
Abstract
Objective:
Interactive virtual reality (iVR) has been widely used for treatment purposes in patients with chronic musculoskeletal disorders. However, no consensus has been reached on the effects of iVR on pain, psychological distress, and functional disability. Therefore, this study aims to investigate the effects of iVR on pain, psychological distress, and functional disability in patients with chronic musculoskeletal disorders compared with no rehabilitation and conventional rehabilitation.
Methods:
Five electronic databases (PubMed, Cochrane CENTRAL, Scopus, EMBASE, and Web of Science) were searched from January 2016 to December 2021. All randomized controlled trials using iVR for treating pain, psychological distress, and functional disability in patients with chronic musculoskeletal disorders were included. A subgroup analysis was conducted to compare the effects of nonimmersive and immersive types of iVR on the outcomes of interest.
Results:
Our study provides good quality evidence that iVR reduced overall pain by 9.28 points as compared with no rehabilitation and by 8.09 points as compared with conventional rehabilitation. In the subgroup analysis, nonimmersive iVR showed a reduction in psychological distress (standardized mean differences = −0.35) as compared with no rehabilitation. However, no statistically significant difference in the outcomes existed between nonimmersive and immersive iVR. Furthermore, there were no statistically significant differences in the outcomes of functional disability.
Conclusions:
iVR is recommended for reducing pain intensity more than no rehabilitation or conventional rehabilitation. Meanwhile, nonimmersive iVR has been proposed for psychological distress improvement, with effects similar to those of conventional rehabilitation. However, iVR may not be an effective intervention in the case of functional disability.
Introduction
Chronic musculoskeletal disorders affect 20%–33% of the worlds' population, which is the second leading cause of disability. 1 In accordance with the 11th revision of the International Classification of Diseases and Related Health Problems, 2 the definition is a persistent disorder lasting >3 months. Chronic musculoskeletal disorders are typically characterized by chronic pain and functional disability. 3 Moreover, patients with chronic musculoskeletal disorders may experience psychological distress, such as fear avoidance and kinesiophobia.4,5 Avoiding physical movement for a long period of time due to psychological distress can increase the risk of reinjury and other comorbidities.4,5 However, many chronic musculoskeletal disorders can be treated with conventional rehabilitation, such as physical therapy and exercise training.3,4
Conventional rehabilitation has proved that it can reduce pain and functional disability.3,4 The promotion of physical movement is an important component in achieving the goal of decreasing these issues.4,5 Therefore, interventions for reducing pain, psychological distress, and functional disability have recently focused on promoting movement.3–5
Virtual reality is a computer technology that creates a virtual world using graphics and sound effects to replace the surrounding environment. 6 Interactive virtual reality (iVR) is known as an intervention that enables users to interact with objects in the virtual world.7–10 The goal of using iVR is to distract participants' attention from pain and fear by providing a fun and motivating rehabilitation experience.7,8
Users are required to concentrate on their performance through a virtual scoreboard during and after the rehabilitation sessions.7,8 In addition, the immersion and feedback provided by virtual reality can keep participants motivated during rehabilitation. 7 The high level of immersion can provide more motivation than the low level of immersion.9–11 The aforementioned properties of iVR are the explanation of whether iVR is becoming interested in rehabilitation of patients with chronic musculoskeletal disorders.7–14
Patients with chronic musculoskeletal disorders can be treated for their issues by promoting physical movement.3,4 Although previous review studies12–14 have explored the benefits of virtual reality on pain, the control of confounding factors (such as the specification of intervention or the stage of musculoskeletal disorders) has not been demonstrated. Moreover, the impact of iVR on psychological distress and functional disability in patients with chronic musculoskeletal disorders has not been determined. Therefore, this study intends to determine the effectiveness of iVR, as shown in Figure 1. Specifically, this systematic review and meta-analysis aimed to investigate the benefits of iVR on pain, psychological distress, and functional disability in patients with chronic musculoskeletal disorders as compared with no rehabilitation or conventional rehabilitation.
The theoretical framework of the research.
Materials and Methods
Protocol and registration
This study was conducted according to the Prefered Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews.15,16 Moreover, our protocol was submitted to the international prospective register of systematic reviews (PROSPERO), ID: CRD42019122549.
Data sources and search strategies
Five electronic databases (PubMed, Cochrane CENTRAL, Scopus, EMBASE, and Web of Science) were searched from January 2016 to December 2021. A sensitive search strategy was implemented to find randomized controlled trials (RCTs) that used iVR for the rehabilitation of patients with chronic musculoskeletal disorders. The following key terms were used in the search: “virtual reality,” “pain,” “psychological*,” “functional*,” and “musculoskeletal*” (as shown in Supplementary Table S1).
Eligibility criteria
Studies were included according to the following requirements: (1) Population: a RCT of adults (aged >20 years) in which the participants had chronic musculoskeletal disorders. We excluded studies in which the population had acute musculoskeletal disorders or in which the disorder duration was not provided; (2) Intervention: we considered all iVR interventions used to treat patients with chronic musculoskeletal disorders. We excluded studies in which the intervention was passive virtual reality, wherein users passively observe the virtual world without moving or interacting.
We also excluded studies in which the intervention was a combination of iVR and conventional rehabilitation; (3) Comparisons: the comparison groups were no rehabilitation or conventional rehabilitation; and (4) Outcomes: to be included, the study had to use a clinical questionnaire relating to pain, psychological distress, or functional disability. Non-English studies, unpublished articles, and nonoriginal articles were not included in the study.
Study selection and data extraction
After the removal of duplicate studies, two independent review authors screened the articles based on the titles and abstracts. We included studies that met the eligibility criteria and removed irrelevant studies using Endnote reference management. The two independent review authors retrieved and assessed the full text of each study after the screening of the titles and abstracts. The data from the included studies, after screening of the full text, were extracted by two independent review authors using a data extraction table that was agreed upon by the two independent review authors. The baseline and follow-up data for the outcomes of interest were extracted by two independent review authors.
In cases of disagreement on study selection (i.e., data screening and extraction), the third independent review author led a meeting to reach agreement on adjudication. The following information was extracted: (1) first author and year of publication; (2) sample size, patients' age, disease diagnosis, and diagnosis duration; (3) type of iVR, system of iVR, and iVR intervention; (4) iVR duration and iVR frequency; (5) setting of iVR; (6) type of comparisons (i.e., no rehabilitation or conventional rehabilitation) and sample size; (7) outcomes (i.e., pain, psychological distress, functional disability, and other related results); (8) adverse events; and (9) adherence levels.
Risk of bias and quality of evidence assessment
The Physiotherapy Evidence Database (PEDro) scale is a reliable tool for determining the validity of clinical trial methodological quality. 17 We used the PEDro scores from the PEDro database to assess the quality of the included studies. If a study had not been rated in the database, two independent review authors scored it. PEDro scores range from 0 (lowest quality) to 10 (highest quality) (highest quality). Total scores of 8–10 indicate “excellent,” 6–8 indicate “good,” 4–5 indicate “moderate,” and <4 indicates “poor.”
Synthesis of results
The meta-analysis was conducted in Review Manager v.5.3 (RevMan, The Nordic Cochrane Centre, Cochrane Collaboration, Copenhagen, Denmark) to compare outcomes between iVR and comparison groups (i.e., no rehabilitation and conventional rehabilitation). The I2 statistic was used to assess data heterogeneity. 15 Where an I2 of >50% was identified as heterogeneity, the random-effects model was used. On the contrary, where an I2 of <50% was identified as homogeneity, the fixed-effects model was used. When data were presented on the same scale and in the same units, the results were reported as mean differences (MDs) with 95% confidence intervals (CIs). 15
A negative value of MD indicated that iVR had a benefit on pain outcomes. When data were presented on various scales and in various units, the results were reported as standardized mean differences (SMDs) with a 95% CI. A positive value of SMD represented an improvement effect on comparisons (i.e., no rehabilitation or conventional rehabilitation) for psychological distress outcomes, while a positive value of SMD represented an advantageous effect of iVR on functional disability outcomes.
Subgroup analysis was conducted to compare the effects of different types of iVR (i.e., nonimmersive and immersive) on the outcomes of interest (i.e., pain, psychological distress, and functional disability) because different types of immersion had the potential to affect the outcomes. 9 According to immersion, iVR has been divided into two types: nonimmersive iVR and immersive iVR. Nonimmersive iVR is displayed on a monitor or television screen that is smaller than the visual field, such as the Nintendo Wii Fit™. Immersive iVR is projected on a head-mounted display that fills the users' visual field in all directions, such as the HTC VIVE headset.
Results
Study search and selection
A total of 3437 studies were found after searching five databases, and after the removal of duplicates 1661 studies remained. After screening of the titles and abstracts, 89 studies were identified for full-text reviews. We excluded 80 studies from our review because they were duplicates, had a non-RCT study design, were not classified as chronic musculoskeletal disorders, and did not use iVR intervention for rehabilitation. Finally, nine studies18–26 met the criteria for inclusion in this review and were analyzed (Fig. 2).
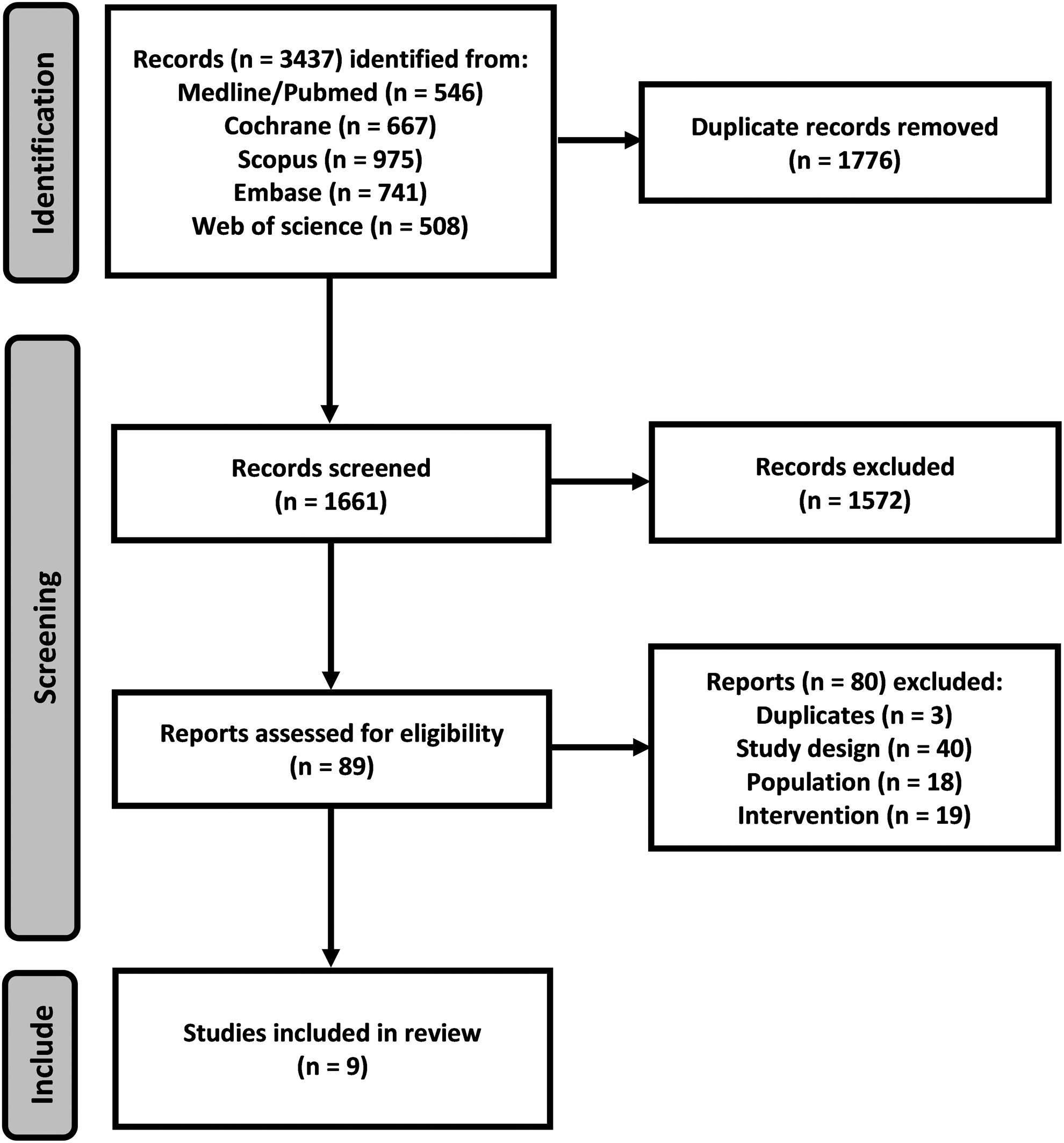
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart showing the study search and selection methods.
Risk of bias and quality of evidence
PEDro scores were obtained from the PEDro database. The included studies' quality scores on the PEDro ranged from 6 to 8 points. The average PEDro score was 6.8, indicating that the quality of the RCTs included in this meta-analysis was good. All of the studies included in this review lacked participant and therapist blinding. The PEDro results are summarized in Table 1.
The Quality of the Included Studies
N, absent; PEDro, Physiotherapy Evidence Database; Y, present.
Study characteristics
A total of 554 patients with chronic musculoskeletal disorders (250 of whom received iVR) were recruited from nine included studies,18–26 published between 2016 and 2021 (Table 2). The ages of the patients ranged from 32 to 68 years (mean of 44.66 ± 11.87 years). The musculoskeletal disorders in the nine included studies were fibromyalgia,18,20,25 ankylosing spondylitis, 19 low back pain, 26 chronic ankle sprain, 21 or neck pain.22–24 The duration of musculoskeletal disorders ranged from 1.5 to 10 years (mean of 5.52 ± 4.50 years).
Summary of the Included Study Characteristics
6MWT, 6-minute walk test; ASQoL, ankylosing spondylitis quality of life; BASDAI, bath ankylosing spondylitis disease activity index; BASFI, bath ankylosing spondylitis functional index; ECUS, eyes closed on an unstable surface; EQ5D, European quality of life-5 dimensions; FAAM, foot and ankle ability measure; FSS, fatigue severity scale; iVR, interactive virtual reality; N/A, not applicable; NDI, neck disability index; NVP, number of velocity peaks; PPT, pressure pain threshold; PSFS, pain self-efficacy questionnaire; PT, physical therapy; TS, temporal summation; TSK, tampa scale for kinesiophobia; TTP%, time to peak velocity percentage; TUG, timed up and go test; VAS, visual analog scale; YBT, Y-balance test.
For iVR, seven studies18–22,25,26 used nonimmersive iVR, whereas two studies23,24 used immersive iVR. The total duration of the iVR interventions ranged from 2.6 to 48 hours (mean of 15.62 ± 15.41 hours). The daily intensity ranged between 15 and 60 minutes (mean of 36.87 ± 19.80 minutes). The frequency of training varied from 2 to 5 days per week (mean of 2.77 ± 1.09 days per week). The training length ranged from 4 to 24 weeks (mean of 8.66 ± 6.32 weeks). The included studies were conducted in clinics,18–20,22 hospitals, 21 laboratories,25,26 and homes.23,24
In terms of conventional rehabilitation, five studies20–24 were conducted on muscle strengthening, balance, flexibility, joint mobilization, proprioceptive exercises, eye-following exercises, kinematic training, and neck exercises. Nonetheless, the total durations, daily intensities, frequencies of training, and training lengths of conventional rehabilitation were the same as those in iVR.
Adverse events were reported in one of the nine studies. 23 Six studies18–21,25,26 found no adverse events, while the incidence of adverse events was not reported in two others.22,24 The adverse events consisted of motion sickness and headaches, which occurred in 5 of the 250 participants (2%) in the iVR group. Meanwhile, the mean adherence level of iVR across nine studies was 93%.
The effect of iVR on pain outcomes
In comparison with no rehabilitation, five studies19,21,23,25,26 with 292 participants (146 of whom received iVR) are illustrated in Figure 3A. In the group that received iVR, the overall pain intensity was reduced by an MD of 9.28 (P < 0.01, 95% CI = −13.96 to −4.60, Z = 3.89, I2 = 0%). In subgroup analysis, nonimmersive iVR reduced pain intensity by an MD of 9.45 (P < 0.01, 95% CI = −14.57 to −4.33, Z = 3.62, I2 = 0%), while immersive iVR did not decrease pain intensity (MD = −8.40, P = 0.15, 95% CI = −19.95 to 3.15, Z = 1.43).

Forest plots showing weighted mean differences with 95% CI in the effect of iVR on pain as compared with:
In comparison with conventional rehabilitation, five studies20–24 with 246 participants (123 of whom received iVR) are illustrated in Figure 3B. In the group that received iVR, the overall pain intensity was reduced by an MD of 8.09 (P < 0.01, 95% CI = −12.42 to −3.76, Z = 3.66, I2 = 16.3%). In subgroup analysis, nonimmersive iVR reduced pain intensity by an MD of 9.75 (P < 0.01, 95% CI = −15.00 to −4.49, Z = 3.64, I2 = 0%), while immersive iVR did not decrease pain intensity (MD = −4.57, P = 0.24, 95% CI = −12.22 to 3.08, Z = 1.17, I2 = 0%).
The effect of iVR on psychological distress outcomes
In comparison with no rehabilitation, three studies18,23,26 with 196 participants (101 of whom received iVR) are illustrated in Figure 4A. In the group that received iVR, the overall psychological distress was not reduced (SMD = −0.27, P = 0.06, 95% CI = −0.55 to 0.01, Z = 1.89, I2 = 0%). However, in a subgroup analysis, nonimmersive iVR was found to reduce psychological distress (SMD = −0.35, P = 0.04, 95% CI = −0.69 to −0.01, Z = 2.03, I2 = 0%). Meanwhile, immersive iVR did not decrease psychological distress (SMD = −0.10, P = 0.71, 95% CI = −0.60 to 0.41, Z = 0.37).

Forest plots showing weighted SMD with 95% CI in the effect of iVR on psychological distress as compared with:
In comparison with conventional rehabilitation, two studies23,24 with 104 participants (52 of whom received iVR) are illustrated in Figure 4B. In the group that received iVR, the overall psychological distress was not reduced (SMD = −0.07, P = 0.73, 95% CI = −0.45 to 0.32, Z = 0.35, I2 = 0%). There was no subgroup analysis because none of the studies included in this comparison were conducted on nonimmersive iVR.
The effect of iVR on functional disability outcomes
In comparison with no rehabilitation, five studies19,21,23,25,26 with 292 participants (146 of whom received iVR) are illustrated in Figure 5A. In the group that received iVR, the overall functional disability was not improved (SMD = 0.17, P = 0.15, 95% CI = −0.06 to 0.40, Z = 1.44, I2 = 0%). In a subgroup analysis, neither nonimmersive nor immersive iVR improved functional disability (SMD = 0.20, P = 0.14, 95% CI = −0.06 to 0.45, Z = 1.48, I2 = 0%; and SMD = 0.07, P = 0.79, 95% CI = −0.44 to 0.57, Z = 0.27, respectively).
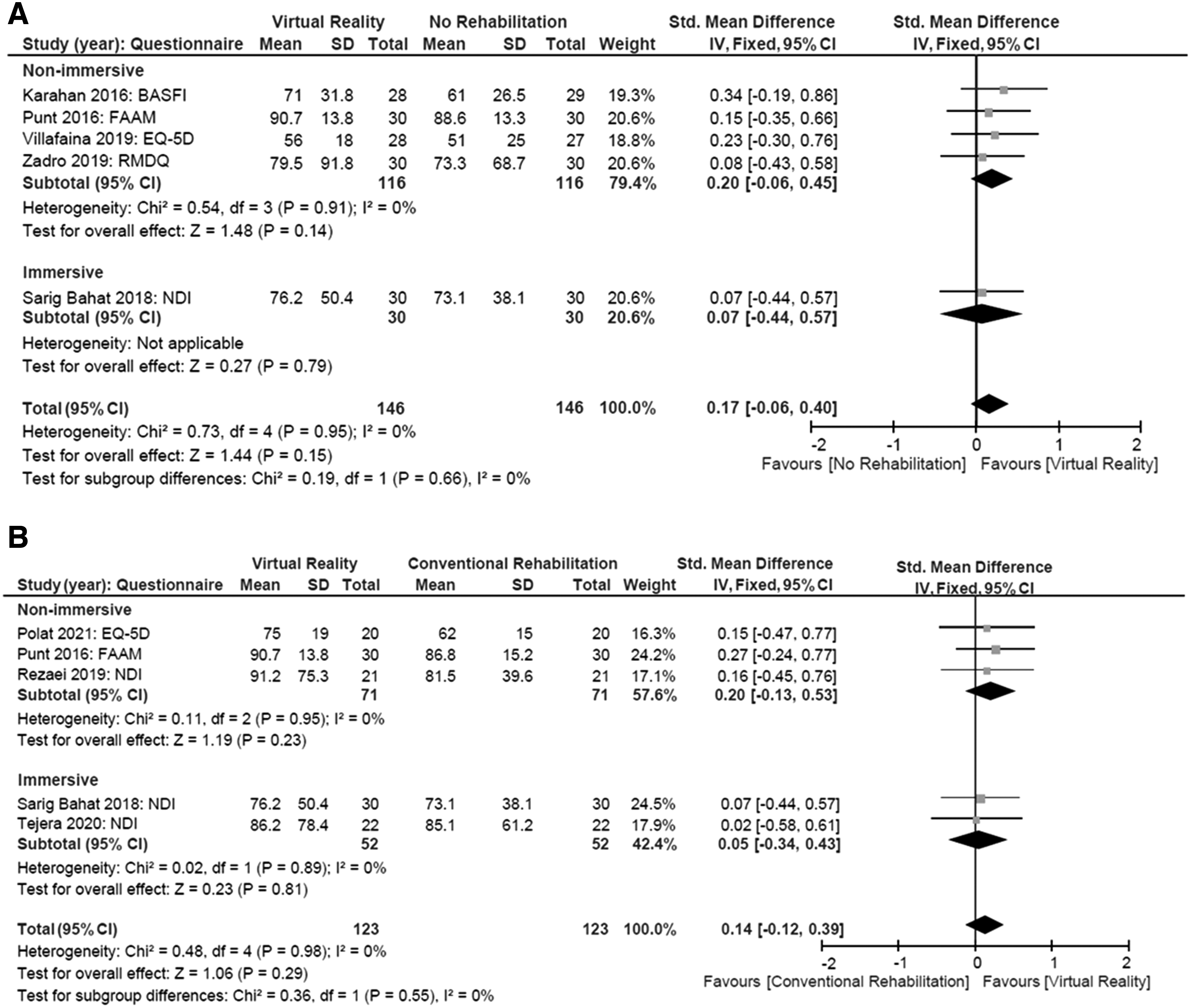
Forest plots showing weighted SMD with 95% CI in the effect of iVR on functional disability as compared with:
In comparison with conventional rehabilitation, five studies20–24 with 246 participants (123 of whom received iVR) are illustrated in Figure 5B. In the group that received iVR, the overall functional disability was not improved (SMD = 0.14, P = 0.29, 95% CI = −0.12 to 0.39, Z = 1.06, I2 = 0%). In a subgroup analysis, neither nonimmersive nor immersive iVR improved functional disability (SMD = 0.20, P = 0.23, 95% CI = −0.13 to 0.53, Z = 1.19, I2 = 0%; and SMD = 0.05, P = 0.81, 95% CI = −0.34 to 0.43, Z = 0.23, I2 = 0%, respectively).
The effect between nonimmersive and immersive iVR
There was no significant difference between nonimmersive and immersive iVR on pain outcomes (in comparison with no rehabilitation: P = 0.87, χ 2 = 0.03, I2 = 0%; in comparison with conventional rehabilitation: P = 0.27, χ 2 = 1.20, I2 = 16.3%), psychological distress outcomes (in comparison with no rehabilitation: P = 0.41, χ 2 = 0.68, I2 = 0%; in comparison with conventional rehabilitation: not applicable), nor functional disability outcomes (in comparison with no rehabilitation: P = 0.66, χ 2 = 0.19, I2 = 0%; in comparison with conventional rehabilitation: P = 0.55, χ 2 = 0.36, I2 = 0%).
Discussion
Our study provides good quality evidence that iVR can improve pain and psychological distress outcomes in patients with chronic musculoskeletal disorders in comparison with no rehabilitation and conventional rehabilitation. According to previous review studies,12–14 the results on pain outcomes were consistent with our findings. However, our study focused on patients at the chronic stage of musculoskeletal disorders. The chronic stage can relatively reduce the effect of self-recovery as confounding factors that affect the outcomes.27,28
Moreover, unlike previous review studies,12–14 our study separated the comparison groups into no rehabilitation and conventional rehabilitation. In addition, previous review studies12–14 did not specifically examine the effect of iVR. Some of the included studies in the previous review involved the combination of iVR and conventional rehabilitation.12–14 Meanwhile, this study intends to investigate the genuine effect of iVR on the outcomes.
Our findings showed that iVR (both nonimmersive and immersive) appeared to reduce pain, while the nonimmersion types of iVR appeared to reduce psychological distress. However, our meta-analysis indicated that iVR may not be an effective intervention for functional disability outcomes. Consequently, we proposed using iVR for pain and psychological distress rehabilitation. Nonetheless, no clear consensus on the use of iVR to improve functional disability was presented in this study.
Our study conducted a subgroup analysis between nonimmersive and immersive iVR. The different types of immersion have been concerned about the potential effect on the outcomes. 9 However, there was no difference in pain or psychological distress between nonimmersive and immersive iVR. It should be noted that part of our analysis was limited due to the small number of studies on immersive iVR. The small number of included studies may have resulted in a lower significant impact on the outcomes between nonimmersive and immersive iVR. Hence, the findings on different types of immersion remain unclear.
Our study is the most current meta-analysis of the effect of iVR on pain outcomes. According to the included studies (since 2016),19–26 after the completion of a rehabilitation session, iVR was found to provide a significant amount of pain relief. Patients with chronic musculoskeletal disorders who suffer from chronic pain frequently complain about avoiding physical movement.4,5,29 The use of iVR can distract patients' attention away from their pain.8,29 The absence of pain can help patients gain confidence in their ability to move around in a virtual world.8,29 Increased physical movement can alter patients' perceptions of pain during rehabilitation.5,29,30 These effects of iVR might be a pain-relieving mechanism in patients with chronic musculoskeletal disorders. 28
In our analysis, two studies18,26 showed that nonimmersive iVR and conventional rehabilitation had the same beneficial effect on psychological distress, as compared with no rehabilitation. Psychological distress is well known to have a positive relationship with pain intensity.29–31 Therefore, a reduction in pain intensity might be associated with reduced psychological distress.29,31 Another explanation is that any type of active physical movement (whether iVR or conventional rehabilitation) can result in changes in psychological distress.3,29,31
Active physical movement can help patients with chronic diseases reduce stress by releasing endorphins. 32 Our findings on reducing psychological distress could indicate that promoting physical movement can have a potential impact on patients' mental systems or perceptions. Thus, iVR has been suggested as an optional or alternative rehabilitation for reducing psychological distress.
Eight of the included studies19–26 indicated that iVR did not improve functional disability in patients with chronic musculoskeletal disorders. The reason is that task-specific training is essential for rehabilitation, neural plasticity, and functional improvement.33–35 It is possible that the studies included in this meta-analysis used nonspecific interventions for rehabilitation.
Six of the included studies18–21,25,26 used ready-made games, while only three of the studies22–24 developed their own iVR for specifying the training protocol. This factor may have played a role in the lower potential to improve functional disability outcomes.33,36–38 Hence, future research should focus on developing specific iVR interventions based on the disorder for effective rehabilitation. Nevertheless, in the included studies of iVR rehabilitation,18,20,22,23 other functional-related outcomes such as gait performance, balance control, muscle strength, and joint movement were reported to improve.
All of the included studies were designed with the same dosages for iVR and conventional rehabilitation. The dosage of the interventions (∼9 weeks, 3 days per week, 36 minutes per day) in this review study is sufficient for improving pain and psychological distress, but it may not be adequate for enhancing functional disability. However, a previous meta-analysis 39 recommended that the dosage of interventions for improving functional disability in older adults should be >150 minutes per week. In our study, we discovered that the average weekly dosage of iVR was <120 minutes. Therefore, the rehabilitation intensity should be >150 minutes per week to improve functional disability, according to a previous study. 39
The enrolled participants in iVR had a consistent intention to participate in and complete the iVR rehabilitation, as evidenced by the high adherence rate (93%). This evidence suggests that an iVR intervention could help patients with chronic musculoskeletal disorders maintain their motivation during rehabilitation. Although our study did not analyze statistical comparisons of adherence levels between iVR and conventional rehabilitation, it is important to consider whether interest in iVR can be maintained by providing a new and challenging task.36,39,40
In addition, a previous study 9 evaluated the effectiveness of different types of immersion on adherence level. Immersive iVR can attract more attention and interest from patients than nonimmersive iVR can. 9 Therefore, future research should consider the type of immersion to keep participants motivated.
The majority of the studies included in this review did not report the incidence of adverse events or reported no adverse events. One study 23 reported motion sickness and headaches, both of which are minor adverse events, in 2% of all included participants. These adverse events have been reported to gradually recover or decrease over time. 23 However, future studies have been suggested to examine adverse events that occur during iVR sessions.
This study had some limitations. First, the outcomes of this meta-analysis were presented as subjectively administered outcomes because some objective outcomes could not be normalized or compared between studies. In addition, the heterogeneity of the outcomes due to the sensitivity and specificity of each assessment should be a concern. Although our study normalized the scores for comparing the effectiveness of iVR, high heterogeneity was still present. Second, some subgroup analysis was not performed in our study due to a lack of data for calculation. The small number of iVR studies makes them relatively underpowered for meta-analysis. The lack of power might explain the nonsignificant findings for iVR.
Third, our meta-analysis was unable to analyze the outcomes using change scores or effect sizes. It was difficult to obtain data that were not available in the published articles. Fourth, this study included patients with fibromyalgia who had hyperalgesia. Patients with high pain sensitivity may respond differently to iVR from those with other chronic musculoskeletal disorders. 41 Finally, since our study was constrained to studies published in English, we may have omitted some recent studies published in other languages.
Conclusions
According to good quality evidence, iVR appears to reduce pain in patients with chronic musculoskeletal disorders. We recommend using iVR (especially nonimmersive iVR) to reduce pain. Moreover, nonimmersive iVR is suggested for reducing psychological distress. The findings were sufficient to conclude that iVR rehabilitation may provide benefits similar to those of conventional rehabilitation in clinics, particularly for the purpose of pain relief. Therefore, iVR can be recommended as an optional or alternative rehabilitation for pain relief and reducing psychological distress in patients with chronic musculoskeletal conditions.
Footnotes
Acknowledgment
We thank Dr. Shwu-Fen Wang for providing a suggestion about a systematic review.
Author Disclosure Statement
The author has no potential conflicts of interest to disclose.
Funding Information
This work was supported by the National Health Research Institutes (NHRI-EX111-11019EI), Ministry of Science and Technology (MOST109-2221-E-002-100-MY3), and National Taiwan University (NTU-CDP-111L7815) awarded to Dr. Wei-Li Hsu.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.