
Abstract
Background:
Continuous advances in virtual reality (VR) technology have increased its potential for clinical use in the research, assessment, and treatment of mental health difficulties. One potential target for VR use is childhood behavior problems, which are often associated with social-cognitive deficits that can be difficult to measure or modify.
Materials and Methods:
We enrolled 36 boys between the ages of 8–13 to assess the usability of a VR device and its feasibility as a psychiatric tool for youth. Each participant experienced three virtual school cafeteria scenes that varied in antisocial content and the intentions of a virtual counterpart (VC) (control, ambiguous, or hostile). Following each scene, participants completed questions about ease and comfort in using the headset as well as an assessment of hostile attribution bias (HAB). HAB is the tendency to attribute hostile motivations to others' behaviors, which contributes to antisocial thoughts and behaviors. Following this VR use, participants completed a standard text assessment of HAB.
Results:
In general, participants reported the VR headset to be enjoyable and easy to use, and scenes worked as intended, with VCs in the hostile scene rated the meanest. In addition, boys with more conduct problems reported that virtual characters were meaner to them, despite no difference in text vignette measures of HAB.
Conclusion:
This study provides preliminary evidence supporting the further development of VR programs to assess and treat childhood behavior problems.
Introduction
Aggression and behavior problems during childhood accompany a variety of mental health disorders, most notably attention-deficit/hyperactivity disorder, oppositional defiant disorder (ODD), and conduct disorder (CD). In particular, ODD and CD are defined by the prevalence and severity of these sorts of conduct problems in youth. 1 These conduct problems have widespread short- and long-term consequences: victims may be psychosocially or physically harmed; society at large can be disrupted; and perpetrators can be incarcerated, injured, and socially rejected, and have reduced educational opportunities.2–5
One contributor to conduct and aggression problems in childhood is hostile attribution bias (HAB). HAB is the tendency to infer hostile intent to another's actions even when the actual intent is not clear.6,7 HAB draws youth to conflict where there may be no reason for one, such as interpreting a bump from a stranger as an aggressive act, which, in turn, triggers anger and an aggressive response from the child. Compared to youth with low aggression, such bias is most apparent when interpreting “ambiguous” interactions, rather than situations in which others' intentions are clear. 8 Measuring HAB is key to identifying the developmental and environmental factors that affect it, as well as how it can be reduced. HAB has typically been measured by brief text vignettes and follow-up questions. 9
Accurately measuring HAB and other social-cognitive deficits that accompany conduct problems can be difficult, particularly within the real-world contexts in which interpersonal conflicts arise. Parent- or child-report measures are commonly used to quantify problematic thoughts or behaviors related to distinct psychiatric domains,10,11 including specific measures aimed at assessing aggression12,13; empathy 14 ; and callous-unemotional traits. 15 In the laboratory, static facial images, 16 video clips, 17 or cartoons 18 are among the tools employed to measure a variety of social-cognitive constructs underlying conduct problems. Alternatively, measuring reactions to “real” social interactions typically requires the use of confederate(s) in a laboratory setting to mimic real-world situations. This toolset is useful, but incomplete for research settings, as either does not capture thoughts or behaviors as they happen or are a step removed from the experiences and environments in which they occur.
One burgeoning technology platform that holds promise for assessing HAB in a more realistic manner is virtual reality (VR). VR has an advantage over traditional assessment methods because it allows testing to occur in simulated real-world environments where problematic behaviors typically occur (as opposed to unnatural laboratories or doctors' offices), while also maintaining safety and control. Over the long term, this balance of ecological validity and control can enable development of more effective teaching tools to modify HAB and transfer improvements to real-world situations.
However, before its long-term promise can be achieved, we must assess whether the VR program can be used by children, and whether the program can be reliably used to assess HAB. The goal of this investigation was to examine the feasibility of VR to measure HAB in children, by first examining usability and psychological responses during virtual school scenarios that varied in antisocial content and intention (e.g., clearly hostile, ambiguous). We targeted an age range (ages 8–13) during which conduct problems become more prominent, and when characterizing deficits take on greater importance so early, interventions can improve long-term behavioral trajectories.
To this end, we compared boys with low or high levels of conduct problems on their responses to virtual interactions in a school cafeteria. We hypothesized that boys classified as having greater conduct problems would report that virtual counterparts (VCs) were more purposely mean and would experience more negative emotions following virtual encounters, with the largest differences in “ambiguous” situations that are more open to interpretation. We also compared these VR responses to a standard text vignette measure of HAB.
Materials and Methods
Thirty-six English-speaking boys (8–13 years of age), along with their parents (for survey data), were enrolled in this study. Participants were recruited from the community, through paper flyers, word-of-mouth, and email listserv to the local hospital system's employees. These children were required to be free of parent-reported bipolar disorder, any disorder involving psychosis, pervasive developmental disorders, current depression or substance abuse, or any neurological disorder, verified through phone screen and survey responses. As a feasibility study, enrolling only boys allowed us to focus time and resources on developing virtual male counterparts, given the desire to have same-sex virtual interactions to limit response variability.
Visit overview
In-person study visits were conducted in a private laboratory in a rehabilitation hospital. Following informed consent and assent, parents completed a questionnaire outside the room, and the child also completed their surveys before and after experiencing VR scenarios (Fig. 1). Study visits lasted ∼2 hours in duration. Following completion of study procedures, children were compensated $40 and parents $20 for their time. All study procedures were approved by the Indiana University Institutional Review Board.
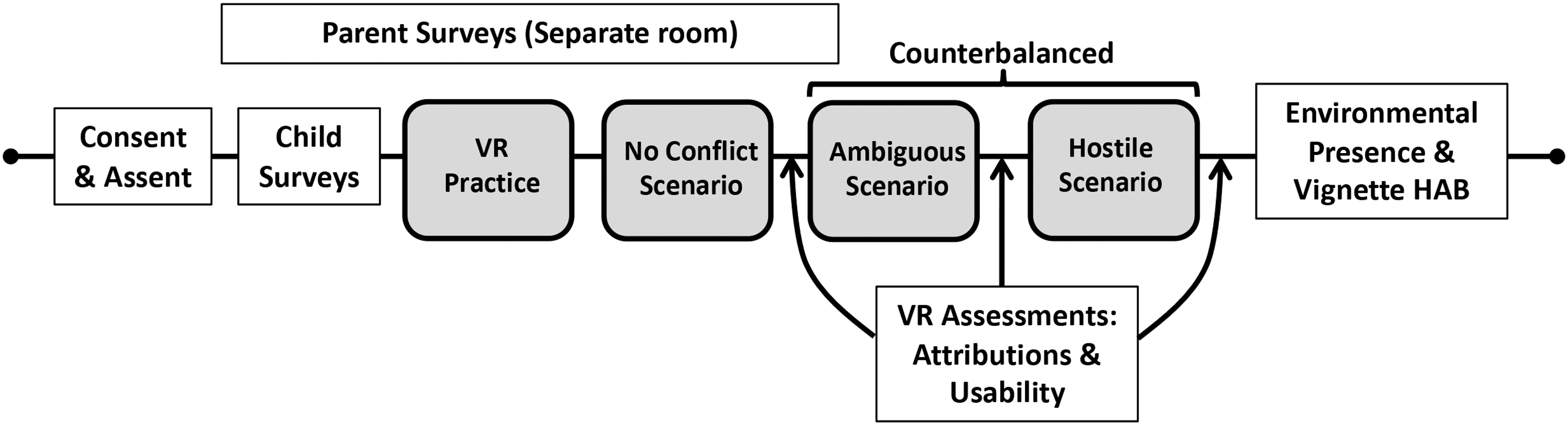
Study design. Participants completed surveys before VR. After each VR scenario, participants removed the headset to answer questions about VR characters and usability of the headset on an electronic tablet. Upon completion of VR scenarios, additional surveys quantified responses to the VR environment and measured HAB through responses to text vignettes. HAB, hostile attribution bias; VR, virtual reality.
Pre-VR questionnaires
Before the VR task, the child and parent completed surveys with an electronic tablet. All survey data were recorded through an online survey system.
Child-completed questionnaires
The aggression scale
This survey measures aggressive behaviors using an 11-item scale (reported Cronbach's α = 0.87). 13 Participants select how many times during the previous week they exhibited a specific behavior or action (7-point scale: 0 times to 6 or more times; e.g., “I got angry very easily with someone.”), with higher scores reflecting greater levels of aggressive behaviors.
The index of empathy for children and adolescents
This tool measures child and adolescent empathy on a 22-item scale (Cronbach's α = 0.68–0.79). 19 Children indicate whether each item is true or false, depending on whether they agree (e.g., “I get upset when I see a boy being hurt”). Higher scores indicate greater empathy.
Past VR exposure
Past VR exposure was measured through several questions asking about the child's technology use. The child indicated whether they had used VR: never (0), 1 time before today (1), 2–5 times before today (2), 6–10 times before today (3), or more than 10 times before today (4). They also indicated specifically whether they had used a full VR headset.
Parent-completed questionnaires
Demographics
The demographic survey allows researchers to gather background data about the parent, child, and household. Specific items within the survey include sex, race, employment, occupation, child's past or current use of services and medication, and information on additional family members in the home.
Behavior Assessment System for Children-2
The Behavior Assessment System for Children (BASC)-2 allows parents to report how often children engage in specific behaviors through a 160-item form. 20 The information from this assessment then allows symptom severity to be quantified along 16 different dimensions, including conduct problems, aggression, and attention problems.
Griffith empathy measure
The Griffith Empathy Measure, which is based on the child-report empathy measure, 19 quantifies the child's cognitive and affective empathy through statements such as “My child becomes sad when other children are sad” and “My child can't understand why other people get upset.” 21 This measure operates through 23 items, which are scored on a 9-point Likert scale, ranging from Strongly Disagree to Strongly Agree (Cronbach's α = 0.81).
VR protocol and questionnaires
VR protocol
Virtual scenarios were presented using an Oculus Rift VR headset (Facebook, Inc., Menlo Park, CA), which includes both head-mounted display and headphones. The headset was connected to an Alienware Aurora R5 computer running 64-bit Windows Enterprise (CPU: Intel i7–6700; GPU: NVIDIA GTX 1070). Oculus Touch hand controls allowed participants to move virtual hands, with thumb-controlled joysticks directing body movement in the virtual world and trigger buttons allowing items to be picked up. Scenarios were programmed with Unity (Unity Technologies, San Francisco, CA).
Subjects remained seated while interacting with the virtual world and used the hand-held controls to move or control objects. Subjects could turn their head to look in any direction in the virtual world. Headphones played auditory stimuli, including background audio recorded from a local middle school. The skin tone of the participant's virtual arms and hands was matched as close as possible (from four options) by the experimenter. This selection was done discreetly by the experimenter, so that the participant was not primed to think about skin color/race during his participation.
VR scenarios
All scenarios took place in an identical school cafeteria environment (Fig. 2). Following a practice scenario, participants were presented with three scenarios. In each, after the subject heard the school bell ring, the goal was to place trash on their cafeteria tray, take the tray to the trash, and empty the tray. Once the task is complete, subjects were allowed to continue exploring the room. Each scenario lasted 3 minutes after the bell rang. The social environments differed in each scenario, creating distinct conditions: No Conflict (baseline), Hostile, and Ambiguous. The No Conflict scenario was always first, while the order of Hostile and Ambiguous scenarios was counterbalanced between subjects.

Virtual cafeteria. All scenarios took place in the same virtual cafeteria. The participant was required to take their tray to the trash can (around the corner that is in middle of left image). In the Hostile scenario (Middle), a single VC purposefully interfered with the participant. In the Ambiguous scenario (Right), a virtual character backs into the participant, with his intent less clear. VC, virtual counterpart. Color images are available online.
During the Hostile and Ambiguous scenarios, a VC interfered with the participant's goal. In the Hostile scenario, a male counterpart menacingly walked toward the participant as he approached the virtual trashcan. When the VC is directly in front of the participant, the participant is frozen in the virtual world, so he cannot escape or move around him. The VC knocks the tray out of the participant's hands and the trash falls to the floor. The VC verbally accosts the participant (e.g., “Hey don't get in my way, you in a hurry or something?!”), and the participant must pick up their items and take them to the trash before time expires.
In the Ambiguous scenario, two virtual characters are standing in front of the trashcan talking with each other about a math test. One of the virtual characters backs into the participant, knocking the tray and items to the floor, looks down at the items (but says nothing), and returns to talking.
VR assessments
After each scenario, children removed the VR headset and completed questions on an electronic tablet, to indicate how mean VCs were (vMean); how mad they would be at these characters (vMad); and usability of the VR headset. A 3-minute rest period was provided before initiation of the next scenario.
VR attribution survey
After each scenario, children responded to questions about the scenario, with a continuous slider that ranged from “No, not at all” to “Yes, definitely.” All continuous scales provided scores from 0 to 100, although numbers were not visible to subjects. These questions asked about their response to characters in the scene and how they would respond if it happened in real life (see Table 1 for all questions), based on prior work measuring attributions and intentions from depicted scenes6,22,23 and designed to quantify a range of responses, in addition to HAB.
Virtual Reality Assessments
VR, virtual reality.
Virtual hostile attributions bias
To quantify HABs, we focused on the VR Attribution Survey question asking how mean users thought the VCs were (“Were any of the characters trying to be mean to you?”). The vMean score was the numeric response to this question. Our other primary measure was how participants would feel if it was a real-life scenario (e.g., “Would you be mad if this happened in real life?”), quantifying the vMad score.
VR acceptability and usability
Subjects also evaluated their physical response to VR (e.g., unwanted side effects) and usability of the VR system (Table 1). Potential side effects were measured with our Child VR Sickness Scale, a version of the Simulation Sickness Questionnaire (SSQ), 24 shortened and modified to be age appropriate. On this scale, children report levels of 12 distinct symptoms (0-None/1-A little/2-A lot/3-Severe; total score could range from 0 to 36). Included in the usability survey were statements informed by the System Usability Scale, 25 aimed at evaluating our team's potential concerns regarding comfort of the headset (e.g., “The headset is comfortable”), ease of controls (e.g., “The controls were easy to use”), and likeability of the VR system (e.g., “I like using the virtual reality headset”), with five possible responses (Strongly Disagree to Strongly Agree).
Post-VR assessments
Environmental presence
After all three VR scenarios and accompanying surveys, children answered questions regarding environmental presence (adapted from Fox and colleagues 26 ) on a continuous 0–100 scale, indicating the degree to which subjects felt they were embodied in a virtual world (e.g., “To what extent did you feel like you were in a real cafeteria?”; Not at all to Extremely; Table 1).
Vignette HAB
Finally, children completed the HAB Questionnaire, 9 which presents 10 unique text scenarios involving ambiguous interactions (e.g., “Imagine that you are standing in the hallway one morning at school. As you are standing there, two kids from your class walk by. As they walk by you, the two kids look at you, whisper something to each other and then they laugh”). For each scenario, children selected from four options (two hostile and two neutral) indicating why an action occurred. Along with this scale, we added a continuous scale after each text scenario asking the degree to which participants believed a counterpart was being purposefully mean and whether they would be mad if the situation happened in real life.
Analysis
Data analysis was performed using SPSS 27.0 (IBM, Armonk, NY). BASC-2 scores for Conduct Problems subscales were converted to T-scores. 20 For group analyses, subjects were split into low/high conduct problems (LCP/HCP) based on a median split of BASC-2 Conduct Problems T-scores. The primary outcome measures were participants' vMean and vMad during each conflict scenario. To quantify these responses, all Hostile and Ambiguous scores were calculated relative to the control scenario (e.g., Hostile—Control; Ambiguous—Control). These scores were assessed by group-by-condition analysis of variance (ANOVA) tests and compared to HAB Questionnaire scores with Pearson correlations.
Usability and environmental presence ratings were also evaluated. Finally, exploratory forward stepwise regression models were performed to identify the best predictors of study withdrawal (logistic regression) and of vMean and vMad scores (linear regression). For these analyses, the best predictors were added to the model one step at a time until no more coefficient was significant at P < 0.05.
Results
Participant overview
Thirty-six boys, 8–13 years of age (mean 11.0, sd 1.4), took part in the study. Subjects were divided into two groups (n = 18 in each group): HCP and LCP, based on parent responses to the BASC-2 survey. The cutoff used for the HCP group was a T-score of 56 or higher, which equates to an approximate percentile of the most severe 20% of boys in the general population.
Four participants did not complete all scenarios due to experiences of VR sickness. These subjects are not included in analysis of vMean and vMad scenario data (see full demographic data for remaining 32 participants in Table 2). Groups did not differ in average age or past VR experience. The HCP group had significantly higher BASC-2 Aggression scores, in addition to the Conduct Problems score, but did not differ in the youth subjects' self-reported empathy or aggression.
Participant Characterization
For Race/Ethnicity, C = Caucasian; AA = African-American/Black; Hisp Ethn = Hispanic Ethnicity.
BASC-2, Behavior Assessment System for Children-2; HAB, hostile attribution bias.
VR scenario fidelity check
Nearly all included subjects completed the goal in all three scenarios within the allotted time (93.75% completion rate). The scenarios also worked as intended, with nearly all participants (96.9%) indicating that someone was mean to them (>50 on 0–100 scale) in the Hostile scenario, with lower amounts in the Ambiguous scenario (25%), and Control scenario (6.2%). All participants indicated a higher vMean rating in the hostile scenario relative to the control scenario.
Attribution bias
Virtual reality HAB
The HCP group reported higher vMean scores compared to the non-HCP group, across both conditions [group main effect: F(1,30) = 4.20, P = 0.049]. The Hostile condition received significantly higher vMean scores across each group [main effect of condition: F(1,30) = 114.63, P < 0.001]. There was no significant group-by-condition interaction [F(1,30) = 0.008, P = 0.92; Fig. 3]. To calculate a total effect size for between-group differences, we averaged the vMean score of each condition, resulting in a Cohen's d of 0.72, indicating a medium to large effect. Participants also reported that they would be madder in real life during the Hostile condition than the Ambiguous condition [Main effect of vMad: F(1,30) = 59.72, P < 0.001].
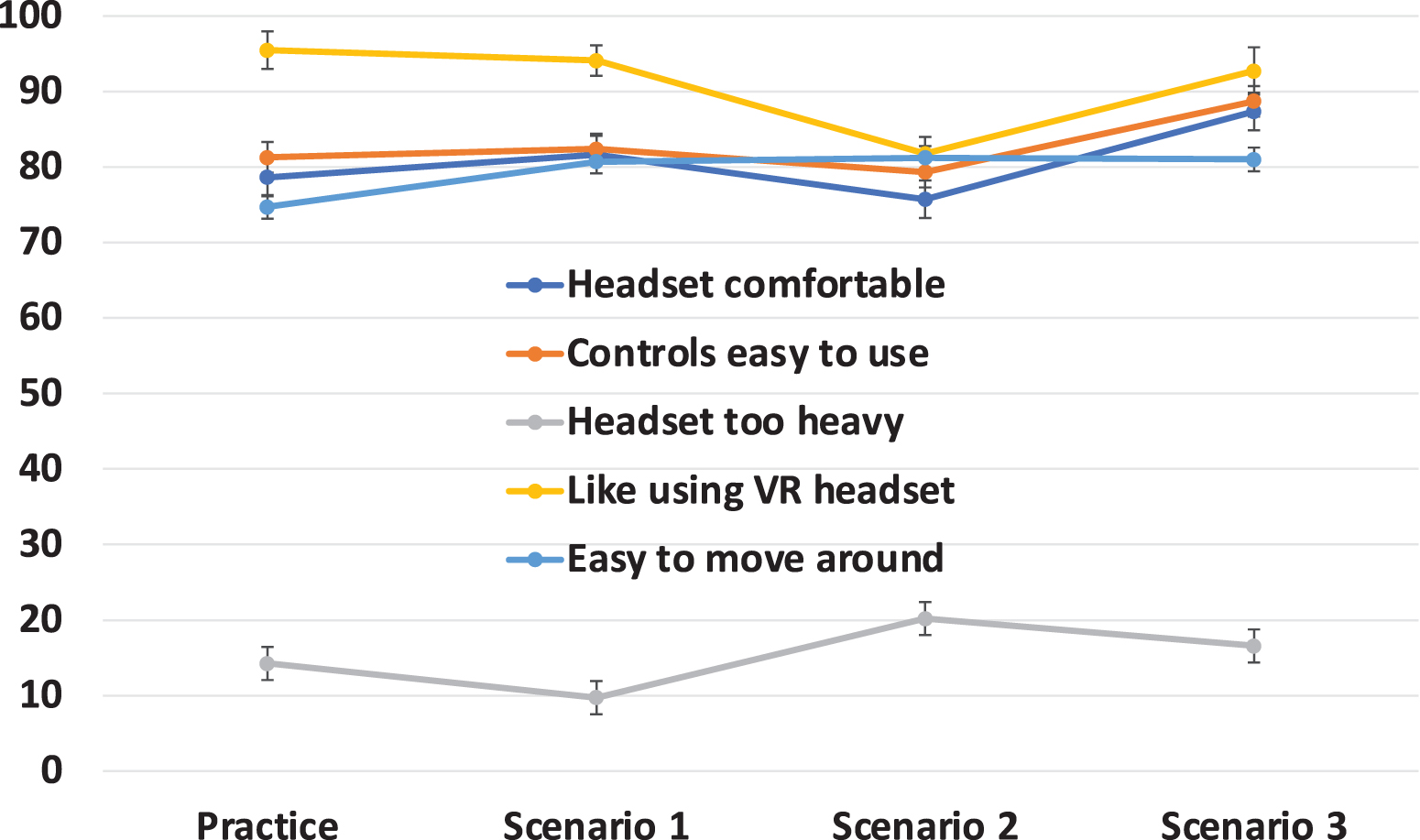
Usability of VR headset. Participants indicated agreement on a 0–100 scale with several statements following each virtual scenario. High agreement was found with positive statements and low agreement with the lone negative statement (“The headset is too heavy.”). Mean ± standard error of the mean scores depicted. Color images are available online.
However, groups did not differ on this score [F(1,30) = 0.63, P = 0.43], and there was no significant interaction [F(1,30) = 0.07, P = 0.79]. Averaged across both conditions, the vMean score was correlated with the vMad score [r(32) = 0.41, P = 0.02] across the entire sample, with a slightly stronger correlation for the Hostile condition [r(32) = 0.43, P = 0.01] than for Ambiguous scenarios [r(32) = 0.37, P = 0.03].
An additional multivariate ANOVA (MANOVA) test with remaining post-scenario VR Attribution Survey measures (see Table 1 for items) similarly found overall effects on condition [F(6,25) = 8.81, P < 0.001], but no group or group-by-condition effects.
Vignette HAB
For HAB measured by text scenarios, overall scores did not significantly differ between groups [t(35) = 0.52, P = 0.61 for all subjects; t(31) = 0.30, P = 0.77 for those completing all VR], nor was this measure correlated with vMean ratings for either Hostile or Ambiguous VR scenarios (for correlations with vignette HAB, raw Hostile and Ambiguous vMean and vMad scores were used, rather than relative to Control, since the vignette HAB has no control scenarios). However, the averaged vMad score was positively correlated with the HAB survey Mad-in-real-life average [r(30) = 0.38, P = 0.04]. The association was stronger with the VR Hostile condition [r(30) = 0.47, P = 0.008] than the VR Ambiguous condition [r(30) = 0.11, P = 0.55]. Thus, emotional responses to virtual and text scenarios were similar when the VR scenarios were hostile.
Finally, exploratory stepwise regression models were employed to identify the best predictors of Hostile and Ambiguous vMean and vMad ratings, with parent-reported empathy, child-reported cognitive and affective empathy, parent- and child-report aggression scores, and summed environmental presence. Parent-reported cognitive empathy was the best predictor of Hostile vMean scores (standardized β = 0.45, P = 0.01), with greater cognitive empathy indicating lower reported vMean. A second regressor, total environmental presence, showed a trend when included in this model (standardized β = 0.32, P = 0.054): greater environmental presence predicted higher vMean score, potentially indicating greater responsiveness to the scenario. No other variable was significantly predictive (P < 0.05) of vMean or vMad scores for either scenario.
VR usability
Overall, the VR system was generally rated to be enjoyable, comfortable, and easy to use (Fig. 4), with high levels of agreement with positive usage statements, and low levels of agreement that “the headset was too heavy.” These scores were relatively stable following each condition, with no significant effect of time. Of note, in their final response to how much “I like using the virtual reality headset,” there was a clear distinction between those who completed and those who withdrew due to VR sickness.
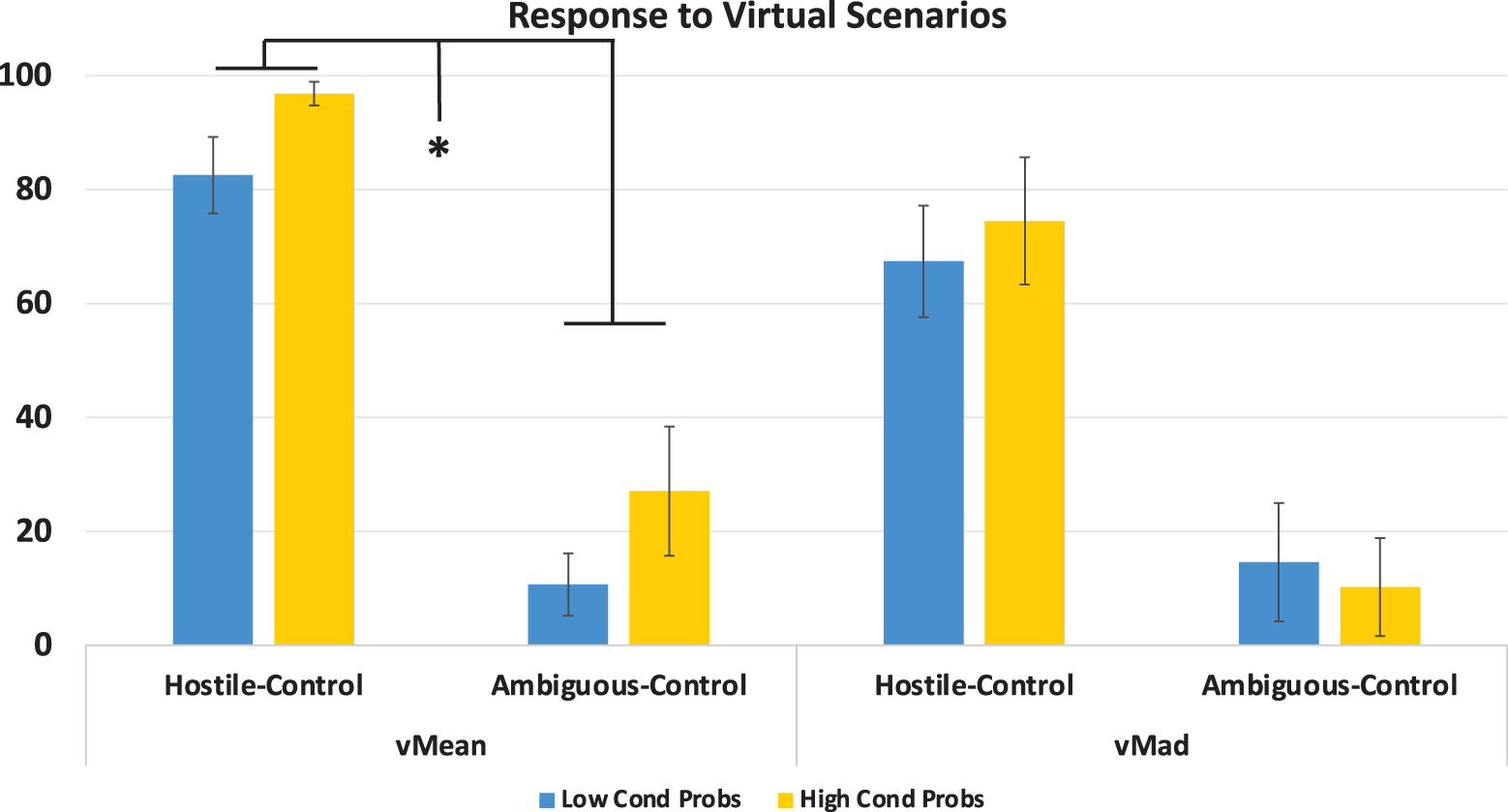
Responses to the virtual scenarios. Mean ± standard error ratings of the vMean and vMad scores for high conduct problem and low conduct problems groups. On continuous 0–100 scales, vMean reflects the participant's judgment of how mean the VC was and vMad reflects their assessment of how mad they would be if the situation happened in real life. Responses were gathered immediately following Hostile and Ambiguous scenarios. *Main effect of group (p < .05). Color images are available online.
Of the 32 who did not withdraw, 72% indicated how much they liked using the VR with the highest rating possible (i.e., 100). There was one outlier who scored 16; remaining scores for the completed subjects ranged between 68 and 100 (median score = 100). Conversely, for the four subjects who withdrew early, final scores ranged between 0 and 33, with a median score of 12.5.
Participants generally reported low incidence of symptoms on the Child VR Sickness Scale [0–36 scale: Post-practice: 2.5 (2.9); Post-scenario 1: 3.2 (3.6); Post-scenario 2: 3.8 (4.4); and Post-scenario 3: 3.9 (4.5)]. These scores trended upward over time, even among those who completed all scenarios [main effect of time: F(3,28) = 2.92, P = 0.051], although there was no difference by group or a group-by-time interaction (P > 0.30). Notably, an exploratory stepwise logistic regression analysis, with the final responses from all Sickness and Usability items, found that two items alone could predict who withdrew: low scores on the Usability question “I like using the virtual reality headset,” and high scores for “Sick to stomach” on the Child VR Sickness Scale.
VR environmental presence
Participants indicated moderate to high agreement that the VR felt like the real world (73.1 on 0–100 scale; sd 32.8); that they were in a cafeteria [70.2 (30.1)]; that they could reach out and touch objects [67.9 (31.3)]; they could explore [59.1 (33.8)]; and that the characters felt real [54.5 (40.0)]. There was lower agreement that they felt like they were in a school [34.9 (33.4)]. There was no significant difference between groups on any of these scores, including the overall summed score (all P > 0.30).
Discussion
This investigation examined the potential for VR to be used in middle childhood to measure HABs associated with conduct problems. Overall, we found that boys with high levels of conduct problems rated virtual characters as meaner than did boys with fewer conduct problems. In addition, we measured broader assessments of feasibility and usability of the VR program and headset in boys, to examine the long-term potential of VR to assess and treat social-cognitive deficits such as HAB. We found that the VR headset was easy for children to use, they enjoyed using it, and the virtual scenarios were generally accurate at depicting the environment and interpersonal interactions as intended.
HAB is widely believed to contribute to antisocial thoughts, feelings, and actions, and the ability to better assess and reduce this bias can help children improve their social behaviors. 27 Prior research has found HAB deficits in youth with conduct problems, particularly those with strong reactive aggression,8,9,28 including youth with ODD and CD. In finding that children with greater conduct problems reported that their VCs were meaner, we provide evidence that these VR scenarios can be a valid way to assess attribution biases that may underlie behavior problems, including aggression. By invoking the cognitive and emotional reactions to virtual situations that align with problematic behaviors, we have an accessible target for instruction or intervention. Further refinement of virtual scenes, as technology continues to improve, can increase the realism of characters and settings, more readily evoking aggressive and disruptive thoughts that therapists aim to assess and ameliorate.
We expected group differences for vMean ratings to be more pronounced in the Ambiguous scenario, when the intentions of the VC were less clear (compared to the Hostile scenario). Instead, on average, the HCP group reported the actions of virtual characters to be meaner than did the LCP group, regardless of whether the scenario was intended to be ambiguous or clearly hostile. To be clear, this finding does not diminish the virtual HAB findings. Rather, the lack of an interaction—with some differentiation during the Hostile scenario—could indicate that the VC in this scenario was not perceived to be unequivocally mean, particularly by those with fewer conduct problems.
Future development and testing can help identify factors that impact the perceived hostility of VCs, including use of tactile stimuli (e.g., vibrations), modifications to VC dialog and actions, or virtual visual or gameplay boundaries that focus more attention on the VC.
In this study, we evaluated HAB with both VR and vignette versions. The VR scenarios may provide a more sensitive measure than the text surveys, possibly due to the more explicit depictions of scenes—in contrast to what we found with VR HAB, when using the traditional text scenarios, no HAB group difference was found. In this sample, with fewer clinically significant impairments, a more sensitive measure may be necessary to detect group differences, which may also explain why we did not find the overall vignette HAB score to be related to VR attribution responses. However, the VR Hostile scenario did elicit a similar emotional response as the Vignette HAB regarding how mad participants thought they would be in real life, which suggests the virtual scenario tapped into anticipated emotional responses in a comparable manner as the traditional text scenarios.
Measuring HAB by VR may alleviate some of the cognitive obstacles (e.g., reading comprehension, theory of mind) present in survey assessments. As such, VR may provide a more accurate indication of HAB, although more technological development and subsequent research and validation are necessary. Because the focus of this study was VR, the text HAB assessments always took place following the VR measurements, which may have impacted responses; future work to compare the two techniques should employ a counterbalanced design. Examining the relative advantages of text versus VR assessments (even beyond HAB) would likewise require larger, more clinically severe samples with both boys and girls, with the incorporation of additional virtual scenarios also likely to be helpful.
Strategies that attempt to reduce HAB have shown some promise29,30 in improving prosocial behaviors, highlighting this social-cognitive deficit as a key target for treatment. One potential avenue to reduce HAB by VR is to improve perspective taking by enabling users to inhabit different sides of virtual interactions such as those presented in this study. Perspective taking is tied closely to cognitive empathy, 31 which was related to VR-assessed hostility in this study. Improved perspective taking (seeing and understanding the world from another person's point-of-view) can reduce HAB by enabling individuals to better understand the intentions of others when disagreements occur. Perspective-taking training programs, conducted by such manners as video modeling, roleplaying, reinforcement, and computer games, have been effective at increasing prosocial behaviors in children and adults.32–36
VR can provide a more efficient, engaging, and less cognitively demanding manner in which to improve perspective-taking, and research has shown promise improving people's ability to understand the perspective of out-groups, such as individuals with different skin tones37,38 or with psychiatric impairments such as schizophrenia.39,40 Boys in this study greatly enjoyed using VR and found it easy to use, which alone are strong points in favor of its use for clinical purposes, as therapists seek ways to engage youth in a productive manner. Importantly, if VR is to be used as part of an intervention, particularly with behavior disorders, short-term interventions are not likely to be successful,41,42 so progress in creating multi-session, adaptive programs is needed.
For VR to continue to progress as a viable psychiatric tool for research, several issues must be addressed and undergo further research and development. First, potential VR sickness may interfere with the ability of some children to use a headset. In this study, we found roughly 10% of children were unable to complete the study due to experiencing nausea or similar symptoms. While some level of nausea may always be present in a minority of individuals, steps can be taken to minimize potential issues, including modifying field of view, improving frame rates, and providing fixed references.43,44
Another challenge is making VR interventions that are targeted to distinct age groups: making content that is engaging and effective to a specified age, while also being cognitively appropriate. For instance, anecdotally, the youngest subjects in this study required more practice, additional instructions, and more help with reading. Care should be taken when designing VR software to alleviate such concerns and enable user-friendly tools (or plan for more adult supervision). The good news is that potential biophysical concerns, such as postural stability and eye problems, do not appear to be an issue, even at younger ages. 45
Next, to maximize the advantages of VR, future development should continue to focus on the realism of characters and the environment, and ongoing technological advancements should help this area. In this study, participants rated character realism to be the lowest dimension of their environmental presence. Since environmental presence did seem to influence the strength of participants' reactions, improvements in realism and presence should bolster the effects of virtual interventions. Prior studies have shown that more realistic avatars and scenes are associated with increased immersion, and thus psychological effects.46,47
Conclusion
This study represents an important step in implementing VR to measure HAB in children, while pointing to potential future applications of VR in clinical pediatric settings. We found that boys 8–13 years of age could navigate a school cafeteria environment and found the VR equipment easy and enjoyable to use. Reactions to virtual interactions reflected a HAB present in boys with higher levels of conduct problems. This presents an exciting avenue for potential VR interventions in this age range, which focus on improving social-cognitive deficits in youth with behavior problems.
Footnotes
Acknowledgments
We thank Michael Conner, Lauren Adams, and Kelsey Hurm for their assistance in recruitment and conducting study procedures. Thanks to Carson Cady and Jordan Poore for help with VR program development.
Authors' Contributions
T.A.H.: conceptualization, methodology, formal analysis, writing—original draft (lead), visualization, supervision, project administration, and funding acquisition; Z.M.W.: conceptualization, methodology, software, resources, writing–reviewing and editing, supervision, and funding acquisition; K.M.: methodology, software, writing–reviewing and editing, and visualization; R.L.M.: formal analysis, visualization, and writing—original draft; J.E.B.: formal analysis, visualization, and writing—original draft; and D.N: conceptualization, methodology, resources, writing–original draft, supervision, project administration, and funding acquisition.
Funding Information
Funding support for project provided by the Indiana University Collaborative Research Grant Fund of the Office of the Vice President for Research. Additional salary support by National Institute of Mental Health award R61MH119291 (all authors). Funding sources had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.