
Abstract
The aim of this scoping review was to examine virtual reality (VR) interventions used within rehabilitation and their effect on the functional outcomes of individuals with stroke. Specifically, this study sought to determine the impact of VR on the upper extremity (UE) use of participants as it relates to body function, occupational participation, and overall UE function (UEfxn). Twenty-six articles were selected for inclusion and results were extracted to determine common themes of outcomes among the effects of VR intervention (VRI). Thematic analysis included details about the VRIs used, as well as the change in UE outcomes post-VRI. Overall, positive change in UEfxn was found across many of the studies, indicating that VR technologies may be an effective intervention technique for individuals, poststroke. Findings of this review encourage clinicians to conduct further research regarding VR technology for UE rehabilitation poststroke.
Introduction
Stroke is the third leading cause of death in western countries and has been described as a worldwide pandemic.1,2 In recent studies, it was found that up to 85% of people reported sensorimotor dysfunction in the affected arm for 3–6 months poststroke.1,3,4 Common upper extremity (UE) physical impairments after stroke include paresis, loss of fractionated movement, abnormal muscle tone, and/or changes in somatosensation. 5 These symptoms present great difficulty by limiting an affected person's ability to engage in daily tasks and increasing their dependence on others.
Rehabilitation is a major component of recovery for patients who have experienced a stroke. Multidisciplinary and supportive services begin once a patient is medically stable, ∼48 hours poststroke. 6 Interventions can be performed separately or combined so the treatment plan addresses the functional deficits associated with stroke. 6 Pollock et al. 6 and Delden et al. 7 examined bilateral arm training used in stroke rehabilitation to incorporate identical, synchronous movement.
Bilateral training results included improvement of speed and function of the affected UE during a reaching task. Strengthening interventions after a stroke can increase muscle strength, promote functional improvement, and change the quality of life of the patient. Interventions such as neurodevelopmental treatment, 8 neuromuscular electrical stimulation,6,9,10 and mirror therapy6,11 are also common for UE function (UEfxn) rehabilitation following a stroke. While these interventions are considered to be gold standards for stroke rehabilitation, virtual reality (VR) interventions are promising and should be considered for additional benefits related to improving UEfxn.
VR can be defined as an interactive environment created using an electronic device to immerse an individual in the environment using sounds, feelings, and/or visual options. 12 VR can be categorized by nonimmersive, immersive, motion sensor-based initiation, wearable initiation (WI), game based, occupation based, home based, or facilitybased.5,12 The versatility of technology allows for multiple combinations of VR interventions (VRIs) for stroke rehabilitation targeted toward improving UEfxn.
Available literature discusses features and reasons for use of each VR category, including cost, location, and injury-specific needs. WI technology is most frequently researched and cited in the literature, including the Rehabilitation Gaming System (RGS), the CyberGlove, and the Interactive Rehabilitative and Exercise System, among others.13–20 Nonwearable systems such as the Nintendo Wii, PlayStation EyeToy, and the Computer Assisted Rehabilitation Environment (CAREN) were also used for therapeutic measures.1,21–23 The interactions of VRI targeting the affected UE poststroke can be an innovative therapeutic approach.
Two theoretical bases guiding VR technology in rehabilitation include Social Cognitive Theory (SCT) and Motor Learning Theory. The key concept of SCT is self-efficacy, which can be enhanced by incorporating vicarious learning, encouragement, and rewards based on accomplishment in an effort to strengthen performance. 24 SCT also employs the introduction of more complex tasks as simpler ones are mastered. 24 The combination of improving self-efficacy, while challenging the client creates an ideal atmosphere for continued recovery.
Motor Learning Theory is a complex theory that considers a multitude of factors that contribute to the learning process. With VRI, initial exposure to a novel movement begins the learning process. The client's reproduction of this movement in later sessions and the transfer of skills learned to functional tasks are the true indication of learned behavior. 24 Technologies like VR can create a combination of both internal and external feedback, materializing into what is now known as augmented feedback. This approach is effective in promoting acquisition of new knowledge and skills, as well as transfer to everyday life situations. In this way, VR technologies create a unique experience that provides individuals with necessary feedback to effectively implement learned movement patterns. 24
Previous research is extensive and presents great evidence toward determining the impact of VR on stroke rehabilitation efforts. However, gaps were identified in the literature, indicating lack of knowledge surrounding an established best practice VRI for improvement of UEfxn in individuals with stroke. In an effort to create a greater understanding of this topic, we conducted a scoping review to investigate the impact of VRI on UEfxn for individuals, poststroke.
Methods
Study design and search strategy
This review utilized established procedures25,26 and conformed to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews. 27 Using these guidelines and procedures, primary peer-reviewed journal articles were aggregated from the following databases: MEDLINE, CINAHL, NCBI, Elsevier, and Google Scholar. Key search terms used included the following: stroke; UE deficits, hemiparetic limb, and upper body; gross motor and fine motor; activities of daily living (ADL); VR, virtual game, Xbox Kinect, and Nintendo Wii; and intervention approaches and gold standard interventions. To capture more recently published studies, a supplemental literature search was conducted using the Web of Science database with additional search criteria of publication years 2020–2022.
Eligibility criteria and study selection
Primary research articles were selected for inclusion based on the following criteria: (1) full text, (2) written in English, (3) published between 2007 and 2022, (4) participants must be poststroke with resultant UE functional deficits due to the stroke, (5) use VR as a primary intervention addressing UEfxn, (6) includes information regarding specific VRI protocols, sample size, and participant characteristics, and (7) includes reliable and valid baseline and postintervention outcome measures (OM) evaluating at least one of the following: UEfxn, body function (BF), or occupational participation (OP).
UEfxn included the individual's ability to complete effective functional movement with use of the upper limb as measured by a performance-based UE assessment. BF measures included joint range of motion (ROM) and musculoskeletal strength. OP included an individual's ability to engage in daily functional activities within various settings. Articles were excluded if they involved interventions that did not focus on UE rehabilitation, or if participants were experiencing UE deficits from diagnoses other than stroke. Reviews and meta-analyses were also excluded. Eligibility criteria were used as a screening method for further data extraction.
All authors contributed to the study selection process by screening titles and abstracts for keywords and outcomes. A research table was created in a shared online drive to organize articles. The screening process continued as three reviewers evaluated data within full-text articles for relevance. All reviewers analyzed articles utilizing the stated inclusion and exclusion criteria. In the event of a disagreement, a fourth researcher completed a separate full-text analysis to determine inclusion or exclusion of the article. The shared research table was adapted to reflect the selected articles to prepare for thematic analysis and coding processes.
Data extraction
Three authors primarily contributed to extracting data from selected articles. Data extracted included the following: technology characteristics, intervention protocols, OM, sample size, participant characteristics, and study design. Due to the extensive diversity of assessments utilized across the selected articles, a need emerged for further categorization of each assessment tool OM (i.e., UEfxn, BF, OP). Selected articles were coded for thematic pattern emergence according to the designated OM, study design, significance level, and VRI.
Results
Of the 8096 records initially found, 7952 records were removed due to duplication, inaccessibility to full text, or ineligibility by automation tools. The titles and abstracts of the remaining 144 records were screened based on the remaining inclusion criteria. Eighty-nine articles underwent full-text assessment, with 26 articles meeting the inclusion criteria and selected for inclusion in the scoping review. Of the included studies, 22 were randomized controlled trials, two were cohort studies, one was a prospective pilot design, and one was quasi-experimental. The process for the selection of articles is depicted in the PRISMA flow diagram (Fig. 1).
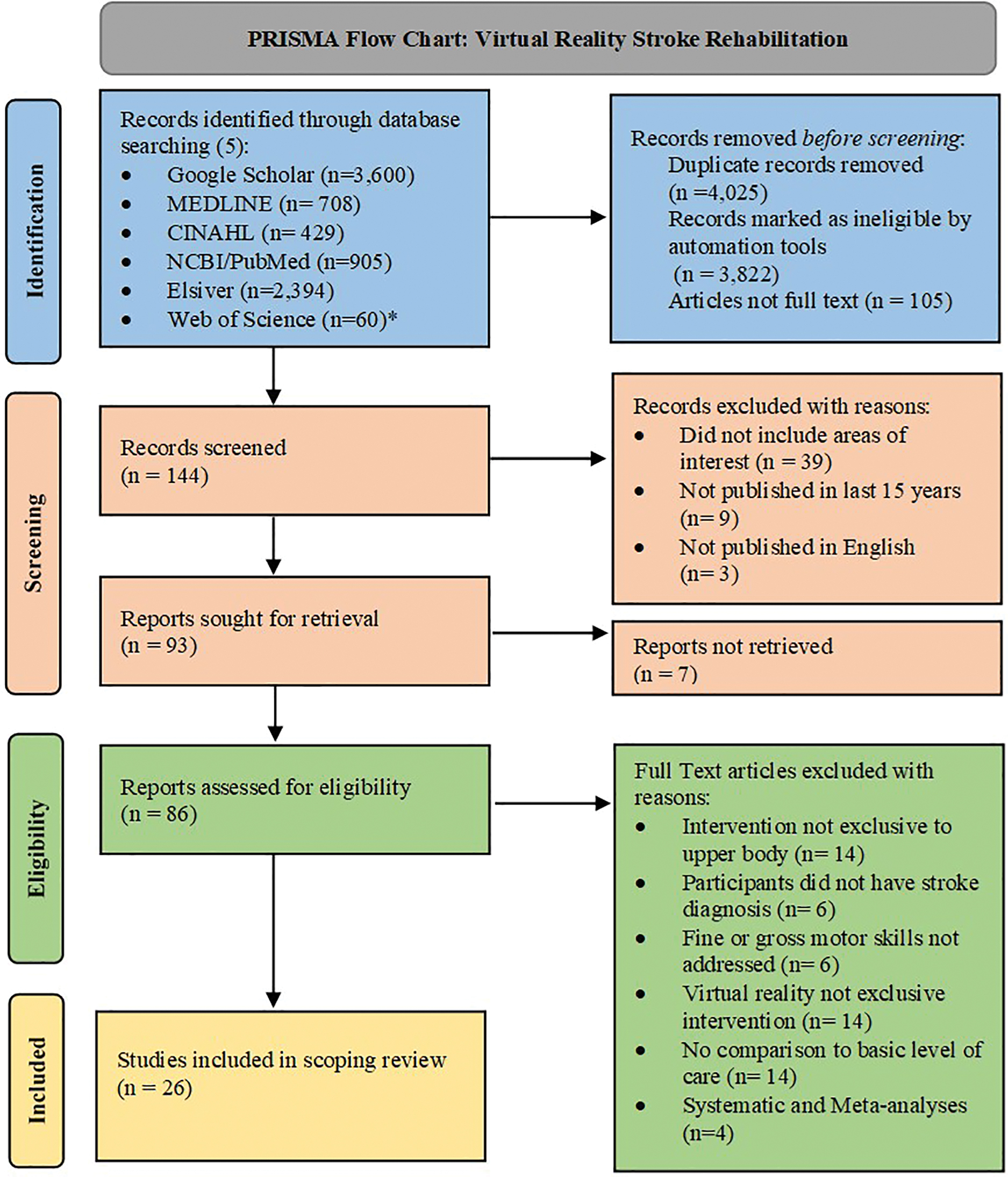
PRISMA flowchart for data collection process of VRI and its impact on UEfxn in stroke populations. *Second literature search of denoted database using additional publication year (2022–2022) search criteria. PRISMAUEfxn, UE function; VRI, VR intervention. Color images are available online.
Three main themes emerged from our extracted data regarding the effect of VR on the UEfxn of individuals poststroke, including the OM related to UEfxn, BF, and OP. The primary UEfxn assessments included Fugl-Meyer (FMA), Wolf Motor Function Test (WMFT), Action Research Arm Test (ARAT), and the Motor Activity Log (MAL). BF assessments included manual muscle testing, joint ROM, Composite Spasticity Index (CSI), and grip strength. The assessments related to OP included the Barthel Index (BI), Canadian Occupational Performance Measure (COPM), Stroke Impact Scale (SIS), Functional Independence Measure (FIM), and the Stroke Self-Efficacy Questionnaire (SSEQ).
Upper extremity function
UEfxn OM results across selected articles are displayed in Table 1. All interventions utilizing the FMA found significant increases (P < 0.05) within the UE portions of the assessment, with the majority reaching levels of P < 0.001.13,15,16,20,28–39 Da Silva Cameirão et al. 19 and McNulty et al. 21 reported the highest increases in scores with an average increase of 46.8 and 34.7, respectfully.
Upper Extremity Function Study Results
Significant value.
AOU, amount of use; ARAT, Action Research Arm Test; BBT, box and blocks test; CAHAI, Chedoke Arm and Hand Activity Index; CT, close target; CTE, close target elbow; DH, dominant hand; FMA, Fugl-Meyer Assessment; FT, far target; FTE, far target elbow; HW, hand and wrist; JTHF, Jebsen Taylor Hand Function test; MAL, Motor Activity Log; MF, motor function; NDH, nondominant hand; OM, outcome measures; QOM, quality of movement; RSPP, reaching performance scale in stroke; SD, standard deviation; SULCS, stroke upper limb capacity scale; UE, upper extremity; WMFT, Wolf Motor Function Test.
Utilizing the MAL amount of use and quality of movement, McNulty et al., 21 Borstad et al., 40 and Fong et al. 33 reported a significance level of P < 0.001, while Levin et al. 41 and Housman et al. 20 found no significant change as a result of VRI. Five studies found significant change in UEfxn as assessed by the WMFT, with Jo et al, 18 Borstad et al., 40 and Fong et al. 33 reaching significance of P < 0.001. 27 Levin et al. 41 had five out of six participants show improvements in UEfxn at the post-test, while using Gesture Extreme (GX) providing a nonspecific significance level.
Wittmann et al. 15 found a small change of 1.2 in UEfxn after 6 weeks, which was not significant. Three studies found significant changes in UEfxn as demonstrated by the ARAT with all studies reaching significance level of P < 0.001.39,42,43 Specifics regarding the significance and changes from baseline to post-test are shown in Table 1.
Body function
Postintervention CSI scores improved for three of the six participants in Levin et al. 41 One study that utilized the MI reported significant improvement in scores following VRI. 19 An increase in shoulder horizontal adduction and flexion, as well as elbow extension ROM was found immediately after the intervention. 1 Prange et al. 16 saw a significant increase in joint ROM using the max reach test. Significant positive changes were reported in shoulder abduction for the participants who utilized the Therapy Wilmington Robotic Exoskeleton (T-WREX) and NeuroR system.20,30 Huang et al. 36 demonstrated a significant increase in joint ROM using the HTC Vive, a wearable head-mounted VR device. Multiple studies assessed grip and while all resulted in increased grip strength, only two studies39,42 reported significant increases. BF results are shown in Table 2.
Body Function Outcome Measures
Significant value.
Partial significance.
ADB, abduction; CSI, composite spasticity index; EXT, extension; FLEX, flexion; MMT, manual muscle test; ROM, range of motion.
Occupational participation
As shown in Table 3, the BI was the most widely utilized assessment for the evaluation of changes in OP following VRI, with three studies reporting a significant increase in mean scores postintervention.19,29,31 Long et al. 29 and Mekbib et al. 31 found significant increases in postintervention measures with changes of ∼11 points and 4 points, respectively. On the other hand, Choi et al. 13 showed no significant change between baseline and post-test assessment scores on the BI.
Occupational Performance Outcome Measures
Significant value.
Median value.
COPM, Canadian Occupational Performance Measure; FIM, functional independence measure; SIS, stroke impact scale; SSEQ, stroke self-efficacy questionnaire.
Yavuzer et al. 23 used the FIM and found a mean increase of 5.5 between baseline and post-testing in the VRI group compared to 1.8 in the control group; this increase was found to be statistically significant. While Gueye et al. 32 also saw a meaningful increase in FIM scores, this change occurred in both the VRI and control groups resulting in no significant difference between groups. Change in SIS scores between baseline and post-testing was found to be significant as a result of VRI in one study. 14 Long et al. 29 found a statistically significant increase in both SSEQ and COPM median scores following VRI.
Comparison of VRI
The VRI used showed significant differences in the timing and systems used as displayed in Table 4. The variance in VRI duration varied from 10 days to 12 weeks. Individual session duration also varied from 15 minutes to 3 hours, with over half the sessions lasting between 30 and 60 minutes. The VRI that showed significant changes from baseline to post-test all used different systems, yet similarities can be found. Six studies used a wearable glove as the VRI interface; these systems included the SmartGlove, RGS, Interactive Rehabilitation and Exercise System (IREX), NeuroR, and Rapid Recovery.14,18,19,30,37,40
Virtual Reality Intervention Techniques and Timing
ADD, adduction; ADL, activities of daily living; CAREN, Computer Assisted Rehabilitation Environment; HMD, head-mounted device; IREX, Interactive Rehabilitation and Exercise System; NIVR, nonimmersive virtual reality; NW, nonwearable; PRON, pronation; RGS, Rehabilitation Gaming System; SUP, supination; T-WREX, Therapy Wilmington Robotic Exoskeleton; VR, virtual reality; WI, wearable initiation.
Four VRI used passive, full-arm devices utilizing the T-WREX ArmeoSpring, and a combination of an arm support device and the ArmeoBoom.16,20,32,43 Four VRI used the Leap Motion Controller,31,33,35,42 while another theme found was commercial gaming systems (CGS), which included the Nintendo Wii, PlayStation EyeToy, and the Xbox 360 Kinect.21,23,28,34,38,40 Finally, three studies utilized wearable head-mounted devices that created immersive VR environments for participants.31,35,36
Discussion
The primary purpose of this scoping review was to identify different forms of VR technology in rehabilitation and investigate the effects of VRI on UEfxn of the stroke population. Findings from selected articles were categorized based on OM.
Upper extremity function
The FMA was the most used OM, which is consistent with previous literature 44 ; it also showed the most significant gains in UEfxn compared to other assessments. While the WMFT, MAL, and other OM found significance, the results varied based on the intervention. When comparing interventions using the FMA, the greatest increases in scores were provided by da Silva Cameirão et al. 19 and McNulty et al. 21 ; however, nine VRI reported significance, while others were nonspecific regarding statistical significance. The most significant variables were treatment time, length of treatment, and type of treatment. The highly significant VRI included wearable gloves, touch screen computer, arm simulation, immersive environment, and CGS. The timing varied from 30 to 60 minutes per session from 10 days to 6 weeks.14,16,21,29,33,34,37–39 Due to the consistency of significance, but variability in intervention protocols, additional themes could not be concluded based on VRI timing or type.
Of the WMFT, the most significant difference from pretraining to post-training occurred with the IREX and Rapid Recovery, which are both wearable-glove VRI.18,40 In contrast, Levin et al. 41 utilized the GX, which simulates an environment on the screen to perform goal-directed reaching tasks. Abd El-Kafy et al. 43 and Fong et al. 33 utilized the ArmeoSpring and Leap Motion Controller, respectively, to engage in goal-directed computer games that engaged functional movements to participate. While interventions were comparable, timing varied from 30 minutes to 3 hours per session over 2–12 weeks within the significant intervention, which makes it difficult to evaluate themes.18,30–33,35,40,42,43 There were small and insignificant changes shown in WMFT scores that utilized the ArmeoSenso. 15
The MAL scores included in this review varied in significance, but McNulty et al. 21 and Borstad et al. 40 showed the most significant changes in UEfxn. McNulty et al. 21 utilized a Nintendo Wii for 60-minute sessions for 10 days. Borstad et al. 40 provided similar time periods to McNulty et al. 21 as 10 treatment days were used. In contrast, Rapid Recovery was the console used for 3 hours of treatment. 40 The use of the GX showed no significance; however, the participants did report increased motivation to improve their UEfxn when using the VR technology.18,21.41
Recent studies incorporated the ARAT with Lam et al. 39 demonstrating the most significant score increase, however, the ARAT was infrequently used in this review. Common VRI equipment such as Armeo devices and Microsoft Kinect have a greater focus on proximal UE movements (e.g., shoulder flexion, elbow extension) compared to distal UE movements such as grasp and pinch. Sixteen of the 19 tasks of the ARAT involve distal UE functional movements. 45 While proximal UEfxn is also evaluated during the ARAT, the emphasis on distal UEfxn may have influenced researchers to select other OM.
Similar reviews had differing outcomes. Laver et al. 46 included 19 trials and found statistically significant increases in UEfxn. Laver et al.2,47 differed as up to 75 trials were included, both reporting no significant change when using VRI or when comparing VRI to conventional training. Specifics found within each article reported specific VRI consoles had increased significance compared to CGS and higher doses showed a significant change in arm function.2,46,47
Body function
Significant improvement in elbow flexor spasticity was demonstrated by the CSI in patients after using the GX VRI. The unconstrained movements in multiple joint planes of the GX VRI are a possible explanation for the significant improvement in spasticity levels. 41
The CAREN software was used to assess ROM showing a gain of shoulder horizontal adduction and flexion postintervention, while an improvement in elbow extension was found 3 months afterward. 1 The ArmeoBoom intervention assessed the participant's reach distance and found a statistically significant increase was achieved postintervention. 16
Significant improvement in ROM was demonstrated after the T-WREX VRI, which utilizes a five-degree of freedom arm orthosis that allowed individuals to exercise their affected UE by playing computer games in a gravity-supported position using a custom grip sensor to detect finger movement and allow incorporation of grasp and release to facilitate arm training. The gains made in grip strength as a result of intervention were found to be insignificant. 20
Huang et al. 36 utilized the HTC Vive to create an immersive VR-based motor control training program, which demonstrated a significant increase in active ROM, post-VRI, for shoulder flexion, elbow extension, forearm pronation and supination, and wrist extension.
The NeuroR system utilized a physiotherapist who assisted in passive ROM of shoulder flexion and abduction of the affected arm in which the VR technology mirrored their movements. The participant then completed these movements independently with visual feedback from the device. As a result, shoulder abduction and flexion made significant ROM gains. 16
Five studies20,33,39,42,43 utilized grip strength as an OM and while all studies resulted in measurable increases in grip strength, only two articles reported significant increases.39,42 Considering functional movement restoration is the primary objective of most VRI, it is understandable that insignificant strength gains may be achieved. 33
In another scoping review, 26 studies were reviewed to compare VRI versus conventional interventions, which reported to have a significant increase in BF. An increase in BF led to a decrease in limitations impacting everyday occupations. 48
Occupational participation
Nearly all studies included in this review showed statistically significant results indicating improvement in OP after VRI. The results show that immersive technologies that allow participants to engage in functional tasks create an opportunity for UEfxn and BF improvements to translate to everyday occupations. In addition, task-oriented and repetitive training is a common component of most VR technologies used in rehabilitation; previous research has shown that these techniques are highly effective for the relearning of movements in poststroke.5,12
A previous scoping review highlighted specific areas of occupation that responded most to VRI and found that resulting increases in muscular strength and tension contributed to greater mastery of ADL tasks and routines. 5 The greatest improvement in OP in this review was in Long et al. 29 The intervention used within this study set it apart from the others as it incorporated movements necessary for the completion of daily tasks, such as bilateral upper limb flexion, abduction, and pinching activities. Significant increases in COPM, SSEQ, and BI scores suggest that VRI geared toward common functional movements result in increased self-efficacy and improved overall OP. 29
Limitations
The limitations of this review are related to the small sample of included research articles, resulting in decreased generalizability. The assessments utilized across studies were not universal; therefore, grouping into OM groups was necessary and may have resulted in error. In addition, due to the specific eligibility criteria and study selection process utilized, some studies with significant findings may have been overlooked. Finally, as the purpose and priority of this review were to construct a comprehensive overview of findings related to the topic of VRI and its impact on UEfxn poststroke and the nature of scoping reviews, the methodological quality of selected articles was not systematically assessed and did not limit search criteria; therefore, possible biases may have occurred.
Conclusions
This scoping review found a variety of VRIs with mixed OM. While some assessments and interventions found insignificant changes in UEfxn, other studies had promising outcomes. In addition, the lack of comparable interventions or duration among studies leaves a gap in the literature to draw a reliable conclusion related to definitive recommendations of VR gaming interventions to treat stroke-related UE deficits.
With the findings related to increased UEfxn from VRI, future research should investigate the advantages and disadvantages of these various interventions, as well as address the use of different consoles regarding features like wearability, immersiveness, and recommended timing for VR rehabilitation. Additional comparison between conventional OT and new trends such as VR should be evaluated as well. Exploring innovative intervention methods, such as VRI, has the potential to increase UEfxn, BF, and OP for individuals with stroke deficits.
Footnotes
Acknowledgments
The authors of this review would like to thank the valuable knowledge and support of the Occupational Therapy Program and University Libraries at Murray State University.
Authors' Contributions
K.B., C.B., J.R., and K.R.: conceptualization, methodology, investigation, resources, data curation, writing–original, writing–review and editing, and visualization. K.L.T.: investigation, data curation, writing–review and editing, supervision, mentorship, and project administration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.