
Abstract
Motivation and adherence are the main factors that limit participation in physiotherapy exercise sessions and airway clearance in cystic fibrosis (CF) population. One of the newly developed techniques is to use virtual reality (VR) games to increase motivation and adherence during exercise sessions for this population. However, this area is still poorly investigated. This review aims to evaluate, summarize, and review published literature regarding the effects of VR exercise on cardiopulmonary function and the use of VR games as a tool for airway clearance technique in CF population. A systematic search was conducted using PEDro, MEDLINE, AMED, CINAHL Plus, and relevant associated keywords. Seventy-three citations were identified from the search, of which 10 were included in this review. Overall, the use of VR was found to have positive effects on cardiac function and improved adherence and motivation during the exercise sessions in people with CF. Incorporating VR into exercise and airway clearance interventions may be beneficial for people with CF. However, further studies with larger sample size and wider range of disease severity are required to be conducted in future.
Introduction
Cystic fibrosis (CF) is a genetic disorder caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene, affecting >70,000 adults, adolescence, and children worldwide. 1 CF affects multiple body regions, but mainly targets the respiratory system and the gastrointestinal system. 2 This therefore leads to infections and progressive inflammatory processes impairing pulmonary function and exercise capacity. 2 Symptoms of CF include wheezing, coughing, shortness of breath (dyspnea), weight loss, jaundice, and diarrhea or constipation, 3 which may affect adults, adolescents, and children with quality of life.
Although there is no cure for CF, certain interventions reduce or delay associated complications. These include antibiotics; inhaled medicines; pancreatic enzyme supplements; CFTR modulator combination therapy; airway clearance techniques (ACT); and pulmonary rehabilitation programs. 4 The new CFTR modulator combination therapy include elexacaftor/tezacaftor/ivacaftor (Trikafta) and this therapy was approved by the FDA for CF treatment in October 2019. 5 Pulmonary rehabilitation programs for CF focus on both resistance and aerobic exercises.6,7 Aerobic exercise contribute to the reduction in dyspnea, improving aerobic capacity and exercise tolerance, improving mucociliary clearance, reducing depression, and improving quality of life.4,7 ACT such as huffing is an essential physiotherapy technique as part of autogenic drainage for children with CF. 4
However, most people with CF do not adhere to both pulmonary rehabilitation, physical exercises, and ACT. 8 Previous studies reported that enjoyment and engagement are the main factors that limit adherence and compliance with physiotherapy programs for people with CF. 9 Other factors include perceptions of physical activity, value attributed to physical activity, and social influences. 10
With the revolution and rapid advancement of technology, games started to take an important role in self-management physiotherapy programs in different populations. For example, virtual reality (VR) games were used as a physiotherapy intervention to improve physical functioning in: stroke survivors 11 ; cerebral palsy 12 ; adults, adolescents, and children with acquired brain injuries 13 ; orthopedic conditions 14 ; cancer 15 ; burn injuries 16 ; people with Parkinson's 17 ; and multiple sclerosis. 18
It is well documented and known that adolescents and children in the general population are interested in different means of entertainment including VR games. 19 Therefore, using videogames to physically challenge children and adolescents with CF might help to increase their motivation and engagement in pulmonary rehabilitation exercises and in ACT. Several studies have investigated the effects of VR physiotherapy interventions for people with CF.20–29 In addition, VR physiotherapy interventions showed that although clinical or community-based rehabilitation might need to purchase the required equipment, it will still be more cost-effective than the supervised traditional physiotherapy sessions.30–32 Furthermore, VR exercises allowed physiotherapy to expand in terms of home-unsupervised rehabilitation programs and hospital-based programs.30–32
However, prescribing exercise using videogames remains challenging in terms of intensity of the game used, type of console used, and accuracy of sensors to movement. Thus, this systematic review aims to evaluate, summarize, and review published literature about (1) the effects of VR exercise on cardiopulmonary function in CF; and (2) the use of VR games as a tool for ACT in pediatrics, adolescents, and adults with CF.
Methodology
Design
A systematic review with quality assessment and narrative synthesis of relevant published literature. The systematic review protocol is registered in the International prospective register of systematic reviews database (PROSPERO) (PROSPERO 2021, CRD42021242496). Outcomes are defined as pulmonary function test (PFT) variables including forced expiratory volume in one second (FEV1) and vital capacity (VC), cardiopulmonary exercise test (CPET) variables including oxygen uptake at maximal exertion (VO2max); oxygen uptake at peak exertion (VO2peak); maximum Heart rate (HR) (HRmax); and peak HR (HRpeak); dyspnea, forced breathing techniques (FBT), motivation, and adherence. The study aimed to conduct a meta-analysis for the outcome measures, where feasible. If conducting a meta-analysis was not possible, the study aimed to conduct a narrative synthesis. PRISMA checklist was used while conducting and writing the systematic review for quality assurance.
Search strategy
A search was completed through EBSCO using the following electronic databases: MEDLINE, AMED, and CINHAL Plus. In addition, the Physiotherapy Evidence Database (PEDro) was used for further searches. The search was limited to full-text English language articles and excluded conference abstracts. The selected databases were chosen because of the likely availability of CF physiotherapy and exercise-related articles. The databases were searched for studies published between January 1, 1970, and April 1, 2022, with results of the searches managed using Endnote Version X7 (Clarivate Analytics, Philadelphia). The Medical Subject Headings (MeSH) were used to allow reproducibility and accuracy of the search. Table 1 summarizes the combinations of keywords included in the search strategies.
Summary of Keywords Used and Search Strategy
To allow reproduction of the results, adapted searches for each database was conducted according to the PRISMA guidelines. Figure 1 is a screen shot of the adapted search for the MEDLINE database.

A screenshot showing MEDLINE separate search as an example about reproducibility of the results.
To have a broader idea about ongoing research, gray literature was explored using the World Health Organization (WHO) International Clinical Trials Registry platform.
Inclusion and exclusion criteria
PICOS system (population, Intervention, comparison, outcome measures, and study design) was used for the inclusion and exclusion. Cross-sectional studies, randomized controlled trials, nonrandomized controlled trials, controlled quasi-experimental studies, and case studies investigating the effects of VR exercise on cardiopulmonary function in CF were included. Studies that did not include either exercise testing, spirometry, motivation/adherence assessment, or breathing control exercises were excluded. Preclinical studies (animal model studies) were excluded (Table 1). Primary outcomes were defined as exercise test outcomes (heart rate, oxygen consumption, distance walked, or workload). Secondary outcomes included number of FBT and FEV1, VC, ACT, motivation, and adherence.
Study selection
Following the search and subsequent removal of duplicates, titles and abstracts were screened by two researchers (M.Z.D., A.A.) for relevance. Full texts of relevant studies were then screened for eligibility against the inclusion and exclusion criteria.
Data extraction
The following data were extracted from the included studies and presented in a table: study design, sample size, sex, age, console used/games used, exercise test utilized, outcome measures reported, and key findings. Where available, frequency, time, intensity, and type of exercise were noted.
Quality assessment of the included studies
Quality assessment of included studies was assessed using the PEDro scale, a valid and reliable tool for assessment of quality of interventional studies specifically related to physical therapy interventions.33,34 Studies with cross-sectional design were checked for quality using the STROBE tool. PEDro scores and STROBE results for the studies were not used as an inclusion or exclusion criterion, but as a basis for best evidence synthesis and to determine the strengths and weaknesses of each study.
Results
The systematic search identified 73 citations, of which 23 were duplicates. Consequently, 50 citations were screened from titles and abstracts and 28 were considered not to be relevant owing to not including participants diagnosed with CF. Of the 22 remaining studies, 12 were excluded because they did not include VR aerobic exercise, VR breathing control, VR exercise, exercise test, or PFT. Consequently, 10 studies were included in the review: 4 studies were cross-sectional-controlled studies; 3 crossover trials; 1 nonrandomized trial; 1 case study pilot trial; and only 1 randomized controlled trial. The randomized controlled trial compared active videogames with traditional patient management. Three studies of the total included studies focused on breathing controlled VR exercise. Figure 2 represents a PRISMA flow chart for the findings of the search. In addition to published studies, two studies were identified from the gray literature search. One of these is a randomized controlled trial, and the other one is a crossover randomized controlled trial.
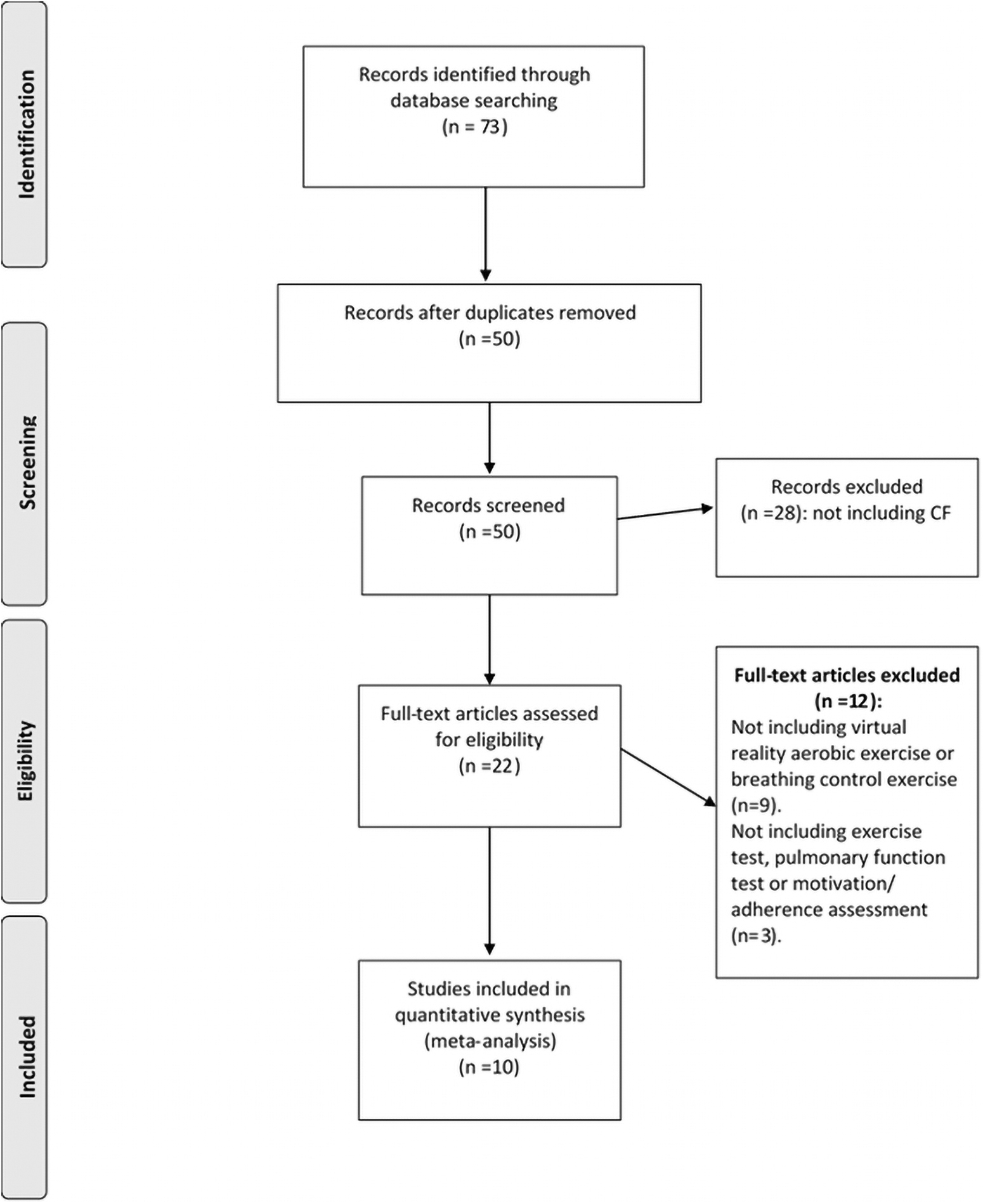
PRISMA flowchart for the search results and the included studies.
Quality assessment
PEDro scores for the five trials ranged from 6 to 9 (Table 2). STROBE results for the included cross-sectional studies are reported in Table 3.
Quality Assessment for the Included Trials
PEDro criteria: 1: eligibility criteria (not used to calculate the PEDro score); 2: random allocation; 3: concealed allocation; 4: baseline comparability; 5: blind subjects; 6: blind therapists; 7: blind assessors; 8: adequate follow-up; 9: intention-to-treat analysis; 10: between-group comparisons; 11: point estimated, and variability provided.
CF, cystic fibrosis; PEDro, Physiotherapy Evidence Database; VR, virtual reality.
STROBE Results for the Included Cross-Sectional Studies
To assess the feasibility of conducting a meta-analysis, data were extracted and summarized in Table 4 and focused on PFT variables; the protocols used for CPET; mode of the test: treadmill, cycle test, or field-based test; CPET test primary outcomes (VO2max and VO2peak); HRmax, and HRpeak. Only one study investigated the effects of VR games on spirometry. Meta-analysis of data was not conducted owing to the heterogeneity of the studies, specifically inclusion/exclusion criteria, exercise test protocol, mode of exercise test (cycle, treadmill, or field-based test), exercise intensity (maximum or sub-maximum), and physiological outcomes (HR, VO2peak, VO2max). Instead, a narrative review was conducted.
Summary of Studies That Investigated the Effects of Virtual Reality Exercise and Breath-Control Exercise on Cardiopulmonary Function and Adherence in People with Cystic Fibrosis
ACT, airway clearance techniques; AT, aerobic threshold; CG, Control group; CI, confidence interval; CPET, cardiopulmonary exercise test; EA, Early Access; EG, exercise group; FEV1, forced expiratory volume in one second; HC, Healthy control; HR, heart rate; MET, metabolic equivalent; MSWT, modified shuttle walk test; MVV, maximum voluntary ventilation; MWT, minutes walk test; PEP, positive expiratory pressure; PFT, pulmonary function test; RCT, randomised controlled trial; RER, respiratory exchange ratio; RR, respiratory rate; SD, standard deviation.
Consoles used and games developed
Four studies used the Nintendo Wii™,23,24,26,27 two studies used the Xbox Kinect™,25,28 and one study used both Wii™ and Xbox™. 22 Games used in these studies included activities like boxing, running, jogging, jumping, dancing, balance, and coordination. The three breath-control studies used spirometers connected to computers.20,21,29 The two unpublished/ongoing trials include both the Wii and the Xbox as part of their interventions.
Key difference between Xbox Kinect and Nintendo Wii is that the Xbox Kinect can recognize voice commands, has voice and facial recognition, whereas Nintendo Wii does not have these features. In addition, Xbox Kinect uses a camera, whereas Nintendo Wii uses a wireless remote controller, and only one Xbox Kinect is needed for multiplayer gaming, whereas in Nintendo Wii multiple Wii remotes are needed. 35
None of the studies reported that the patients have worn VR glasses. All the games in the included studies used 3D environment platforms.
Effects of VR exercise programs on cardiopulmonary function
Heart rate
Seven articles included in the study assessed the effects of VR exercise on HR in CF. VR exercise showed to have similar HR response compared with exercise testing.22–24 Although HR achieved in stationary cycling was higher, HR response in VR training showed acceptable range to the recommended exercise intensity levels (50%–86%). 28 Furthermore, O'Donovan et al 27 reported that HR response in CF was similar to healthy controls in VR training (ranges between 63% and 78% of HRmax). Holmes et al 25 compared VR exercise with CPET and reported that people with CF achieved 86% of their HRmax indicating high intensity achieved. Similarly, Campos et al reported very similar responses in VR gaming between patients with CF and healthy controls. 22 Furthermore, VR training showed similar intensities to aerobic treadmill running and cycling. 26
Oxygen consumption and exercise capacity
When comparing oxygen consumption in different VR games, Campos et al, found that the Summer game for Xbox and the Free Run game for Nintendo Wii had similar responses to aerobic threshold achieved in CPET, indicating the ability to achieve high-intensity training in these games. On the contrary, children with CF achieved lower oxygen consumption while playing the Love Me Again game. 22 When compared with the 6-minute walk test (6MWT), VR training showed higher VO2 levels in CF. 27 Similarly, Del Corral et al 24 reported higher VO2 response in CF who played Wii-Acti and Wii-Train games compared with the 6MWT, but lower levels when playing the Wii Fit game. Moreover, Nintendo Wii Fit Free Jogging game achieved higher VO2 levels compared with Nintendo Wii Sports Boxing in CF. 27
Dyspnea and fatigue
Campos et al reported no significant differences between CF and healthy children who played Wii and Xbox when assessed the subjective sensation of dyspnea (Borg for dyspnea), lower limb muscle fatigue (Borg for leg fatigue) and exertion (OMNI scale). Decreased lower limb fatigue was found after VR training in two studies,25,28 whereas Kuys et al 26 found no change in dyspnea after the VR training. When comparing fatigue between three Wii games (Wii Fit Plus, Wii Active, and Wii Family Trainer), Del Corral et al found no significant differences in dyspnea. 24
Airway clearance/breath-controlled games
FBT and FEV1 was similar in VR training and traditional ACT (for example, huffing; coughing; active cycle breathing technique; or autogenic drainage). 21 However, increased number of minutes played showed significant positive correlation with FEV1. 21 In addition, VC showed similar correlations with the game period. 21 The other two studies did not assess physiological changes, but were case studies to develop and improve the games for future trials. 29 Wetzel et al reported positive feedback for both players (adolescents) who were included with the need for more challenging levels. 29 Moreover, Bingham et al 20 reported that repeated measures analysis of variance of a tracking fidelity statistic showed improvement in eye–breath coordination over five sessions of VR training (P = 0.026).
Motivation and adherence
All studies included reported high adherence to VR training. In 2018, Del Corral et al 23 reported 95% adherence to the sessions in CF who played 6 weeks VR games. Campos et al reported high motivation levels for children with CF who played both Xbox One and Nintendo Wii. 22 Similarly, motivation to VR training was higher than traditional exercise therapy and more preferable for children with CF. 27 In addition, Salonini et al 28 and Kuys et al 26 reported that higher satisfaction level was achieved when exercising with Xbox compared with stationary cycling (when assessed by visual satisfaction scales). Similarly, the three breath-controlled VR training studies reported high engagement and adherence to the interventions,20,21,29 and more minutes were spent using VR training than traditional ACT. 21
Discussion
This review has shown that only a limited number of studies have investigated the effects of VR exercise on cardiopulmonary function in CF, and it has indicated that VR training could help achieve the targeted heart rate needed for this population. VR games are considered to be a cheap, self-management intervention compared with traditional physiotherapy exercise and ACT sessions. However, only one study has assessed pulmonary function using spirometer. In addition, studies included in this review were investigating short-term effects only. Therefore, future studies are recommended to investigate the long-term effects of VR exercise on pulmonary function, with an appropriate calculated sample size and different disease stages. The range of games/levels available also requires consideration to allow exercise prescription for different severities of the condition and to allow more choices for children and adolescents with CF.
In addition, this review revealed that there are three studies that developed VR breath-control exercise games and investigated its effect on respiration, motivation, and adherence. All the 10 studies included showed high adherence and motivation to VR exercise in CF. This finding is important, as adherence is considered the most limiting factor for ACT performance and pulmonary rehabilitation in CF. 9 Patient adherence to recommended self-management interventions such as ACT depends on perceived reward value, which could be achieved through games. In addition, Swisher et al (2008) found that the unpleasantness associated with physical activity outweigh any positive associations in people with CF who do not enjoy physical activity sessions. 36 Thus, VR training might address this problem.
This is the second systematic review addressing the effects of VR exercise on cardiopulmonary function in CF. In 2016, Carbonera et al conducted the first systematic review that included five articles. 37 However, the review excluded breath-control exercise. Thus, this systematic review has run the search again, taking into consideration the fast development of technology and included breath-control VR exercise. In addition, this systematic review included outcomes for cardiopulmonary exercise testing and exercise tolerance in general, PFT, fatigue, motivation, and adherence. Furthermore, this systematic review included 10 studies, compared with 5 studies only for the previous systematic review. Moreover, this review included ongoing trials from gray literature that could give further insights about the future of this field in management of CF.
Limitations of the study
This systematic review is not without any limitation. It was not feasible to conduct a meta-analysis owing to the heterogeneity of the data, different study designs, outcome measures, methods, protocols used in the included studies, and potential for missing unpublished data. In addition, the systematic review included only 10 studies, with only one randomized controlled trial. Accordingly, this systematic review findings need to be further enhanced by running more randomized controlled trials with larger sample size.
Impact
This review summarizes the effects of VR exercises on cardiopulmonary function and increased adherence to aerobic exercise and breath-control exercise in CF. As reported in a previous study that interviewed physiotherapists regarding including VR in their rehab programs, VR helped to improve pediatrics' motivation toward aerobic exercise, but it is still a challenge for therapists to choose the correct game for each specific case. 13 Moreover, taking into consideration the current circumstances regarding the COVID-19 (corona virus disease) pandemic, and for any future unexpected circumstances, physiotherapists started to adapt their programs remotely to continue delivering their programs and to avoid deteriorations in different populations. 38 Subsequently, findings of this review revealed that using VR games may help in airway clearance interventions and cause a positive effect on cardiac function, and improve adherence and motivation during the exercise sessions in people with CF. In addition. This review provides an insight about the importance of further investigating this mode of physiotherapy service delivery in CF in light with the limited number of studies.
Footnotes
Authors' Contributions
M.Z.D. and A.A. were responsible for the data collection, data interpretation, study design, and writing the first draft of the article. S.D. was responsible for revising the article and data interpretation. All authors have participated in editing and completion of the article. All authors have read and agreed to the published version of the article.
Data Availability
All data are fully available without restriction.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.