
Abstract
Purpose:
The purpose of this study was to determine the effects of nonimmersive virtual reality (VR) and task-oriented circuit training on gait, balance, cognitive domains, and quality of life among the elderly population.
Methods:
This is a single-blind randomized control trial in which 28 elderly individuals between 60 and 75 years were selected. The participants were divided into two groups, task-oriented circuit training and the other receiving nonimmersive VR treatment, with 14 participants in each group. To analyze the effects of both training on balance and gait time up and go test (TUGT), dynamic gait index (DGI), measures were used and for cognitive domains Montreal cognitive assessment (MoCA) scale was used. Short form 12 (SF-12) (along with two domains, Physical Component Summary and Mental Component Summary) was used for the measurement of quality of life. The treatment duration was 8 weeks for both groups. Both the pre-test and post-test readings were analyzed and compared.
Results:
The mean age of participants was 66.91 ± 3.79 years. Within-group comparison between the pre-test and post-test indicated that significant differences (P < 0.05) existed in all the outcome measures (TUGT, DGI, MoCA, and SF-12) in both groups. However, between-group comparison, significant differences were only found in TUGT and DGI in nonimmersive VR group.
Conclusion:
This study concluded that both interventions nonimmersive VR and task-oriented circuit training were beneficial for improving balance, gait, quality of life, and cognitive domains like memory, attention spans, executive functions, and so on in elderly population. However nonimmersive virtual reality training is a more effective, feasible, and safe alternative and can be proposed as a form of fall prevention exercise for the older adults.
ClinicalTrials.gov Identifier:
NCT05021432.
Introduction
The rapidity in number of elderly population has led to challenging effects for the rehabilitation professionals as well as the overall health system, especially for daily activities of living in functional capacity and independence. 1 With growing age, several physical and functional alterations occur especially related to mobility, disturbed body balance (static and dynamic), physical and cognitive declines, impaired gait, thereby leading to falls and fall-related mortality among the elderly population. 2 Falls are the second leading cause of accidental or unintentional injury deaths worldwide. Approximately 40% of older adults >65 years fall at least once a year and 10%–20% of these falls result in hospitalizations, which leads to increase in disability-adjusted life-years. Women are more prone to age-specific fall rates than men. 3
Regular exercise-based activities performed by the elderly can improve walking speed, balance impairments, muscle strength, and mobility capabilities by increasing their functional abilities, thereby eliminating the risk of falling and providing stabilization. 4 Previously it has been reported that different approaches useful in improving balance, gait, and cognition as compared with the general conventional therapies to manage balance impairment and postural instability in community-dwelling older adults has been recommended. 5 These include specially designed exercise programs for targeted muscle strength and endurance, stretching, sensory feedback training, vestibular rehabilitation with reaction time training, cognitive exercises, frequent proprioceptor's stimulation around muscles and joints, tai-chi, environmental modification with proper ergonomics, and circuit training.6,7
In recent years, intervention methods based on virtual reality (VR) have been introduced. VR refers to interactive, three-dimensional simulated world wherein a person can move about and interact, as if one is actually present in the imaginary space that may provide the feedback mechanism about the body orientation. 8
This method can increase motivational effects while the users perform tasks with interest and engaging environment making it fun for the individuals. 9 As described previously, VR has been studied to overcome limitations in existing interventions, and preventive medicine exercises can be applied with it to prevent falling in the elderly population. 10 However, existing studies are limited because they only studied the balance ability of the elderly after the application of nonimmersive VR exercise programs, and most of them only focused on comparing the application of VR programs and exercises that combined a VR exercise program and visual and auditory sensory feedback exercises. 11
Task-oriented circuit class training is defined as intervention provided to more than two participants or in group simultaneously, which involves a series of workstations focusing on gait practice and functional gait-related tasks. In this program, multiple task-related training patterns involving neuromuscular and musculoskeletal systems are targeted to achieve functional goals. 12
Some researchers have shown that circuit-based training, where lighter loads are lifted with minimal rest, is very effective for increasing functional capacity, and strength while improving body composition. Thus, circuit training is a time-efficient training modality that can elicit demonstrable improvements in health and physical fitness. 13
There are few studies on the effect of nonimmersive VR exercise programs accompanied by task-oriented circuit training in the elderly population; so the purpose of this study was to determine the comparative effects of VR and task-oriented circuit training on gait, balance, cognition, and quality of life among the elderly population. This study aims to investigate the cost-effectiveness and its effects in the elderly population taking comorbidity into account, and to investigate how to help people maintain and improve their physical and cognitive abilities, like gait, balance, memory, attention span, and task planning and execution after their rehabilitation program ends by gradually adding complexity and intensity progression in the tasks.
Methods
Study design
This study was a randomized clinical trial, comparing effects of nonimmersive VR and task-oriented circuit training in elderly population. Sample size was calculated through Open Epi tool. It was set at a significance level of α = 0.05. Assumed error was calculated according to the standard deviation established for time up and go test (TUGT) in previous studies and a significance level of α = 0.05. A total of 28 participants completed the intervention. Participants who meet the inclusion criteria were electronically (https://www.randomizer.org) randomized by blocked design into two arms: a nonimmersive VR training group (VRTG) (n = 14), and a task-oriented circuit training group (TOCTG) (n = 14). This procedure was established according to “CONSORT” statement (www.consort-statement.org), as given in the flowchart in Figure 1.
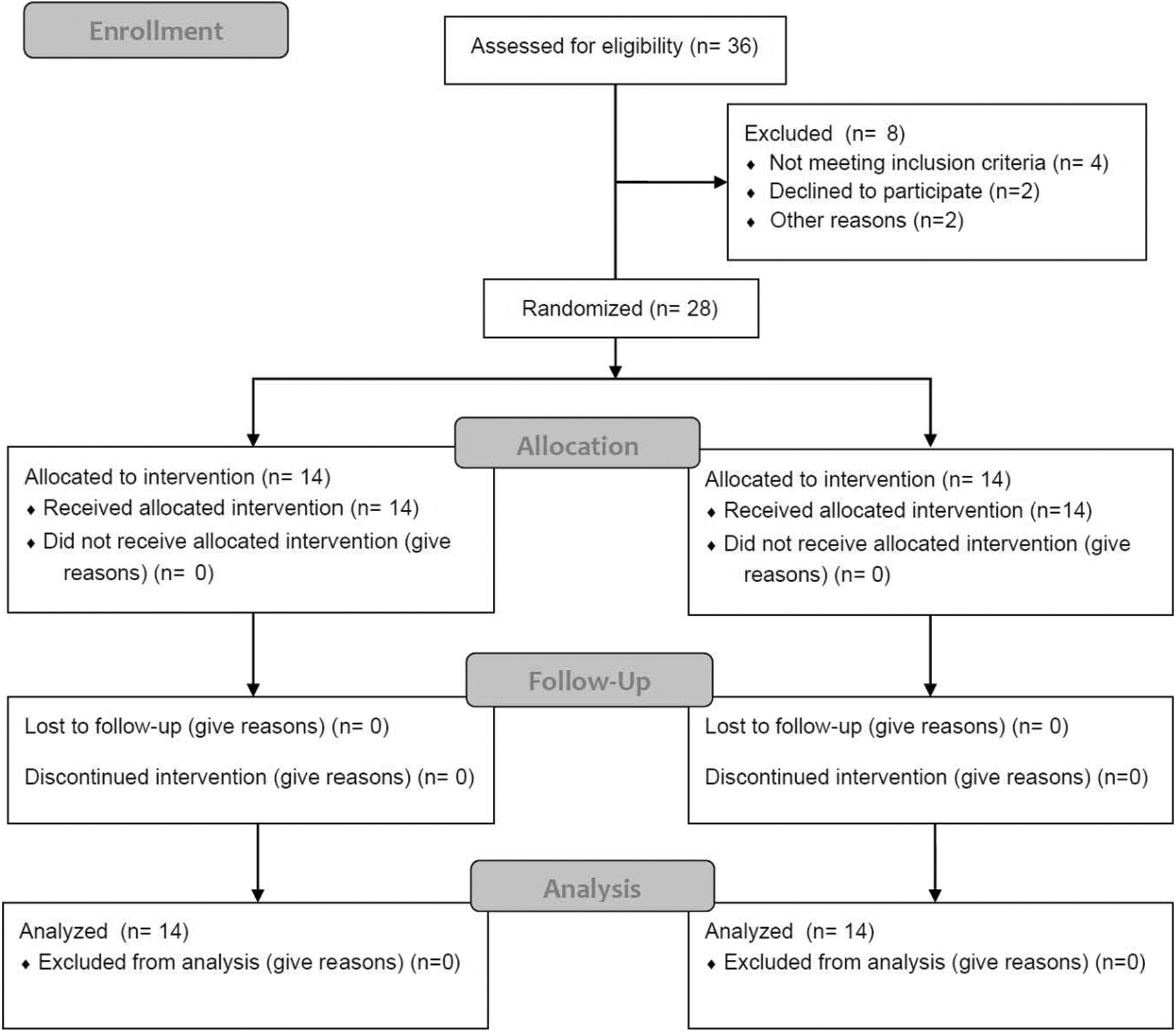
CONSORT flow diagram.
The study was conducted for a duration of 6 months at physiotherapy departments of Pakistan Railway General Hospital (PRH) and Al-Mustafa trust Medical center. Written consent from all participants was obtained. All participants were assessed for eligibility criteria and then divided into two groups.
Participants
Ethical consideration was obtained from Ethical Committee of Riphah International University. Permission letter was also obtained from PRH and Al-Mustafa Trust Medical center for conducting this research. During the development and implementation of the research plan there was no violation of the ethical and moral values. All the subjects were explained about the study purpose before the start of data collection and their identity was protected as data were coded. Participants aged between 60 and 75 years of both genders with Standardized Mini-Mental State Examination (SMMSE) score >19, having a history of fall once or twice in the past year and being identified as being at medium risk for a fall on the initial medical assessment, score better than 36 on the Berg Balance Scale, able to walk with or without assistive devices after physiotherapist evaluation, and oral consent taken were recruited in the study.
Participants presenting with a progressive neurologic disease or vestibular disease or diseases like myasthenia gravis, stroke (any type), multiple sclerosis or any severe inflammatory conditions, acute exacerbations, fractures, and open wounds, or patients declared unfit for physical activities following medical assessment, were excluded from the study.
Interventions
Patients reporting with balance, gait, fall, or cognition problems according to the preset criteria were randomized into two groups, that is, VRTG and TOCTG. Outcomes of both groups were evaluated at baseline and 8 weeks. Physiotherapists were present with the patient during the session to ensure safety and protection during protocols.
For the nonimmersive VR-based training, the following components were utilized: The Wii Console Nintendo (RVL001, Nintendo, EUR, 2008), Wii Balance Board (Nintendo D-63760 GroBostheim WBB) provided by Nintendo, the Wii Fit Plus software, and the Wii remote control (RVL-003, Nintendo Wii, EUR, 2008). The program consisted of table tilt, heading, tightrope walking, penguin slide, balance slalom, and jogging activity. Before initiating the program, patients were instructed to stand on the balance board, which was connected to the Wii console Bluetooth. Patient movement was displayed on the light emitting diode screen by a representative Avatar (this allows a nonegoistic self-expression). 15 For the Wii Fit Plus software, the users' basic registration information was entered into the system before starting the program.
Movement of physical center of gravity and body mass index were measured by the WBB, and the individual exercise time and results were recorded. The VR-based games were selected depending on the subjects' interests and motivation, and the levels of difficulty were decided based on information provided in previous studies to achieve suitable levels for balance, gait, cognition, and quality of life, thereby reducing the risk of falls. 16
The subjects participated in the nonimmersive VR training program for a total of 30 minutes. They performed all seven programs once and then freely participated in the games of their choice for the remainder of the session. In this study, the subjects stood in front of the monitor at 2 m. An axillary table was placed next to the participant, and an assistant stood on the other side for the subject's safety. If abnormal myotonic was noted in any of the limbs or any compensatory movements, the assistant lowered the patient with assistance before the initiation of training. When the participant successfully completed the program that was based on the individual's abilities, the level of difficulty was adjusted to an advanced level. The training programs in both the experimental and control groups aimed to improve weight shift control. All the subjects who participated in the experimental group received a nonimmersive VR-based training program for 30 min/day, 3 days/week for 4 weeks, and in next 4 weeks for 40 minutes. Each session included a 10-minute warm-up stretch.
Simultaneously, the other group underwent task-oriented circuit training. In this program, multiple task-related training patterns involving neuromuscular and musculoskeletal systems were targeted. This involved training the individual by utilizing 10 different exercises in a single program. The participants had a total of 24 sessions, 30 minutes, and 3 days in a week for 4 weeks (gradually increasing time periods from 30 to 40 minutes in the next 4 weeks). The circuit consisted of; sit-to-stand, self-sways, standing balance, step ups, standing hamstring curls, tandem walking, Swiss ball squats, backward walks, side leg lifts, and marching in place. The intervention protocol is given in Table 1 for both groups.
Intervention Given to Virtual Reality Training Group and Task-Oriented Circuit Training Group
COG, center of gravity; LED, light emitting diode; TOCTG, task-oriented circuit training group; VRTG, nonimmersive virtual reality training group.
Outcome measures
There was no allocation concealment in the study. Subjects were not aware of the hypotheses being tested. Both groups trained at different times, therefore participants were partially blinded. Testing personnel were blinded to group assignments. TUGT, dynamic gait index (DGI), Montreal cognitive scale, and Short Form survey—short form 12 (SF-12) were used in this study.
TUGT was used to measure the functional mobility and determine the dynamic balance abilities among the elderly people. This test shows excellent test–retest among elderly and stroke patients. Reliability was found to be Intraclass coefficient (ICC) = 0.95. 17
DGI was used to test the dynamic walking balance while the participant is given multiple tasks during walk and different dynamic conditions and assess the risk of falls among the elderly and individuals with neurological conditions compromising the balance. ICCs for test–retest and interrater reliability of total scores were good (r = 0.96). 18
MoCA is a brief tool used to assess cognitive domains and executive functions, and very useful to predict mild cognitive impairment (MCI), a dementia leading to Alzheimer's. Interrater reliability analysis shows high correlation (r = 0.99). 19
The short form Health survey (SF-12) questionnaire was used for measuring the quality of life. It is a valid and reliable instrument. 20
Statistical analysis
Statistical analysis was performed by using the IBM Statistics SPSS v21.0. (IBM Corp., Armonk, NY). The Shapiro–Wilk test of normality was applied to all variables to assess the normality. The data were normally distributed as P > 0.05. Based on the normality, parametric tests were applied to all variables. For the intergroup (between) analysis, independent “t”-test was applied and for intragroup (within) analysis paired “t”-test was applied. Results were expressed as mean ± standard deviation. A value of P < 0.05 was significant.
Results
A total of 28 participants were enrolled for treatment, that is, 14 in VRTG and 14 in the TOCTG. No participant withdrew from the program and completed their 8 weeks of training, which indicates a 100% adherence to the treatment. The mean age of participants in VRTG was 66.91 ± 3.79 years and in TOCTG was it was 66.72 ± 2.91 years. At baseline both groups were homogeneous. There were no statistical differences in all parameters. The descriptive and baseline measures in VR and task-oriented circuit training groups are given in Table 2. After, independent “t” test, the following analytical findings were interpreted in Tables 3 and 4; in case of Montreal cognitive assessment (MoCA) scale, preintervention P-value of both groups was 0.821, whereas after 8 weeks of follow-up for both interventional groups it was 0.182, which shows the nonsignificant differences in both groups.
Descriptive and Baseline Measures in Virtual Reality and Task-Oriented Circuit Training Groups
DM, diabetes mellitus; OA, osteoarthritis.
The Pre- and Postcomparisons of Measured Values in Nonimmersive Virtual Reality and Task-Oriented Circuit Training Groups
Level of significance: **P < 0.01.
DGI, dynamic gait index; MCS, Mental Component Summary; MoCA, Montreal cognitive assessment; PCS, Physical Component Summary; SD, standard deviation; SF-12, short form 12; TUGT, time up and go test.
Intragroup Analysis of Nonimmersive Virtual Reality Group
Level of significance: *P < 0.05, **P < 0.01.
We identified a significant improvement in balance and gait parameters after 8 weeks of training in VRTG for TUGT (P = 0.001) and DGI, whereas SF-12 and its domains D1: Physical Component Summary (PCS) and D2: Mental Component Summary (MCS) have been analyzed by web-based calculator. This calculator interpreted the SF-12 readings in the form of its two domains, physical component score and mental component score. Afterward these scores were added to get a total SF-12, which we then analyzed further in both groups. Its results were nonsignificant at postintervention (P > 0.05) in between-group analysis and significant in within-group analysis Tables 3 and 4 (P < 0.05), which indicates that both interventions are effective in improving the quality of life of older adults.
Discussion
Balance and strength are both essential functions a person must have to prevent themselves from falling, but, in many cases, the falls might also be caused by the underlying cognitive limitations of older persons. 21 Therefore, a combination of physical and cognitive exercise might be an extremely beneficial method of fall prevention. This study examined the effect of a nonimmersive VR game intervention and task-oriented circuit training on balance, gait, and cognitive abilities in older adults. The findings of this study showed that VR game intervention is an effective way to improve balance, working memory, attention span, and frontal brain function. In agreement with previous studies, our data show that balance is significantly impaired independently of the evaluation method used. 22 Impaired control of both static and dynamic balance leads to increased risk of falls during daily activities resulting in severe injuries and decline of quality of life in the elderly people. 15
Posture imbalance during aging is likely a result of a combination of various pathophysiological processes and the cause should be assessed individually. 23 However, in general, a typical mosaic of patterns is observed. The presence of neurological, metabolic, musculoskeletal, cardiovascular, or vision disorders influences the ability to sense upright posture and thus negatively and often progressively influence control of balance. Important parts of proprioception also deteriorate with age and result in a diminished information flow to central nervous system and have been linked to poorer balance control. 24 It should be noted that the above-mentioned factors besides static balance also negatively influences overall motor abilities and thus demanding daily activities such as walking represents a high risk of falls and consequent injury. The present findings complement the findings of a prior meta-analysis demonstrating positive effects of exergaming on balance 25 and postural control (Tahmosybayat et al., 2017) in elderly participants.
These findings support the view that combined physical and cognitive interventions can improve Executive functions in older adults effectively. Literature suggested that the exergame training group showed improvements in lower limb strength and balance and exerts greater cognitive and physical function benefits than task-oriented circuit training. 26 The result of this study shows that aging is associated with a decrease in cognitive, motor, and dual-task capacities, leading to a possible loss in autonomy. Task-oriented circuit training is known to be effective on these functions but suffers from low adherence level. On this point, exergames seem to be a promising solution. 27
Gait speed is significantly associated with transitions in an individual's frailty status. Slow gait speed is the strongest predictor of chronic disability and injurious falls. 28 According to the results of this study, gait speed was improved on TUGT and DGI after nonimmersive VR training. Therefore, improvements in gait speed in both groups were clinically important. Older adults are more likely to adhere to a physical activity program if the program is well designed and enjoyable. 29 Over the past decade, technology-based cognitive interventions have gained immense interest worldwide. 30 The results showed positive effects for the nonimmersive VR intervention on key outcome variables, such as cognitive and physical function. Studies have also shown that VR intervention is effective to improve physical function and walking speed of community-dwelling older adults.
According to a systematic review, all the studies reported improvement in the physical outcomes when nonimmersive VR systems were used for rehabilitation. 25 This may be because the participants engage by the practical relevance of the tasks, the realism of the visual and auditory feedback, and the natural movement-based interface. Study results demonstrate that VR training improves performance in complex dual tasks concurrently targeting balance and mental functions with an active control in older adults.31,32 In older adults, deficits in executive–attention function and visuospatial abilities, also including gait disturbances during dual tasking, are independently associated with the risk of postural instability and falls. 33 In addition, decline in memory and executive functions represents an early marker of cognitive impairment, which is linked to substantial decrease in postural control during dual tasking and dramatically elevated fall risk and not well-represented in current interventions in fall prevention. 34
Among various interventional strategies, exergaming represents a successful approach for targeting postural control, cognitive, and dual-task functions in older adults by providing an interactive and motivating environment for the training of complex multimodal tasks. 35
In terms of the weaknesses of this study, sample size is small. Another potential limitation of the study is the use of self-reports for the falls data episodes, which could be inaccurate. However, excluding subjects with reported cognitive impairment could partially solve this limitation. Nevertheless, although this study was not powered to assess its effect on falls prevention owing to the small sample and the use of self-report, our finding that nonimmersive VR training had a significantly higher effect on falls prevention deserves further exploration in future clinical trials. Another limitation was the lack of follow-up assessment after 8 weeks of intervention limits the inference of the long-term or maintenance effect of the treatment. Furthermore, some important variables such as comorbidities and depression were not assessed in this study, which may affect our results.
Conclusion
This study concluded that nonimmersive VR and task-oriented circuit training can be beneficial for improving balance, gait, quality of life, and cognitive domains like memory, attention and concentration spans, executive functions, and so on in elderly population. However, nonimmersive VR training is more effective and can be proposed as a form of fall prevention exercise for the older adults.
Footnotes
Acknowledgments
The authors thank the staff of the Pakistan General Railway hospital and Al-Mustafa Trust Medical center for their assistance in supervising participants and organizational support for this study.
Authors' Contribution
All authors have made substantial contributions to the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.