
Abstract
Objectives:
Exergaming is promising for patients with heart failure who are less inclined to start or maintain exercise programs involving traditional modes of physical activity. Although no effect on exercise capacity was found for an off-the-shelf exergame, it is important to gain insights into aspects related to costs to develop such interventions further.
Materials and Methods:
In a randomized controlled trial, the Heart Failure Wii study (HF-Wii study), the intervention group (exergame group) received an introduction to the exergame, the exergame was installed at home and help was offered when needed for 3 months. Patients received telephone follow-ups at 2, 4, 8, and 12 weeks after the installation. The control group (motivational support group) received activity advice and telephone follow-ups at 2, 4, 8, and 12 weeks. We collected data on hospital use and costs, costs of the exergame intervention, patient time-related costs, and willingness to pay.
Results:
No significant differences were found between the exergame group (n = 300) versus the motivational support group (n = 305) in hospital use or costs (1-year number of hospitalizations: P = 0.60, costs: P = 0.73). The cost of the intervention was 190 Euros, and the patient time-related costs were 98 Euros. Of the total estimated costs for the intervention, 287 Euros, patients were willing to pay, on average, 58%.
Conclusion:
This study shows that the costs of an intervention using an off-the-shelve exergame are relatively low and that the patients were willing to pay for more than half of the intervention costs. The trial is registered in ClinicalTrials.gov (NCT01785121).
Introduction
Physical activity is important for patients with heart failure because being regularly physically active can reduce cardiovascular mortality and the risk of hospitalization, while improving exercise capacity and quality of life.1,2 Unfortunately, many patients are not meeting the recommended daily physical activity levels.3,4 Alternative forms of physical activity and novel delivery approaches might be needed for patients with heart failure who are less inclined to start or maintain programs using traditional modes of exercise. The World Health Organization has singled out digital innovation as an important component of a broad “systems-based” solution in their Global Action Plan on Physical Activity. 5
As resources are scarce and decisions on priority settings in health care are necessary, it is important to recognize the efficacy and economic impact of digital health technologies.6,7 to inform those decisions. Using telerehabilitation as an addition to conventional center-based cardiac rehabilitation has been proven to be more cost-effective and efficient than center-based cardiac rehabilitation alone. 8 Another study showed that telerehabilitation appears to be as effective as traditional center-based rehabilitation, but less costly for the health care provider. 9 A study in elderly cardiac patients showed that home-based, mobile, cardiac rehabilitation programs were an effective and cost-effective alternative for patients who were not willing to participate in a regular rehabilitation program. 10
Novel digital health technologies, such as mobile apps or exergaming (active videogames that combine gameplay with physical exercise), can provide alternative forms of physical activity for this patient group. A recent randomized controlled trial called, the Heart Failure Wii study (HF-Wii study) 11 tested exergaming with an off-the-shelf product, the Nintendo® Wii™, in 605 patients with heart failure. Although no significant results were found for exergaming on exercise capacity, there were indications of efficacy in individual muscle function groups and in patient-related outcomes.11,12
The HF-Wii study 11 also showed that exergaming was safe and feasible for patients in diverse health care systems and climates. Qualitative interviews 13 confirmed that patients could also experience exergaming as fun and having added value, but patients would like exergaming to be more tailored to their level of physical activity levels, they would like to be able to be able exergame outside and to exergame with others.
To enable the development of future interventions that include (tailored) exergaming, it is important to evaluate the costs of an exergame intervention, time spent by patients on the intervention, what the patients are willing to pay for an exergame intervention, and factors related to the willingness to pay (WTP). 14
Therefore, the aim of this study was to gain insights into aspects related to the costs of an exergame intervention for patients with heart failure and their WTP.
The research questions were as follows:
What are the costs of heart failure hospitalization during the exergame intervention and after 1-year follow-up? What are the direct costs of the exergame intervention? What are the patient time-related costs invested in the exergame intervention? How much are patients willing to pay for an exergame intervention and what are the factors related to their WTP?
Methods
Study information is reported according to the Consolidated Health Economic Evaluation Reporting Standards. 15 Data were collected from as part of the HF-Wii study, the design and primary results of which have been described previously.11,16 In the HF-Wii study, patients were recruited between September 2013 and April 2017 at five university hospitals, three regional hospitals, and one rehabilitation hospital in Sweden, Italy, Israel, the Netherlands, Germany, and the United States. Eligible participants had been diagnosed with heart failure by a cardiologist according to the European Society of Cardiology guidelines. 17 Patients needed to speak/understand the language of the country where the intervention took place. Patients were excluded if they were unable to use exergame due to visual, cognitive, or motor impairment.
Patients were also excluded if they were unable to complete data collection material and if their life expectancy was shorter than 6 months. The study was conducted according to the principles of the Declaration of Helsinki (2008) in accordance with the Medical Research Involving Human Subjects Act. In Sweden, ethical approval was obtained centrally (DNR 2012/247-31). Additional approval was obtained from local review boards (the Netherlands: NL48647.068.14/METC141085; Italy: 0052838/272/UVF/1; Israel: 0022-13-RMC; Germany: S22(a)/2015; the United States: USA_UCI IRB HS# 2016-2955). The trial is registered in ClinicalTrials.gov. To assess the WTP, we included patients within Sweden and additional ethical approval was obtained (DNR 2017/517-32).
Patients were randomly assigned either to a group having access to an exergame intervention at home plus motivational support (the exergame group) or to a control group where patients only received motivational support (the motivational support group).
Exergame intervention group
Patients were introduced to an exergame platform (Nintendo Wii) in a group-based introductory session of ∼2 hours and the exergame computer was then installed at home. They received the exergame platform (Nintendo Wii), including two remote controls and the Wii Sports game. In general, patients were instructed to exergame for 30 minutes a day, 5 days a week. As patients could exergame at any time of the day, patients who were working could exergame outside working hours. This advice was adapted to the individual physical condition of the patient. During the first 3 months after inclusion, patients were contacted by telephone after 2, 4, 8, and 12 weeks by the instructor, who followed a standard script to discuss the frequency of playing or to solve possible problems with the computer game. After 3 months, the active support ended, but patients kept the exergame platform.
Motivational support group
After enrolment in the study, the patients received protocol-based physical activity advice from a heart failure team member (nurse, cardiologist, and/or physiotherapist) to balance for the extra attention in the form of the introduction to the exergame computer given to the intervention group. The control group also received telephone follow-up calls 2, 4, 8, and 12 weeks after randomization, which followed a standard script to discuss their current physical activity. After 3 months, the motivational support ended. Patients were scheduled for study visits at 3, 6, and 12 months.
Outcomes
Hospital use and costs
Members of the research team collected heart failure hospitalizations for each patient from medical charts. The hospital use was registered directly after the active intervention and after 1-year follow-up.
All the centers included in this study were asked to provide the average cost for 1 day of heart failure hospital treatment. All costs are given in Euros (for costs in each country, see the Supplementary Data).
Costs of the exergame intervention
The costs of the exergame intervention are the personnel costs related to: (1) Supervised exergame session at the hospital (2 hours); (2) Exergame activity advice (10 minutes); (3) Installation of the exergame platform at home (1-hour travel and 1-hour visit); (4) Telephone follow-up calls (four calls of ∼15 minutes each). Although the personnel might have been a registered nurse, a physiotherapist, or another member of the HF-Wii research team, in eight of the nine centers, a registered nurse was the instructor, provided supervised exergaming, exergaming advice, and installation at home (for costs in each country, see the Supplementary Data).
Therefore, we choose to apply the salary of a registered nurse in 2021 (including cost surcharge) for personnel costs. Furthermore, the level of the salaries of nurses and physiotherapists is very similar in many countries. Fixed facility costs were omitted due to the large differences in costs in country-specific facilities. The large differences would have skewed the costs and not become relevant for some countries with low facility costs. An additional cost was the Exergame platform used in the study, Nintendo Wii, together with two consoles and the game Nintendo Wii Sports (Fig. 1).

Visual representation of personnel and patient time during the exergame intervention and the willingness to pay.
The indirect costs were not included since these were considered only to be marginal for this population in relation to the exergame intervention, for instance, effect on loss of production or informal care.
Patient time-related costs of the exergame intervention
Patient-related time for the exergame intervention are related to: (1) Supervised exergame session in the hospital (1-hour travel and 2-hour session); (2) Exergame activity advice (10 minutes); (3) Installation of the exergame platform at home (1 hour); (4) Telephone follow-up calls (four calls of ∼15 minutes each); (5) Time for exergaming (Fig. 1). The time for exergaming was the self-reported time during the telephone follow-up. When patients were not reached for telephone follow-ups, diaries were assessed to find the amount of exergaming time.
To estimate the costs of patient time, we used an estimation of leisure time in 2021 defined as 35% of gross wage rate (for costs in each country, see the Supplementary Data). 18
Willingness to pay
The interviews were conducted among a subgroup of the larger HF-Wii study. After the 1-year follow-up, 34 patients in Sweden from the exergame intervention group were invited to be interviewed regarding their WTP for the exergame intervention, of whom 29 agreed. The interviews were structured (Fig. 2), based on an estimated cost of the intervention of 450 Euros, and conducted over the telephone by the second author. This researcher was not part of the HF-Wii research team or the study. On average, the interviews lasted for 12 minutes (range 8–21 minutes).
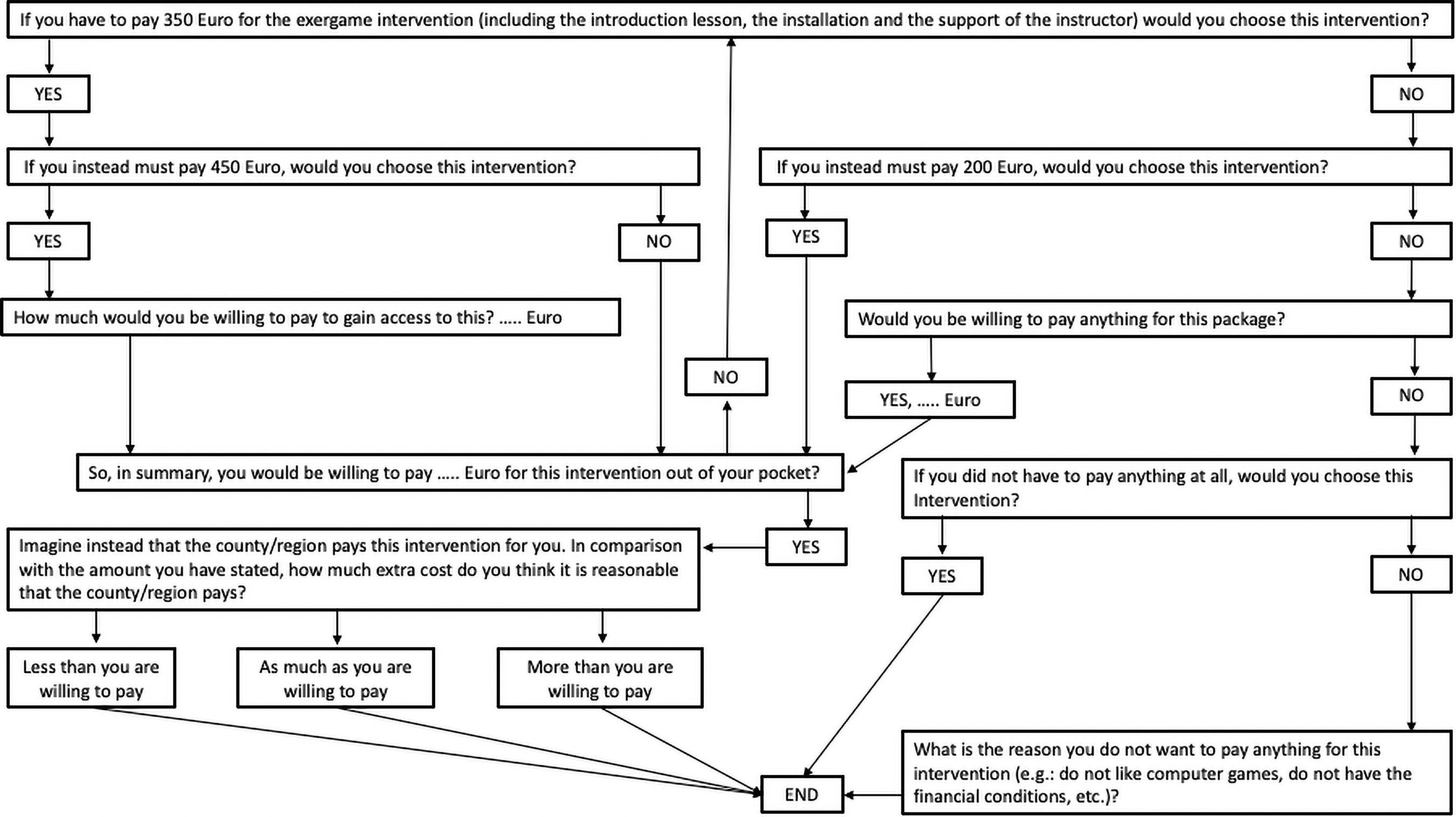
Structured interview guide regarding willingness to pay.
Emotional well-being was assessed using Cantril's Ladder of Life 19 as part of a questionnaire at baseline. Patients rate their current life on a ladder scale in which 0 is “the worst possible life for you” and 10 is “the best possible life for you.” Exercise capacity was assessed at baseline with the 6-minute walk test, 20 in which patients are asked to cover as much ground as possible within 6 minutes according to a protocol developed by the American Thoracic Society. During the interviews, patients were asked for their income and to rate their satisfaction with the exergame intervention on a scale from 0 (not satisfied at all) to 10 (very satisfied).
Statistical analyses
Numbers and percentages were used for categorical variables, whereas mean values and standard deviations (SDs) were used for continuous variables. The normal distribution of the data was tested by the Kolmogorov–Smirnov test. Student t-tests were performed to determine the differences in hospitalization days and hospitalization costs between the exergame group and the group who received motivational support.
Correlations between the WTP and possible related factors (i.e., improvement in exercise capacity, satisfaction level, income, and well-being) were determined using Spearman's rho, and the Kruskal–Wallis test was used to explore how these variables influenced WTP. Satisfaction level was dichotomized into low1–5 and high.6–10 The improvement in distance covered during the 6-minute walking test after 3 months of access to the exergame platform was dichotomized into less than or more than 30 m. Differences in WTP between those with low and high satisfaction level and between those who improved on the 6-minute walking test and those who did not were analyzed using the Mann–Whitney U-test. SPSS Statistics version 26 was used to perform the analyses, and the level of statistical significance was set at α = 0.05.
Results
In total, 605 patients were included in the HF-Wii study, of whom 305 were allocated to the exergame group and 300 to the motivational support group. Patients' mean age was 67 years (±12), 29% (n = 175) were females, and 69% (n = 404) were in New York Heart Association class I or class II. 11
The 29 patients who were interviewed regarding their WTP for the exergame intervention were 68 ± 9 years old, mainly males and married or in a relationship. More than half of them had a university degree, and the mean household disposable income per month in the WTP group was 2800 (±1400) Euros.
Hospitalization costs
No significant differences were found in the number of hospitalizations between the patients who were randomized to the exergame group (n = 305) compared with the patients in the motivational support group (n = 300). A total of 10 hospitalizations due to heart failure occurred during the follow-up period of 3 months: 3 in the exergame group and 7 in the motivational support group, with no significant difference between the groups (P = 0.56). During the follow-up period of 1 year, the exergame group had 18 heart failure-related hospitalizations, and the motivational support group had 26 heart failure-related hospitalizations, with no significant difference between the groups (P = 0.60).
No significant difference in hospitalization costs was found between the patients in the exergame group and the patients in the motivational support group at 1-year follow-up (exergame: median 617 ± 233 Euros vs. motivational support: median 611 ± 234 Euros, P = 0.73).
Costs of the exergame intervention
The exergame platform including the game cost 80 Euros. It required 310 minutes for a research team member to introduce each patient to the exergame in the hospital, perform the home installation, and conduct the telephone follow-ups. In total, these costs amounted to 190 Euros per patient (Table 1).
Costs of Exergame Intervention and Patient Time-Related Costs
Based on the salary + cost surcharge of a registered nurse in 2019.
Based on cost estimation of leisure time.
SD, standard deviation.
Patient time-related costs
In total, patients spent a mean of 300 minutes on the introduction to the exergame platform, installation at home, and the telephone follow-ups. Patients exergamed for a mean of 354 (0–600) minutes during the 3-month intervention (52 of the 305 patients never exergamed). The patient time-related cost was estimated to be 98 Euros per patient.
Willingness to pay
The average WTP for the exergame intervention was 166 Euros (range 0–600 Euros). As the estimated cost of the intervention for the WTP analysis was 450 Euros, on average, patients were willing to pay 37%. After the more thorough analysis of costs, we estimated them to be 287 Euros per patient (Table 1), meaning that, on average, patients were willing to pay 58% of the costs of the exergame intervention.
Satisfaction level regarding the exergame intervention was significantly correlated with WTP (r's = 0.47, P = 0.01). Patients with higher satisfaction levels were willing to pay more (216 ± 170 Euros) than those with lower satisfaction levels (63 ± 75 Euros, P = 0.02). No other variables showed significant correlations with WTP, including income (r's = 0.03, P = 0.89). Some variables tended to correlate with the WTP: having grandchildren (r's = 0.35, P = 0.06), an improved 6-minute walking test (r's = 0.35, P = 0.08), and better emotional well-being (r's = 0.35, P = 0.07).
Discussion
Although we did not find that exergaming increased the exercise capacity of patients with heart failure, previous studies have shown that exergaming is a promising intervention to increase exercise capacity and physical activity levels. To the best of our knowledge, no other studies are available that estimate the cost of exergaming for patients with heart failure. Therefore, we aimed to gain insights into aspects related to the costs of an exergaming intervention. No differences were found in the costs related to heart failure hospitalization between the exergame group and the motivational support group. The costs of the exergame intervention (190 Euros per patient) and patient time-related costs (98 Euros per patient) were low. Patients were willing to pay, on average, 58% (166 Euros) of the costs of the exergame intervention (287 Euros), and patients who were satisfied with the intervention were willing to pay more.
Patients included in this study had, during the follow-up period of 1 year, few heart failure-related hospitalizations (18 in the exergame group vs. 26 in the motivational support group) and thus few hospital days and low costs related to hospitalizations. No significant differences in the number of hospitalization or costs were found between the exergame group and the motivational support group. The low number of hospitalizations could be due to the relatively stable and optimally treated patients with high functional capacity included in this study (the participants had rather low symptom burdens compared with other trials). Future interventions involving low physical activity programs, such as exergaming, should target patients who are inactive, meaning patients who cannot fulfill activity recommendations or those who spend a large amount of sedentary time.
The exergame intervention is a low-cost physical activity program that can be used safely at home for a cost of 287 Euros per patient. This is very low compared with traditional center-based rehabilitation (2395–3446 Euros) or telerehabilitation (1989–2046 Euros).8,9 Studies have shown that telerehabilitation is less costly and just as effective in increasing physical activity in cardiac patients as center-based rehabilitation, or would be a cost-effective addition to it.8,9,21 We should recognize that in this study we omitted the facility costs, due to the large differences between countries. When implementing an exergame intervention in a specific country, these could be added to the total costs of the intervention. Also, the costs of hospitalization, salary of a registered nurse, and patient-related costs differed between the countries included in this study. When implementing an exergaming intervention in a specific country, these costs could differ from the costs presented in this study.
The time that health care personnel had to spend per patient in the HF-Wii study was low: 5 hours and 10 minutes for each patient. For implementation purposes, physical activity programs that place a low time burden on health care personnel are important, especially as many clinics have limited availability of rehabilitation programs or physical activity facilities that are suitable for patients with heart failure. 22 As we did not find any significant effect of exergaming on exercise capacity, 11 future studies should include patients who are physically inactive and could benefit from exergaming, and future studies should develop exergames that can be tailored to patient activity levels (e.g., physical activity level for the exergame can be adjusted to the six-minute walk test outcomes) and preferences (e.g., single play or multi-play; exergaming inside or outside). 23
In this study, we used a relative cheap exergame platform, Nintendo Wii with Sports game, which costed 80 Euros. Other commercial similar exergame platforms are more expensive, for example, the Microsoft Xbox® 360 E Console with Kinect Sensor cost 234 Euros. Development and the regular software update of a new exergame program can be costly. These costs range between 1800 and 7000 Euros, depending on the costs of hardware and software, materials and manufacturing, human resources, marketing, and system maintenance. 24 The costs of the exergame intervention and the implementation of exergaming in practice are low. Mobile applications to increase physical activity in cardiac patients have been shown to be both effective and cost-effective. 10 For these reasons, we believe that tailored exergaming should be developed, preferably as a mobile application.
Patients who reported higher satisfaction levels were willing to pay more for the exergame intervention than those with lower satisfaction levels. Satisfaction with exercise has been shown to be an important factor in physical activity in cardiac patients.21,25 Patients who are satisfied with their exercise experiences during rehabilitation are more likely to engage in exercise after their rehabilitation. 25 Assessing the preferences of patients for the location where they will be physically active could be important because one study 21 showed higher satisfaction with home-based training than center-based training. A possible limitation in the WTP analysis was that that more than half of the patient included in this analysis finished university degree and had an average household income of 2800 Euros (SD 1400). It may be that the results are biased, as patients with a higher education and/or higher salary might be more willing to pay for an exergame intervention compared with patients with lower education or income. However, no correlations were found between these variables and WTP in our analysis.
Footnotes
Acknowledgments
Norrköping: A. Hammarskiold, L. Nestor, C. Norrman, R.M. Petterson, M. Viklander, A. Waldemar, M. Wärfman. Jönköping: J. Mårtensson, E. Lundberg, M. Sahlin, H. Sköldbäck. Linköping: A. Gylling, L. Hjelmfors, M. Huss, M. Jonsson, N.P. Kato, P. Wodlin. Stockholm: E. Hägglund, U. Lennmark. Nyköping: E. Säfström. The Netherlands: J. Boyne, H.P. Brunner-La Rocca, G. Cleuren, M. Spanjers, A. van de Voorde. Italy: R. Corsi, G.A. Ortali, O. Chiala, E. Vellone. Israel: B. Ben Avraham, T. Ben Gal, S. Donanhirsh, Y. Navon, V. Yaari. Germany: A. Hagenow, A. Kuntzsch. USA: J. Ardo, J. Nguyen, M. Cacciata, L. Evangelista. External advisory board: M. Bäck, K. Dickstein, A. Hoes, M.F. Piepoli. Statistical advice: M. Fredrikson, N.P.A. Zuithoff.
Authors' Contributions
L.K.: Conceptualization, writing—original draft, methodology, formal analysis, and writing—review and editing. G.M.: Conceptualization, methodology, writing—original draft, formal analysis, and writing—review and editing. T.J. and A.S.: Conceptualization, methodology, and writing—review and editing. J.A.: Conceptualization, methodology, formal analysis, and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Swedish National Science Council (K2013-69X-22302-01-3, 2016-01390), the Swedish National Science Council/the Swedish Research Council for Health, Working Life and Welfare, VR-FORTE (2014-4100), the Swedish Heart and Lung Association (E085/12), the Swedish Heart and Lung Foundation (20130340, 20160439), the Vårdal Foundation (2014-0018), and the Medical Research Council of Southeast Sweden (FORSS 474681).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.