
Abstract
Background:
Adolescents frequently experience high levels of anxiety and stress, which can impede quality of life and academic performance. Boxing as a form of exercise has been shown to have mental health benefits in adults.
Methods:
This study investigated the impact of boxing exercise with a virtual reality (VR) game vs. with a guided video on anxiety, stress, and executive function in adolescents. Participants were randomly assigned to 1 of 3 cohorts: Oculus Rift BOXVR game (n = 14), boxing with a guided workout video (n = 14), or a non-intervention control (n = 14). The BOXVR and guided video groups participated in 10-minute exercise sessions, 5 times a week for 3 weeks.
Results:
The groups were comparable at baseline on all outcomes. Only BOXVR participants exhibited a significant (p < 0.001) reduction in stress and significant improvements on the Trail Making Test (TMT) B at weekly checkpoints and follow up. All cohorts showed improvements in executive function on the TMT A. At the end of the study, the BOXVR group reported significantly lower stress levels than the guided video group, and significantly better TMT A & B scores than the control group. Only the control group showed a significant reduction in anxiety but the groups were not significantly different in anxiety at the end of the study. The BOXVR group reported significantly greater enjoyment after each exercise session than the guided video group.
Conclusion:
BOXVR was shown to be effective in reducing adolescent stress and improving executive function over a three-week period. While larger studies with real-life functional outcomes are necessary, boxing with an immersive VR game represents a potential non-pharmaceutical mode to reduce stress in adolescents that is easy to implement in school settings.
Introduction
Over the past two decades, rates of adolescent anxiety have steadily risen, reaching 32% in 2020. 1 Adolescent stress levels exceed those of adults, and are significantly higher than the healthy benchmark set by the American Psychological Association both during the academic year and the summer. 2 The Coronavirus Disease 2019 (COVID-19) pandemic3,4 has exacerbated anxiety and stress in adolescents, thus inflating the existing adverse effects that accompany anxiety and stress symptomatology, including reduced cognitive performance.5,6 Heightened anxiety and stress have been shown to negatively impact overall quality of life and academic performance.7,8 The perception of events as stressful is higher in adolescents compared with children and adults and the incidence of stressful events overall is high. This is particularly significant because the adolescent brain has been referred to as “brain in transition” and the cortex undergoes tremendous “remodeling” during this time of life. 9 For instance, when adolescent rats were experimentally induced with stress, noticeable changes occurred with their working memory as grown rats. 10
Given that, there is a crucial need for cost-effective, engaging, and time-sensitive interventions that can reduce anxiety and stress in adolescents and improve cognitive performance while offering the flexibility to be administered in a school and/or home setting.
Exercise represents a nonpharmaceutical method to reduce anxiety and stress and improve cognitive performance in adolescents. Exercising stimulates the production of endorphins, neurosignaling molecules that regulate mood and reduce stress. 11 Exercise can provide a number of other benefits to both physical and mental health, as it has been shown to improve cognitive performance and promote verbal memory potentially by increasing blood flow and brain oxygenation.12,13 Specifically, exercises involving large muscle groups moving at rhythmic flow patterns, have been shown to alleviate depression. 14 A popular example of this type of exercise is boxing. Many benefits have been attributed to boxing as a form of therapy, including help with stress and anger management; improved confidence, self-esteem, and mood; reduced anxiety; and improved focus and sleep quality. 15 Boxing is high-intensity training that may have a better therapeutic effect on obesity, cardiovascular, and health-related quality-of-life outcomes than an equivalent dose of brisk walking. 16
Zheng et al suggested that shadow boxing (i.e., the practice of committing repetitive boxing movements to muscle memory), paired with psychosomatic relaxation, had an added beneficial effect on depression and anxiety among people with type 2 diabetes. 17
Virtual reality (VR) is a novel approach to reducing adolescent anxiety and stress as it has the potential to make exercise more engaging, thus encouraging regular exercise, adherence to an exercise routine and, in turn, overall improvement to both physical and mental health.18,19 Research suggests that across all age demographics, individuals are more likely to adhere to an exercise routine and maintain healthy exercise habits when exercise is paired with VR, which allows users to experience a three-dimensional environment in a controlled setting while sensory information is provided through head-mounted display (HMD).20,21 Research has indicated that exergames, videogames that double as a form of exercise, can improve adolescents' physical health, in addition to providing social and academic advantages. 22 Oculus Rift off-the-shelf game software, may provide an accessible, and engaging solution. Exercise with an Oculus Rift off-the-shelf game was shown to be effective in promoting physical rehabilitation in adults with balance disorders. 23 A recent systematic review noted that boxing exergames are an effective exercise tool to increase energy expenditure and physical activity of adequate intensity in young adults 24
However, there remains a lack of research investigating efficacious and engaging modes of exercise to specifically moderate adolescent anxiety and stress, as much of existing research has focused exclusively on the adult population.25,26 Specifically, the efficacy of Oculus Rift off-the-shelf boxing games has not been investigated in adolescents.
Exercise is categorized in two distinct ways: acute exercise, a single bout of exercise, and chronic exercise, repeated and consistent sessions of exercise over a short or long period of time, ranging from weeks to months.27,28 Research has addressed the efficacy of both acute and chronic exercise in anxiety and stress mediation. Acute exercise has been shown to be effective in reducing anxiety and stress symptomatology immediately after an exercise session and chronic exercise has been demonstrated to be effective in reducing anxiety and stress as exercise sessions are regularly completed.29,30 Young adults reported a reduction in anxiety sensitivity during a six-session exercise intervention program and at a 1-week follow-up after exercise sessions halted. 31 A 20-week exergame program where adolescents played Nintendo Wii Active games for 30–60 minutes daily at school was found to be effective for weight loss and psychosocial health. 32 The evidence regarding the effect of acute or chronic exercise on executive function and academic performance in adolescents is inconclusive with some studies suggesting improvement in memory following exercise. 33
Many adolescents lack the time, resources, or desire to participate in consistent exercise, 34 thus necessitating the development of exercise methods that are more efficacious and engaging and have positive effects in shorter periods of interventions.
This study investigated the impact of chronic exercise with and without VR on anxiety, stress, and executive function in a cohort of adolescents. We also quantified enjoyment immediately after exercise to elucidate if adolescents found exercise with VR more engaging than exercise with a guided video. Adolescents who participated in chronic exercise, with or without VR, were expected to report reduced anxiety and stress and improved executive function at weekly checkpoints and at the culmination of the study. Furthermore, adolescents who participated in exercise with VR were expected to report higher levels of enjoyment than those who engaged in traditional exercise.
Methods
Recruitment and experimental design
Participants were recruited from a public high school in suburban New York through science classes and through email. This study was approved by the Ossining High School Institutional Review Board. There was no clinical trial registration for the study. Participants were healthy high school students between the ages 14 and 18 able to participate in physical activity of at least moderate intensity. All participants completed an informed consent form and a photo release, signed by both the participant and a parent/guardian. Participants were also instructed to complete a short demographics form that collected information on age, gender, and average weekly hours of exercise. Participants (n = 42) were randomized to one of three cohorts: a BOXVR group (n = 14), a guided video group (n = 14), or a nonintervention control group (n = 14). Allocation was done using block randomization. Once 42 students enrolled, a person external to the testing and intervention created a sheet with 14 slots per group and used an excel random generated number to create the group allocation. For 3 weeks, participants in the BOXVR and guided video groups engaged in exercise with VR or exercise with a guided workout video, respectively, 5 times a week, for a total of 15 exercise sessions, each 10 minutes in length.
The nonintervention control group did not participate in any exercise in relation to this study. The study took place in summer 2021. Baseline data were collected, and the first exercise sessions occurred on July 19, 2021. The last session of exercise occurred on August 6, 2021. Follow-up data were collected on August 13, 2021. See Supplementary tables (The Consolidated Standards of Reporting Trials (CONSORT) and the Physiotherapy Evidence Database (PEDro) scale) for a detailed study design.
Outcome measures and testing procedures
In all three cohorts the Trail Making Test (TMT)35,36 was administered twice. The Pediatric Anxiety Short Form 8a (PASF) 37 and Psychological Stress Experience-Short Form 8a (PSES), 38 both certified by the Patient-Reported Outcomes Measurement Information System (PROMIS), were used to measure anxiety and stress, respectively. All participants completed virtual forms of the PASF and PSES a total of five times over the course of this study; at a baseline assessment, at three weekly checkpoints, and at a 1-week follow-up after exercise sessions halted (Fig. 1). Participants in the BOXVR group and the guided video group completed the Physical Activity Enjoyment Scale (PACES) after each exercise session, which asks participants to rate their enjoyment and engagement. 39 Before and immediately after each exercise session, participant heart rate was recorded with a Zacurate Pro Series 500DL Fingertip Pulse Oximeter in beats per minute.
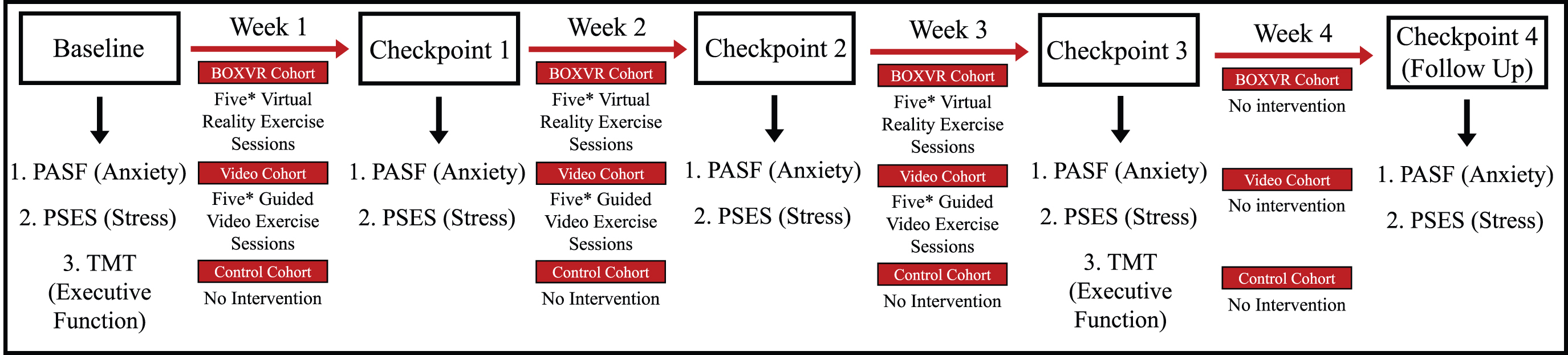
Study timeline indicating when outcome measures were administered. *Indicates that heart rate was measured before and after exercise on a Zacurate Pro Series 500DL Fingertip Pulse Oximeter and enjoyment was quantified at the end of each exercise session using the PACES. PACES, Physical Activity Enjoyment Scale; PASF, Pediatric Anxiety Short Form 8a; PSES, Psychological Stress Experience-Short Form 8a; TMT, Trail Making Test. Color images are available online.
Participants rested for a couple of minutes after entering the room before heart rate was measured. During heart rate measurement, they stood and reached their hand forward and the examiner placed the oximeter on their index finger until the reading stabilized (about 30 seconds). Pulse oximeter has previously been shown to be comparable to radial pulse palpitation in healthy adults. 40
Pediatric Anxiety Short Form 8a
The PASF (Cronbach α = 0.91) 41 was obtained through the PROMIS database and then converted to a digital form to allow participants to complete the form remotely at weekly checkpoints, which occurred on days of no exercise.37,41 The PASF included eight questions and measured anxiety on a Likert scale from 1 (Never) to 5 (Almost Always). Raw scores were calculated by summing participant responses. The lowest possible score is 8 and the highest is 40. Raw scores were then converted to T scores that can be compared with each other and those of the general population using the PROMIS conversion chart. Conversion to a T-score rescales the raw score into a standardized score with a mean of 50 and a standard deviation of 10. T-score <55 is considered normal, 55–64.5 is slightly elevated, 65.7–79.3 is elevated, and above 79.3 is very elevated.
Psychological Stress Experiences Form 8a
The PSES (Cronbach α = 0.90) 42 was obtained through the PROMIS database and then converted to a digital form to allow participants to complete the form remotely at weekly checkpoints, which occurred on days of no exercise.38,42 The structure of the questionnaire and scoring is identical to that of the PASF. Results are interpreted as the number of standard deviations from the average.
TMT parts A and B
The TMT A and B43–44 (Cronbach's α = 0.84), 43 designed to measure executive function, were administered twice. 36 Both parts of the TMT were administered in pen and paper format. Participants were taken to a quiet office in the school building to avoid distraction. They were instructed to connect circles placed in a semirandom fixed order, in either ascending numeric (Part A) or numeric-alphabetical (Part B) order by drawing a line without lifting the pen. Participants were timed as they completed the TMT using a hand-held stopwatch, always by the same examiner. Time to complete the test was reported in milliseconds. A lower score indicates higher executive function. All participants completed the TMT in a quiet classroom with limited auditory and visual distractions. Both parts of the TMT have been demonstrated to have excellent interrater reliability and internal consistency and are ideal for administration to the adolescent population as they are free, simple to understand, and quick to complete. For young adults (18–24 years of age) normal performance on the TMT A is considered 22 seconds (min–max 12–57) and on the TMT B 48 seconds (29–95). 44
Physical Activity Enjoyment Scale
The PACES (Cronbach α = 0.95) 45 measured participant enjoyment through an 18-item questionnaire, which asked participants to rate how they felt about the physical activity they just completed on a Likert scale from 1 to 7.39,45 Participants in both the BOXVR group and guided video group completed the PACES digitally through Google Forms immediately after each exercise session. Scores were calculated by summing participant responses. The lowest possible score (indicating the lowest level of enjoyment) was 18 and the highest was 126. The PACES is widely used to measure physical activity enjoyment in adolescents and has been shown to have high internal consistency and strong test–retest reliability. 45
BOXVR group
Participants in the BOXVR group (n = 14) wore an Oculus Rift (Facebook, CA) HMD, equipped with an earpiece for auditory immersion (Fig. 2A

Guided video group
Participants assigned to the guided video group (n = 14) participated in aerobic exercises with a guided video that mimicked the movements performed while participating in BOXVR, including squats, ducks, hooks, and jabs. A 10-minute guided video titled “10 Minute Beginner Boxing Workout,” produced and led by personal trainer Michelle Sims, guided participants in the traditional exercise group through a beginner boxing workout. Participants were allowed to discontinue at any point during each session. However, no participants reported any discomfort, and all participants completed each session they attended in full.
All BOXVR and guided video sessions took place in a clear area of a quiet classroom with limited distractions. This location was the same for both cohorts and for all exercise sessions. Within the school hours (8 am to 4 pm), participants were given the opportunity to select which times of the day they came in to complete their exercise sessions to best work around their schedules and encourage participation. Most participants opted to come the same time every day (ex. they would sign up for 8 am–8:15 am for all 15 sessions.)
Nonintervention control group
Participants in the nonintervention control group (n = 14) did not participate in any exercise in relation to this study but completed cognitive tests and anxiety/stress measures over the same intervals as the other cohorts.
Data analysis
All data were stored in Microsoft Excel Version 16.51 and analyzed in GraphPad Prism 9.0 and IBM SPSS Statistics Version 27.0. A minimum of eight attended sessions (≥50% adherence standard) was required for participant data to be analyzed. Before beginning data analysis, data were inspected for outliers and normality. Descriptive statistics were calculated for all outcome measures. We applied a nonparametric approach for analysis of PASF, PSES, and TMT data. Kruskal–Wallis tests were used to compare all groups at baseline and at the last data point (immediately after for TMT A and B and follow-up for anxiety and stress). If a significant result was obtained a Mann–Whitney test was performed to compare between each two groups and Bonferroni correction was applied. Friedman's tests were run to test for changes over time in anxiety and stress for each group (BOXVR, guided video, control) across the five data points. Wilcoxon matched pair signed-rank tests were run to compare TMT scores from before (pre) and after (post) the completion of 15 exercise sessions in all cohorts. Enjoyment scores (PACES) were averaged across all sessions and compared between the BOXVR and guided video groups using Mann–Whitney test.
We calculated the mean difference in heart rate from preexercise to postexercise per group and compared between the BOXVR and guided video groups using Mann–Whitney test. Only PACES scores and heart rate measures from exercise sessions 1 through 7 were included in statistical analysis due to missing data values from days 8 through 15. Enjoyment was submitted digitally and sometimes there were connectivity issues, such that participants thought they submitted it, but it did not go through. For heart rate monitoring, there were a few sessions where the batteries needed to be replaced and we did not want to change participants' exercise schedule. Statistical significance for all analyses was held at P < 0.05.
Results
Sample demographics
The mean age of participants in the BOXVR, guided video, and control cohorts was 15.5 (1.1), 15.5 (1.2), and 16.2 (1.1), respectively. The number of females in the BOXVR, guided video, and control cohorts was 9 (64%), 13 (93%), and 7 (50%), respectively. The median exercise hours per week of the BOXVR, guided video, and control cohorts was 3 (12), 2 (15), and 3.5 (14), respectively. Of the 42 participants, 30 (71%) reported that they regularly exercise at varying intensities. Nine participants (21%) reported no prior experience with VR. All participants attended >50% of the sessions and were included in the analysis. The average number of sessions attended was 10.78 (BOXVR, SD = 2.14) and 10.71 (guided video, SD = 1.94). The range was 8 to 15 (100% attendance) in both groups.
Anxiety
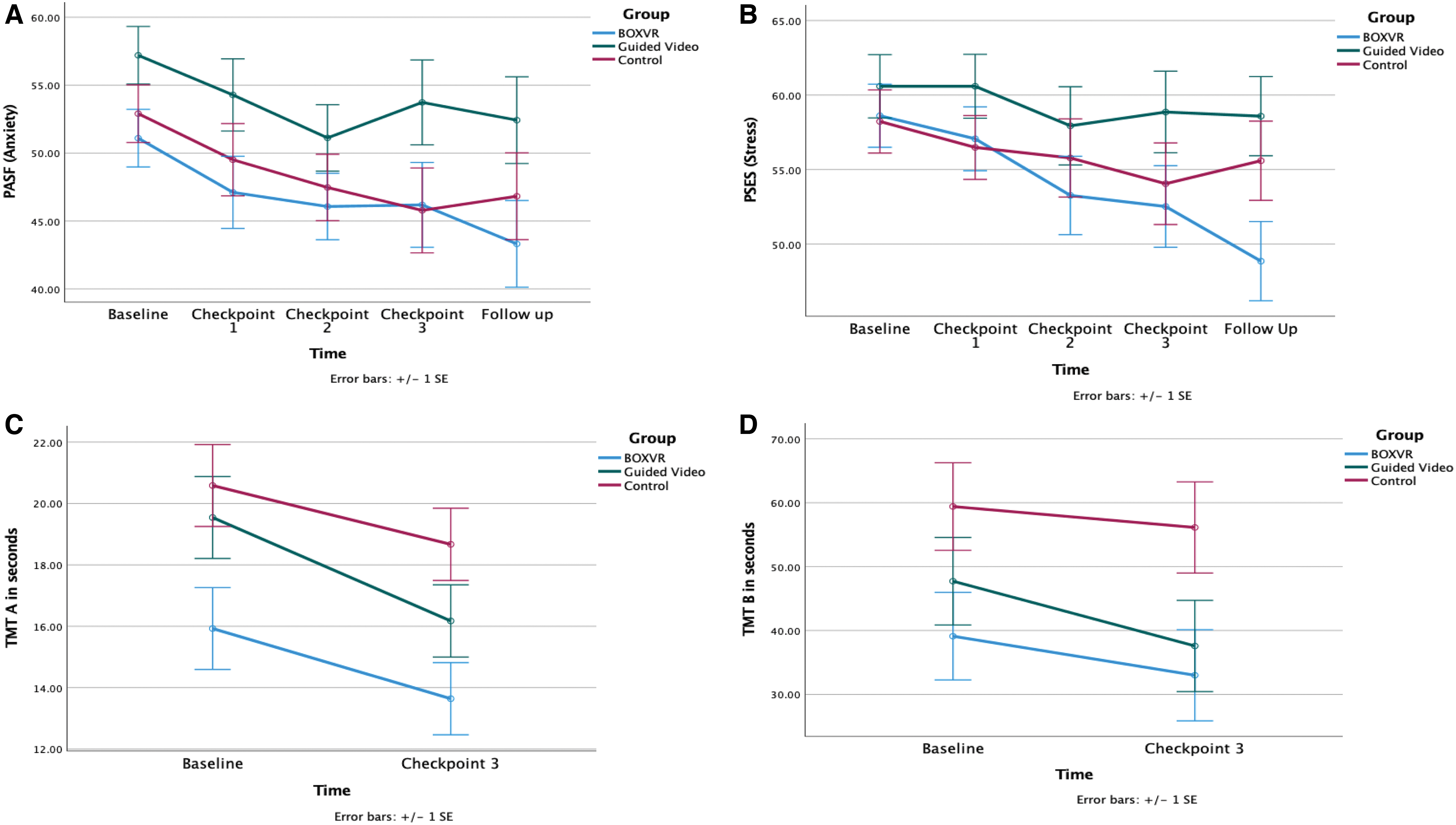
The groups were comparable at baseline (P = 0.16) in PASF scores. While the control group showed a statistically significant reduction (χ 2 = 12.526, P = 0.014) the groups were not significantly different at the end of the study (P = 0.23).
Stress
The groups were comparable at baseline (P = 0.61) in PSES scores. Only the BOXVR group showed a statistically significant reduction in PSES scores from baseline to follow-up (χ 2 = 24.719, P < 0.001; Fig. 3 and Table 1). The groups were significantly different on PSES at the follow-up point (P = 0.049). Pairwise comparisons with Bonferroni correction showed that the BOXVR group had a significantly lower PSES score (less stress) compared with the guided video group (P = 0.048).
Outcome Measures of the Present Study for the BoxVR (1), Guided Video (2) and Control (3) Cohorts
The PASF was used to measure anxiety, the PSES was used to measure stress, and the Trail Making Test Parts A and B were used to measure executive function. Values on this table for the PASF and PSES represent T scores respective to the test (lower score indicating less anxiety/stress) and values for TMT A and TMT B are in seconds (lower score indicating higher levels of executive function). N/A represents that no data were collected from participants at the given timepoint.
PASF, Pediatric Anxiety Short Form 8a; PSES, Psychological Stress Experiences Short Form; Range, difference between minimum and maximum so this is fine; SD, standard deviation; TMT, Trail Making Test.
TMT A
The groups were comparable at baseline (P = 0.07) in TMT A performance. All three cohorts showed statistically significant (P < 0.05) reductions in time needed to complete TMT A at the end of the study (Fig. 3 and Table 1). The groups were significantly different on TMT A at the follow-up point (P = 0.027). Pairwise comparisons with Bonferroni correction showed that the BOXVR group had a significantly faster TMT A performance compared with the control group (P = 0.023).
TMT B
The groups were comparable at baseline (P = 0.18) in TMT B performance. Only the BOXVR group showed a statistically significant (P = 0.02) decrease in time needed to complete TMT B (Fig. 3 and Table 1). The groups were significantly different on TMT B at the end of the study (P = 0.027). Pairwise comparisons with Bonferroni correction showed that the BOXVR group had a significantly faster TMT B performance compared with the control group (P = 0.035).
Enjoyment
Adolescents who participated in exercise with BOXVR reported higher PACES scores (enjoyment) after each exercise session (median = 108.43, 25th percentile = 99.21, 75th percentile = 117.79) than adolescents who participated in exercise with a guided video (median = 90, 25th percentile = 71.57, 75th percentile = 104.36) (Z = −2.76, P = 0.005) (Fig. 4).
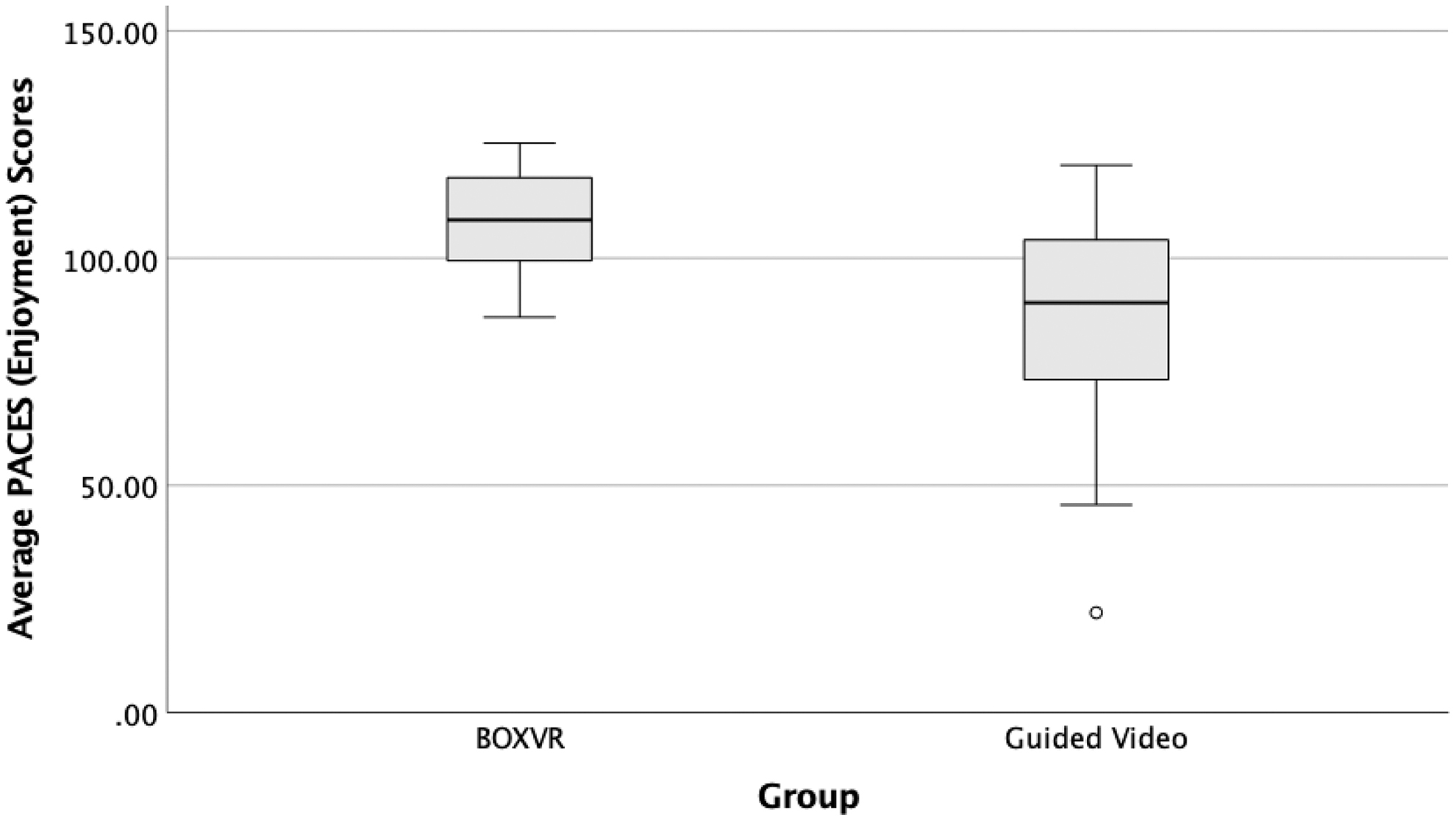
PACES scores (enjoyment) for the BOXVR and guided video groups. Enjoyment was measured immediately after exercise and the average across all sessions was compared. The lowest possible score (indicating the lowest level of enjoyment) is 18 and the highest is 126.
Heart rate
The BOXVR increased their heart rate on average by 16.99 beats per minute (BPM) (SD = 9.95, median = 14.3, min = 4.00, max = 35.21). The guided video group increased their heart rate on average by 31.2 BPM (SD = 7.05, median = 31.63, min = 17.07, max = 44.27). Adolescents in the guided video group showed a significantly larger increase in heart rate from preexercise to postexercise than adolescents in the BOXVR group (Z = −3.22, P = 0.001) (Fig. 5).

Mean difference in heart rate from preexercise to postexercise for the BOXVR and guided video groups. Heart rate was measured with a Zacurate Pro Series 500DL Fingertip Pulse Oximeter immediately before and after each exercise session.
Discussion
This small pilot study investigated the effects of a boxing VR game versus boxing with a guided video and a nonexercise control on anxiety, stress, and executive function in adolescents over a three-week period. The groups were comparable at baseline on all outcomes. The three groups started at the high end of normal for youth anxiety, one standard deviation above the average for youth stress, and at better TMT performance than norms established for young adults. 44 At the end of the study, the BOXVR group reported significantly lower stress levels than the guided video group, and significantly better TMT A and B scores than the control group. All three groups had significantly better TMT A performance at the end of the study. Only the BOXVR group showed a significant improvement in stress levels and TMT B performance. The BOXVR group reported significantly higher levels of enjoyment than the guided video group. The control group demonstrated a significant reduction in anxiety although the groups were not significantly different on anxiety levels at follow-up.
This is a small study and, while the results need to be replicated in larger samples, it appears that the BOXVR group improved more than the control and guided video groups. Lack of significant improvements in the guided video group were surprising given previous studies supporting exercise programs for mental health12,13 and cognitive function. 46 Given that both groups performed boxing movements, and the increase in heart rate with exercise was significantly higher in the guided video group versus the BOXVR group, it is possible that engagement and enjoyment in a “play” setting may contribute to mental aspects of health in the short-term more than level of effort. 47 Indeed, the BOXVR group reported significantly greater enjoyment with some participants in the guided video group reporting they did not enjoy the program at all. An acute bout of exercise with immersive VR that places users in a virtual dodgeball scene and traditional dodgeball were equally effective in reducing stress, anxiety, and improving TMT scores in adolescents but both groups were involved in a game-like activity. 30
The BOXVR games include virtual targets, provide visual and auditory feedback, and provide scores, whereas the guided video does not. Future studies should investigate what aspects of gaming in VR contribute the most to stress reduction and cognitive performance.
The control group was the only group that showed a significant reduction in anxiety. This could be interpreted as possible changes in behavior simply due to being enrolled in a research study and asked about anxiety status. The three groups were not significantly different at follow-up (as they were not at baseline). Overall reported anxiety levels on average were around the norm average for this age group. However, at baseline 28 out of 42 participants reported anxiety above 50 standard score, and 9 of them had a score above 60. These results in a healthy active young sample call for further attention to interventions that address adolescents' mental health in the school environment. Physical activity interventions such as yoga programs for young people have been shown to have a small beneficial effect for reduced anxiety, but overall, the research on anxiety reduction in adolescents is limited and variable. 46 It is possible that changes in anxiety require longer interventions or relaxation-based interventions. This needs to be examined in future research in this specific population.
This study was delivered in a high school setting. The fact that the study was conducted over the summer assisted in providing space, particularly quiet space to conduct the assessments. Overall implementation in the school was found to be feasible and simple. Both interventions required minimal space. The BOXVR game requires a participant to squat, lean, and box but they do not walk or move around. The equipment is affordable, and a high school student with no background in technology was able to setup the game. Once the game is downloaded, there is no need for any network connection to play. The headset has embedded headphones and so the gaming experience is quiet and would not interfere with school activities. This game was run by a gaming computer although new headsets have minimal requirements for a computer or offer an “all in one” experience with no computer at all for their off-the-shelf games.
Several limitations of this study must be acknowledged. This was a first-step pilot study with a short duration (3 weeks) and a small sample size (n = 14 per group). The small sample did not allow for testing of interaction effects and the data were analyzed in a nonparametric approach and future studies with longer follow-up, adequately powered to test for interactions effects, are needed to confirm our preliminary findings. As the results of this study suggest significant positive effects of VR-based chronic exercise, it is crucial that future research examines the cost-efficacy and feasibility of implementing such intervention programs in a high school setting to reduce stress and improve cognitive performance in adolescents in adequately powered studies to fully investigate interaction effects. This study also relied primarily on self-reported data, which are easily influenced by a participant's anxiety and stress levels at the time of completing the questionnaire. We aimed to negate this effect by using measures that specifically ask participants to reflect on the last 7 days as opposed to their current anxiety and stress levels. While statistically significant differences have been observed, minimal clinically important differences have not been established for these measures in adolescents. 48
The fact that all three groups improved significantly on the TMT A and only the BOXVR group improved significantly on the TMT B suggests that the TMT A is still suspectable to learning effects, even after 3 weeks. 49 We did not take into account possible changes in mood due to the menstrual cycle. Nevertheless, given that the study had a random assignment to groups, it is likely that any influence of the menstrual cycle will not be different between groups. Future research should aim to quantify anxiety and stress with clinical, non-self-reported measures.
Conclusion
This study adds to a growing body of literature that indicates the importance of regular exercise for both physical and mental health and builds upon previous research by examining the impact of chronic exercise exclusively in the adolescent population while employing the novel and widely available Oculus Rift off-the-shelf game BOXVR. Our results indicate that boxing with a VR game, when done consistently over a 3-week period, appears to be effective in reducing stress and improving executive function but future larger studies are needed to confirm these findings. Adolescents who participated in BOXVR reported significantly higher levels of enjoyment than those who participated in traditional boxing with a guided video. The results from this pilot study should be interpreted with caution given the limitations discussed above. Future studies should further investigate how VR fitness games, specifically boxing games, may augment the mental and psychological benefits of exercise, thus potentially providing an alternate method of stress reduction in adolescents that is efficacious, engaging, and simple to implement in the school setting.
Footnotes
Acknowledgments
The authors thank Ossining High School as well as the science research teachers, Angelo Piccirillo and Valerie Holmes, for all their guidance on the project.
Authors' Contributions
R.C.: Conceptualization (equal), Methodology (lead), writing—original draft (lead), and review and editing (equal); A.V.L.: Conceptualization (equal), and formal analysis (lead); Methodology (supporting), and writing—review and editing (equal).
Data Availability Statement
Author Disclosure Statement
No competing financial interests exist.
Funding Information
A.V.L. is funded by an R21 DC018101 Early Career Researcher grant from the National Institute on Deafness and Other Communication Disorders (NIDCD). The sponsors had no role in the study design, collection, analysis, and interpretation of data; in the writing of the article; or in the decision to submit the article for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.