
Abstract
Introduction:
Fibromyalgia is a complex pain syndrome with high personal and societal costs, with only few effective tools for treatment. Virtual reality (VR) may be an efficient pain management tool although the effectiveness in fibromyalgia patients is unclear.
Objective:
This randomized crossover study set out to 1) investigate the effect of VR on cold pain threshold, -tolerance, and -intensity in fibromyalgia patients and in pain-free individuals and 2) explore the potential relationships between the effect of VR and pain catastrophizing.
Materials and Methods:
Twenty-two female fibromyalgia patients and 22 sex- and age-matched pain-free individuals participated in two conditions (one with VR and one without VR) with foot immersion in 1°C–2°C cold water. The order of conditions was randomized and counterbalanced for each group. Conditions were separated by 20 minutes. Cold pain threshold, -tolerance, and -intensity were assessed during the conditions. Pain catastrophizing was assessed using the Pain Catastrophizing Scale.
Results:
VR induced moderate to large increases in cold pain threshold and pain tolerance compared with the control condition for both the fibromyalgia group and pain-free individuals (P < 0.03). Pain intensity was reduced after VR only in pain-free individuals (P < 0.003). Pain catastrophizing was not related to VR effect on pain threshold, -tolerance, or -intensity for any group.
Conclusion:
VR had a significant effect on pain threshold and tolerance in fibromyalgia patients and pain-free individuals, which supports its ability to distract from pain. Future studies exploring the VR's potential as part of clinical pain management alone or in combination with other treatments are warranted.
ClinicalTrials.gov (NCT04294914).
Introduction
Fibromyalgia is a challenging condition to manage in clinical practice.1–3 So far, no superior treatment strategy exists and a multimodal approach is recommended.4,5 Although the underlying mechanism of fibromyalgia remains an enigma, it has been suggested that altered central processing of nociceptive input may be a contributing factor.1,6 Although studies have found increased pain sensitivity in those with fibromyalgia compared with a pain-free population, the magnitude may be related to the levels of catastrophizing.7–10 Furthermore, levels of pain catastrophizing may mediate pain intensity during physical activity in fibromyalgia. 11
Distraction, defined as the ability to move focus away from pain,12,13 has been shown to reduce pain intensity, increase pain threshold and -tolerance in pain-free individuals.14,15 However, in chronic pain patients, distraction did not have a consistent hypoalgesic effect, 16 which could be related to attentional bias to pain and pain-related cognitions such as pain catastrophizing.17,18 In fact, high levels of catastrophizing may lead to an impaired ability to be distracted from pain.10,19
A treatment modality used to create an interactive distraction from pain is virtual reality (VR), which allows for moving and solving tasks in a predesigned environment. Studies have shown VR being capable of reducing pain intensity, increase pain threshold and -tolerance for the user with the suggested explanation being distraction from noxious input. 20 One study found reduced pain intensity after exercise training with and without VR in fibromyalgia patients, with the largest effect seen for those using VR. 21 However, the previous study did not investigate the immediate effect of VR on pain intensity, -threshold, and -tolerance. Knowledge on how VR may modulate pain in fibromyalgia patients is of great interest if this is to be recommended as part of a pain modulatory treatment strategy, alone, or in combination with other modalities.
The primary aim of this study was to investigate the effect of VR on pain threshold, -tolerance, and -intensity during ice water immersion compared with ice water immersion without VR in fibromyalgia patients and in pain-free individuals. It was hypothesized that VR would reduce pain intensity, increase pain threshold and -tolerance in both fibromyalgia patients and pain-free individuals. A secondary aim was to explore if higher pain catastrophizing was associated with smaller effects of VR.
Materials and Methods
The Consolidated Standards of Reporting Trials of Non-pharmacological Treatments (CONSORT NPT) were used as a guideline for reporting this study. 22 The trial was preregistered at ClinicalTrials.gov, approved by the Danish Data Protection Agency (REG-004-2020) and the local ethics committee (SJ-822). All participants provided written informed consent before commencing the study. The study was conducted at the Multidisciplinary Pain Center in Næstved, Denmark from February 2020 to May 2020.
Design
A within-subject randomized crossover design (VR and control condition [CC]) for the fibromyalgia group and pain-free individuals, respectively, was used in this nonblinded study. All participants participated in one session with two conditions lasting in total ∼50 minutes. The order of the conditions was randomized and counterbalanced for patients with fibromyalgia and pain-free controls. Between conditions there was a 20-minute break (Fig. 1). Before enrolling in the study, all participants had a 3-minute familiarization session to ensure they tolerated the VR experience.
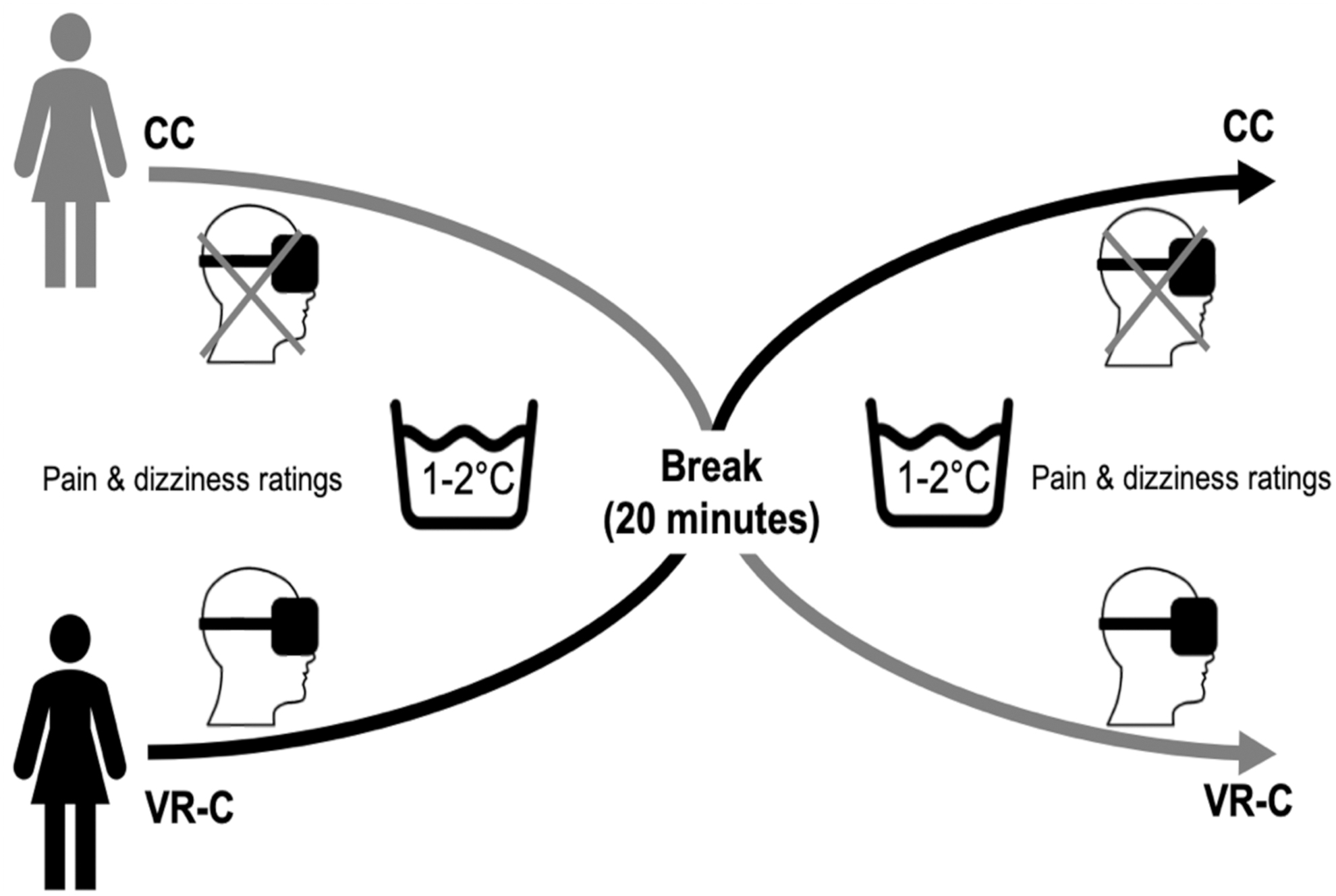
Study overview. Study overview showing the crossover design with the CC and a VR-C during experimentally induced pain (ice water immersion), separated by a 20-minute break. CC, control condition; VR-C, virtual reality condition.
Participants
Twenty-two female fibromyalgia patients with a mean age of 47.6 years (SD 6.6) were recruited from the Multidisciplinary Pain Center in Næstved, Denmark, along with 22 sex- and age-matched pain-free individuals recruited through Facebook adverts seeking healthy participants for a research study. The inclusion criteria for all participants were women 18–65 years old, being able to read, and speak and understand Danish. Participants for both groups were excluded if they were receiving treatment for anxiety, depression, or post-traumatic stress disorder.
In addition, any potential malignant diseases, pregnancy, or conditions impacting on normal sensation in the feet were also cause for exclusion. Fibromyalgia patients had to be diagnosed according to the Criteria for Classification of Fibromyalgia by a rheumatologist23,24 and were excluded if they have had any recent adjustment to their medication such as anticonvulsive, serotonin–norepinephrine reuptake inhibitor or Tricyclic antidepressant. Pain-free individuals were excluded if they experienced any recurrent or ongoing painful condition, whereas slight headaches or any other normal types of unpleasantness commonly reported by the general population were allowed. However, in case of regular use of analgesic medication pain-free individuals were excluded.
Randomization
The randomization of test order, control or VR first, was generated in a balanced way so half of each group would start with the CC before crossing over to the VR condition (VR-C) and vice versa. The randomization was stored in individual sealed opaque envelopes, and after inclusion, participants chose an envelope that determined their test order.
Interventions
For the CC, participants were seated in a comfortable position on a chair with a backrest. From this position they were asked to place their dominant foot into a tub containing ice water (1°C–2°C)25,26 and keep it there until it was perceived as too painful at which time point participants could remove their foot. A maximal duration of the cold pressor test was set to 3 minutes (180 seconds) 27 although this was not communicated to any of the participants to reduce the risk of making the time limit a goal for the participants. The temperature was monitored using a digital thermometer (Vores, Naestved, Denmark) and kept consistent using ice cubes in a separated section of the tub with a pump (Eheim, Deizisau, Germany) ensuring continuous circulation. For the VR-C, the cold pressor task was performed identically with the CC while the participant was exposed to a VR-environment. For the VR-C, an Oculus Rift S VR headset (v.5407469; Oculus, CA) with audio, three motion detectors, and two hand-controllers were used. During the experiment, the VR-software simulated a birthday party. In this nonsocial immersive environment, participants (first-person perspective) were able to move around, see, and use their hands to lighting candles or lift packages from the floor, and so on.
Outcomes
The primary outcomes were cold pain threshold, cold pain tolerance, and pain intensity in the dominant foot. Secondary outcomes were scores on the pain catastrophizing scale (PCS) and dizziness.
Cold pain threshold, defined as the time (seconds) from the participants immerged their foot in the cold water until they started to feel the first sensation of pain 28 was recorded for each condition. Similarly, cold pain tolerance, defined as the time (seconds) from the participants immerged their foot in the water and until they removed their foot due to pain 29 was recorded. Pain intensity in the dominant foot was assessed on a 10 cm visual analog scale (VAS) anchored with 0 as “no pain” and 10 as “maximal imaginable pain”30,31 immediately after each ice water condition (CC; VR-C).
As high levels of catastrophizing may impact the ability to be distracted from pain 32 and thereby the potential efficacy of VR on pain, all participants completed a Danish version of the PCS questionnaire 33 at the beginning of the session. The PCS consists of 13 questions that are answered using a 5-point Likert scale anchored with “Not at all” as 0 and “Very much” as 4, giving a maximal score of 52. 34 Higher scores indicate higher levels of pain catastrophizing.
Dizziness was assessed using a 10 cm VAS 35 anchored with 0 as “no dizziness” and 10 as “maximal imaginable dizziness” immediately before and after each cold pressor condition as this may be experienced by some participants when using VR.36,37 Furthermore, participants were asked to provide information on their age and leggedness, whereas fibromyalgia patients provided the time since receiving their fibromyalgia diagnosis.
Statistics
G*power v3.1.9.4 (Heinrich-Heine-Universität, Düsseldorf, Germany) was used for a sample-size calculation for a paired t-test. A power of 80% and a two-sided significance level of 0.05 was used. Cohen's d of 0.64 was based on a previous study 27 investigating pain threshold during a cold pressor test with and without VR. Based on this, a sample size of 22 was needed for each group. Data distribution was assessed using the Shapiro–Wilk test and the appropriate statistically analysis was conducted.
Main analyses
To investigate the effect of VR in patients with fibromyalgia and pain-free individuals, cold pain threshold, -tolerance, and -intensity were compared between the two conditions (CC and VR-C) using Wilcoxon's tests. Effect size was reported as Eta squared (η 2 ) and interpreted as large (≥0.14), moderate (0.06), and small (0.01) using Cohen's criteria.38,39
Exploratory analyses
To explore the hypothesis that higher pain catastrophizing scores were associated with smaller effects of VR, Pearson's (r) or Spearman's (rs) correlation coefficient analysis (based on data distribution) between PCS scores and change in pain threshold, -tolerance, and -intensity (scores in VR-C minus scores in CC) were conducted. Correlations coefficients were categorized as large (≥0.50), moderate (0.3), or small (0.1) effect sizes using Cohen's criteria.38,39
Finally, to examine if simulator sickness had occurred because of VR, change in dizziness scores over time (pretest and post-test) for the CC and VR-C were compared using Wilcoxon's tests for each group (fibromyalgia and pain-free). All statistical analyses were conducted using SPSS v.27 (IBM, Chicago, IL) and P values of 0.05 or less were considered significant. Data are presented as median and interquartile range (25th and 75th percentile) unless stated otherwise.
Results
A total of 22 fibromyalgia patients and 22 pain-free individuals underwent randomization (Table 1) and completed all conditions with no reported adverse events. Neither group reported any significant dizziness changes during CC (fibromyalgia: pre 0.60 [0.0–3.13] and post 0.55 [0.0–2.63], P = 0.89, η 2 < 0.01; pain-free: pre 0.0 [0.0–0.05], and post 0.0 [0.0–1.0], P = 0.58, η 2 = 0.02) or VR-C (fibromyalgia: pre 0.5 [0.0–2.6], and post 0.55 [0.0–3.38], P = 0.17, η 2 = 0.09; pain-free: pre 0.0 [0.0–0.05], and post 0.00 [0.0–0.08], P = 0.13, η 2 < 0.01). For CC, two fibromyalgia patients (9.1%) tolerated the full 180 seconds of ice water immersion while this was the case for 12 pain-free participants (54.5%). During VR-C, 6 fibromyalgia patients (27.3%) and 20 pain-free participants (90.9%) endured the 180 seconds.
Participant Characteristics for the Fibromyalgia (n = 22) and the Control (n = 22) Group
Data are presented as count (percentage), mean ± SD or median and interquartile range (25th percentile and 75th percentile).
CC, control condition; VAS, visual analog scale; VR-C, virtual reality condition.
Effect of VR on primary outcomes
A large and significant increase in cold pain threshold was observed in the VR-C compared with the CC for both the fibromyalgia group (P < 0.001, η 2 = 0.63; Fig. 2a) and the pain-free group (P < 0.001, η 2 = 0.66). Similarly, higher pain tolerance was found in the VR-C compared with CC for both the fibromyalgia group (P < 0.001, η 2 = 0.50; Fig. 2b) and the pain-free-group (P = 0.028, η 2 = 0.22). The pain-free group displayed a significant reduction in pain intensity after the VR-C compared with the CC (P < 0.003, η 2 = 0.40; Fig. 2c), whereas the fibromyalgia did not (P = 0.231; η 2 = 0.07). Mean difference, SD and 95% CI can be seen in Supplementary Table S1.
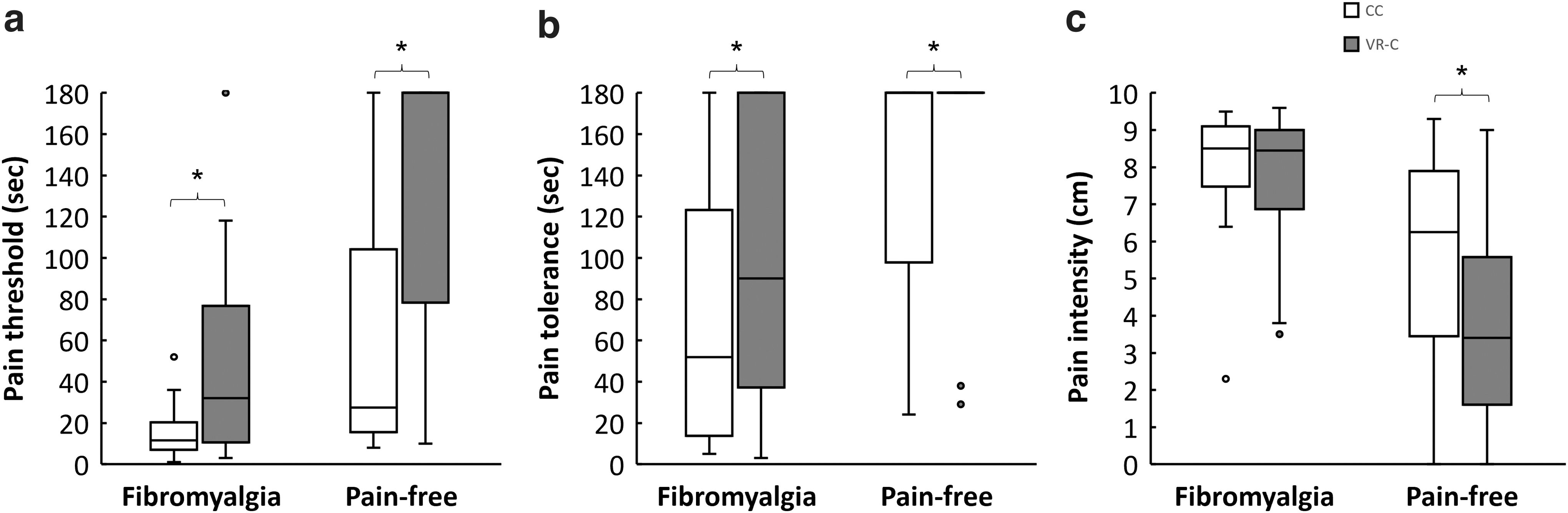
Pain outcomes. Cold pain threshold
Associations between pain catastrophizing and VR effects
No significant correlations between pain catastrophizing scores and effect of VR on pain threshold (fibromyalgia: rs(20) = −0.25, P = 0.27; pain-free: rs(20) = 0.44, P = 0.85), tolerance (fibromyalgia: rs(20) = −0.35, P = 0.11; pain-free: rs(20) = 0.40, P = 0.06) or pain intensity (fibromyalgia: rs(20) = 0.22, P = 0.33 and pain-free: r = −0.36, n = 22, P = 0.99) were observed.
Discussion
The main finding of this study was that VR had large and significant effects on cold pain thresholds and -tolerance in patients with fibromyalgia and moderate to large effects in pain-free individuals. A positive effect of VR on pain intensity was only observed in pain-free individuals. Taken together, the results indicate that VR may have a positive influence on the pain threshold and tolerance and future studies exploring the potential for VR as part of pain management outside a laboratory setting is warranted.
A novel finding of this study is that whereas pain-free individuals reported reduced pain intensity during VR-C compared with CC, this was not seen for the fibromyalgia group. This lack of reduction for pain intensity in the fibromyalgia group is somewhat surprising as the existing literature suggests that using VR should lower pain intensity by distracting the user from pain, which has recently been shown in both persistent painful conditions such as chronic low back pain 40 as well as in experimental pain in healthy populations.27,41–44 One explanation could be that even though distraction, in this study by using VR, can be used to divert from experimental pain20,45 the fibromyalgia group may not have the same beneficial effect as the control group. 46 The reduced ability to be distracted could be impacted by the level of pain intensity experienced by the fibromyalgia group compared with the control group before the two conditions. The underlying mechanism here might then be a potential lack of attentional resources for other tasks, such as engaging with the VR experience, as pain itself draws on attentional resources and the level of perceived threat by pain may play an important role in this. 47 Although some studies suggest that distraction from pain may not be impaired in patients with fibromyalgia compared with pain-free controls,48,49 there is also evidence suggesting the opposite. In contrast to the current findings of no correlation, one study indicated that not only is the ability to distract from pain, measured as reduced pain intensity in fibromyalgia patients compared with pain-free controls, impaired but it is also associated with pain catastrophizing. 10 It has been hypothesized that the difficulty to disengage from pain using VR can be driven by pain-related cognitions (e.g., pain catastrophizing 50 ) that may have affected the VR-induced hypoalgesia. This is supported by a previous study 19 where participants with high pain catastrophizing had reduced analgesic effect of distraction initially but not over time. Although this study did not show any significant impact of pain catastrophizing on neither pain threshold, -tolerance, or -intensity, the current findings are in line with a recent study in individuals with chronic low back pain, which found no moderating role of pain catastrophizing on the effect of VR on pain. 40
Clinically, the aim of pain management for patients with fibromyalgia is to achieve their valued life goals, often through involvement in exercise programs. However, despite exercise training showing positive effect on pain over time51,52 adherence to such programs may be limited due to increases in pain after exercise. 53 A recent study showed pain reduction over time after exercise training with VR that was larger than without VR although this was nonsignificant. 21 In addition, Polat et al 21 found a significant increase in cardiovascular performance and reduced fatigue when compared exercise training without VR, which they argued could be due to decreased perception of pain. This is supported by the current results where both pain threshold and -tolerance was increased although no immediate effect was seen for pain intensity in the fibromyalgia group. Taken together, our results show that VR can modulate pain and if used in combination with exercise as in the previous study, 21 this could make exercise more tolerable to a fibromyalgia population, which in turn may increase adherence to exercise training. However, future prospective randomized controlled studies are needed to investigate the feasibility of using VR in both a clinical setting as well as for self-management in combination with exercise.
Limitations
There are several limitations that need consideration when interpreting the results of this study. This study only included women and the results may not generalize to men.
The current results were based on experimental pain and the VR effect on clinical fibromyalgia pain remains unclear. Furthermore, this study did not consider the potential influence of where pain fibromyalgia patients perceived their pain.
A major limitation in this study is the high number of participants who reached the cold pressor time limit of 180 seconds, which could potentially influence the true effect of VR on pain tolerance and pain intensity. Owing to the proportion of participants reaching the limit of 180 seconds strongly suggests that tolerance results should be interpreted with caution. This ceiling effect indicated that participants in both groups achieved an adaptation to the cold water even though actions were made to minimize this. The maximal limit of time in the cold water was set to 180 seconds. Some studies have used a maximum limit of 5 minutes,27,54 which could have caused less participants reaching the maximal tolerance time in this study. In addition, assessing pain threshold may have affected the distractive effect of VR as participants had to identify when they first experienced pain, 55 which could have been avoided by only recording tolerance values. However, as discussed earlier, the tolerance values have their own limitations. Furthermore, it is recommended to include both pain tolerance and threshold as one assesses the ability to discriminate nociceptive input, whereas the other represents the willingness to endure additional pain. 56
In this study, there was no assessment of the level of immersion with VR or if this was related to the duration of ice water submersion nor was the amount of body movement tracked, both of which has the potential to influence the results and future studies should include these parameters. Another potential limitation is that the CC did not employ a true control (e.g., inactive VR) and this could potentially have caused an overestimation of the VR effects. Furthermore, this study did not investigate the effect of VR on clinical pain; therefore, the results may have limited ecological validity and cannot be directly translated into treatment effects and future studies are needed to clarify this issue. The clinical transferability is further compromised by pain was only assessed immediately after the VR intervention, and not over a longer postintervention period which would be of clinical relevance. Finally, although the hypotheses were not reviled to the participants (e.g., VR was expected to increase the pain threshold and tolerance), it is possible that the lack of participant blinding to VR-C and CC might have influenced the results in case participants expected positive effects from VR.
Conclusion
VR had large positive effects on cold pain thresholds and pain tolerance in patients with fibromyalgia and pain-free individuals. For pain intensity a large positive effect of VR was seen for pain-free individuals but not fibromyalgia patients. No association was shown between pain catastrophizing and the effects of VR on pain threshold, -tolerance, or -intensity. Future prospective studies exploring the feasibility and immediate effect of VR as part of clinical pain management for people with fibromyalgia is warranted.
Footnotes
Acknowledgments
Authors' Contributions
H.A., T.S.V., H.B.V., and S.W.M.C. developed the idea and methods used for the current project. H.A. and T.S.V. collected data. All authors contributed to the data analysis and interpretation as well as preparing the article.
Author Disclosure Statement
S.W.M.C. has received support from the Fund for Research, Quality and Education in Physiotherapy Practice (Fysioterapipraksisfonden) and the Lundbeck Foundation for Health Care Research within the past 5 years. The funders did not have any role in this study. There are no actual or potential conflicts of interest for any of the other authors.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.