relatively low intensity of symptoms, we found that some gameplay-related variables may influence the intensity of those symptoms: the users who reported playing more than 1 hour per session and using apps that include virtual hands or hand tracking showed significantly higher dissociation scores. This makes sense, since users who spend more time continuously in the virtual world, and who choose games where fake hands' trick the mind just like the “Rubber hand,” 15 are constantly giving their body the visual clues it needs to believe that the virtual environment has some realness to it, while at the same time lacks some of the elements of perception such as touch. This disconnection between visual and tactile signs is known to induce dissociative experiences by altering the perception of the “self.”16–19 Simultaneously, VR also affects the vestibular function, since the visual clues it provides about body position and motion are constantly conflicting with signals from the inner ear regarding the real body orientation. In fact, the vestibular symptoms that it causes are so well known that they have their own name—cybersickness.
The perceptual incoherence arising from the vestibular interpretation is known to distort bodily self-consciousness as well. 20 In fact, dizziness and ear caloric stimulation by themselves are able to induce out of body experiences.21,22 As such, it is expected that the longer the body is receiving these conflicting signals among vision, touch, and vestibular system, the greater the possibility of triggering dissociative symptoms.
On the other hand, the frequency/regularity of VR use and the level of immersion described by the users did not seem to impact the intensity of dissociative symptoms. As for the former, we can hypothesize that the regularity of sessions does not affect perception of reality as much as the time spent in each session because the body gets to readjust to the objective reality between each set. As for the latter, it goes against previous knowledge, since the previous study showed that a tendency toward immersion or absorption is significantly related to the level of VR dissociative symptoms. 13 More studies are needed to clarify this matter.
How individual variables impact dissociation
In line with our hypothesis, we found that participants who had a history of previous dissociative experiences, traumatic childhood events, avoidant coping strategies, and psychiatric disorders showed significantly higher dissociation scores. This comes as no surprise, since all of these are known predisposing factors for DP/DR disorder according to the DSM-V. These findings suggest that people who are at risk for dissociative disorders should be more careful when considering using VR devices, especially for long periods of time.
Nonetheless, it is interesting to notice that the psychiatric disorder that led to the highest post-VR dissociation scores was Generalized Anxiety Disorder. In a time when VR is being increasingly used to provide exposure therapy for anxiety-spectrum disorders,23–25 we can hypothesize that having dissociative experiences (that could themselves be anxiogenic) as a possible side effect of VR therapy, could, in turn, exacerbate the patient's anxiety symptoms.
On the other hand, although we found that there were differences in the dissociation scores of people who use substances or have neurological diseases and those who do not, those differences were not statistically significant.
As for substance use, we hypothesize that maybe more importantly than using drugs or not, is the regularity of that use, which we did not account for, to keep the survey as simple as possible. The timing of the drug use (in relation to the time of the VR session) could also be important. We suggest that future studies further explore this matter.
The lack of correlation we found between dissociation score and the selected neurological diseases might be attributed to the fact that we had a short sample of these patients (n = 28), leading to a lack of statistical power.
Future research should also focus on determining potential variables that protect from dissociation, to help developers and clinicians minimize the risk of dissociative experiences.
Impact of symptoms on mental wellbeing
Even though the prevalence of dissociative symptoms was high among VR users, they did not seem to have a big impact on the subjects' lives, since they were generally nonanxiogenic and short lasting.
Unsurprisingly, participants who reported more intense and longer-lasting symptoms also revealed more anxiety toward those symptoms. Additionally, those who reported a longer duration of symptoms also revealed more intense ones.
This means that individuals who experience the most intense dissociative symptoms also experience them for longer and with an associated feeling of anxiety. Since we proved that users who had predisposing factors for dissociation showed a higher intensity of dissociative symptoms, we can thereby assume that these individuals also have longer lasting and anxiety-inducing symptoms, with potential hazards to their mental wellbeing.
Therefore, individuals who have known risk factors for dissociative disorders should be cautious when using VR, since they are more prone to experiencing symptoms that can jeopardize their mental health.
A limitation of the present study is that it relies on self-report assessment, which we attenuated by removing answers that were contradictory or incoherent. This study also had a time gap that could potentiate a memory bias, since participants reported complex experiences that may have occurred months or even years ago.
We recommend that future studies on this matter should be done in a prospective manner, to avoid the memory bias, and to better study the mechanisms behind dissociative VR experiences and their potential contributes and risks for human health and wellbeing.
Conclusion
With this study, we concluded that although VR has the potential to trigger dissociative experiences, in the majority of cases these are mild, nonanxiogenic, and short lasting, making them apparently innocuous to the user.
Nonetheless, more severe and durable effects can happen in people who have a predisposition for these kinds of experiences. Based on this study's findings, we can infer that besides treating and avoiding preventable risk factors, these people should also focus on playing for shorter periods of time and avoiding apps that include hand tracking or other features that trick the circuits of body perception.
With the ongoing technological evolution, VR will keep challenging our body and mind in unexpected ways. We hope the future will unlock its full potential and open a new chapter in the study of the human mind and how it perceives reality and fiction.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.