
Abstract
Introduction:
Early mobilization after surgery is crucial for reducing postoperative complications and restoring patients' fitness and ability to care for themselves. Immersive, activity-promoting fitness games in virtual reality (VR) can be used as a low-cost motivational adjunct to standard physiotherapy to promote recovery after surgery. In addition, they have potentially positive effects on mood and well-being, which are often compromised after colorectal surgery. The purpose of this pilot study was to evaluate the feasibility and clinical outcomes of a VR-based intervention that provides additional mobilization.
Methods:
Patients undergoing curative surgery for colorectal cancer were randomly assigned to an intervention group or a control group. Participants in the intervention group (VR group) received daily bedside fitness exercises using immersive, activity-promoting, virtual reality fitness games in addition to standard care during their postoperative hospital stay.
Results:
A total of 62 patients were randomized. The feasibility outcomes were in line with the predefined goals. In the VR group, an improvement in overall mood (+0.76 points; 95% confidence interval [CI] 0.39 to 1.12; P < 0.001) and a shift toward positive feelings were observed. The median length of hospital stay was 7.0 days in the VR group compared with 9.0 days in the control group, but the difference (2.0 days) did not reach statistical significance (95% CI −0.0001 to 3.00; P = 0.076). Surgical outcomes, health status, and measures of distress did not differ between groups.
Conclusions:
The study demonstrated the feasibility of a VR intervention that improved overall mood and showed a desirable effect on feelings and length of hospital stay after colorectal surgery. The results should stimulate further research investigating the potential of VR as an adjunct to physiotherapy to enhance mobilization after surgery.
Introduction
Early postoperative mobilization after major abdominal surgery is one of the most important measures to restore a patient's physical capacity.1,2 Prolonged bed rest and immobilization after surgery are important risk factors for pulmonary and thromboembolic complications, which are associated with poorer overall survival, higher recurrence rates, and reduced long-term quality of life.2–6
In addition, a delay in mobilization and early postoperative rehabilitation may have a negative impact on the length of hospital stay, as the ability to self-mobilize and independence from external assistance are often considered as important criteria for discharge. 7
Therefore, early mobilization after surgery is recommended by the Enhanced Recovery After Surgery (ERAS®) Society guidelines for most gastrointestinal malignancies, including colorectal cancer.7–9 Mobilization usually starts on the same day as surgery and consists of activities such as sitting, standing, walking, or passive mobilization, depending on the extent of surgery and the patient's individual health and comorbidities.7,10
Studies found that early mobilization goals after upper abdominal surgery and after colorectal resections were not met in the first few days after surgery and differed greatly from guideline recommendations.11,12 Lack of staff and mobilization support has been identified as the underlying cause of insufficient physiotherapy and mobilization in patients undergoing abdominal surgery.11,13,14
Providing adequate physiotherapy after major abdominal surgery is particularly time-consuming and requires a high level of staffing as this group of patients requires intensive mobilization support and most of these patients are dependent on assistance in the first few days after surgery.11,13 In addition, patient-related factors such as fatigue and reduced strength may further reduce the amount of physiotherapy and mobilization performed.15–19
Given the financial and patient-related burdens, cost-effective, motivating, and technology-enabled alternatives for physical therapy and rehabilitation are being explored.
Virtual reality (VR) is a technology that visually, aurally, and haptically simulates a real-world environment.20,21 VR applications are being studied in various clinical contexts and have attracted much attention as effective and low-cost interventions, particularly for treatment of various psychiatric disorders, distress, and acute and peri-interventional pain and for improving emotional well-being, mood, and quality of life.22–26
Visual, auditory, and haptic stimuli, as well as interaction with the virtual environment, create immersion and evoke the feeling of being in the virtual scene often referred to as “presence” in the virtual environment. Emotions elicited by the VR experience can further contribute to this feeling.
Activity-promoting videogames are a subset of videogames that have gained popularity over the past 20 years. These games are usually played with a game controller in each hand, and the game tasks are executed by moving the upper body, shoulders, arms, and legs and other body parts depending on the game. During game play, energy expenditure and heart rate increase in a manner similar to physical activity of similar intensity in the real world.27,28 These games, originally developed for mass entertainment, have the potential for application in the prevention and rehabilitation of a variety of diseases.
In a rehabilitation or exercise setting, fitness games have the advantage over conventional rehabilitation and fitness exercises, in that they are actual games that provide fun and enjoyment, which can increase motivation and compliance.29,30 Compared with conventional physical therapy, fitness games are at least as effective in many cases and are often more motivating and engaging for patients with physical impairments. 31
Rationale for a Pilot Trial
The VR experience in combination with the gaming experience could contribute to motivation and compliance, thereby improving mobilization and thus reducing the risk of postoperative complications and positively impacting length of stay. In addition, VR-based fitness games could have a positive effect on the well-being and quality of life of patients.
Currently, there is no data on the use of VR-based fitness games in the early postoperative period after colorectal surgery. There is no data available to estimate the effect size and thus enable a high-quality sample size calculation. Therefore, this pilot study aims to investigate clinical and feasibility endpoints of the proposed intervention.
Our aim is to assess whether the design and protocol used will prove useful in terms of patient recruitment, patient compliance, and patient acceptance of the intervention and whether the intervention will have an impact on general health, patient satisfaction, length of stay, and complication rates in the VR group compared with the control group after surgery for colorectal cancer. The impact of the intervention on mood, feelings, and vital signs will be assessed within the VR group.
Methods
This pilot trial was a randomized controlled trial with a 2-arm design. The trial was conducted at the Department of General, Visceral and Transplantation Surgery, University Hospital Augsburg, Germany. The study protocol was approved by the Ethics Committee of the Ludwig Maximilian University Munich, Germany (reference number 20-1042).
The trial was prospectively registered in a primary registry of the World Health Organization (WHO) Registry Network (German Clinical Trials Register, registration number DRKS00024888) on April 13, 2021. The flow chart of the trial is shown in Figure 1. The study protocol has been published previously with open access. 32
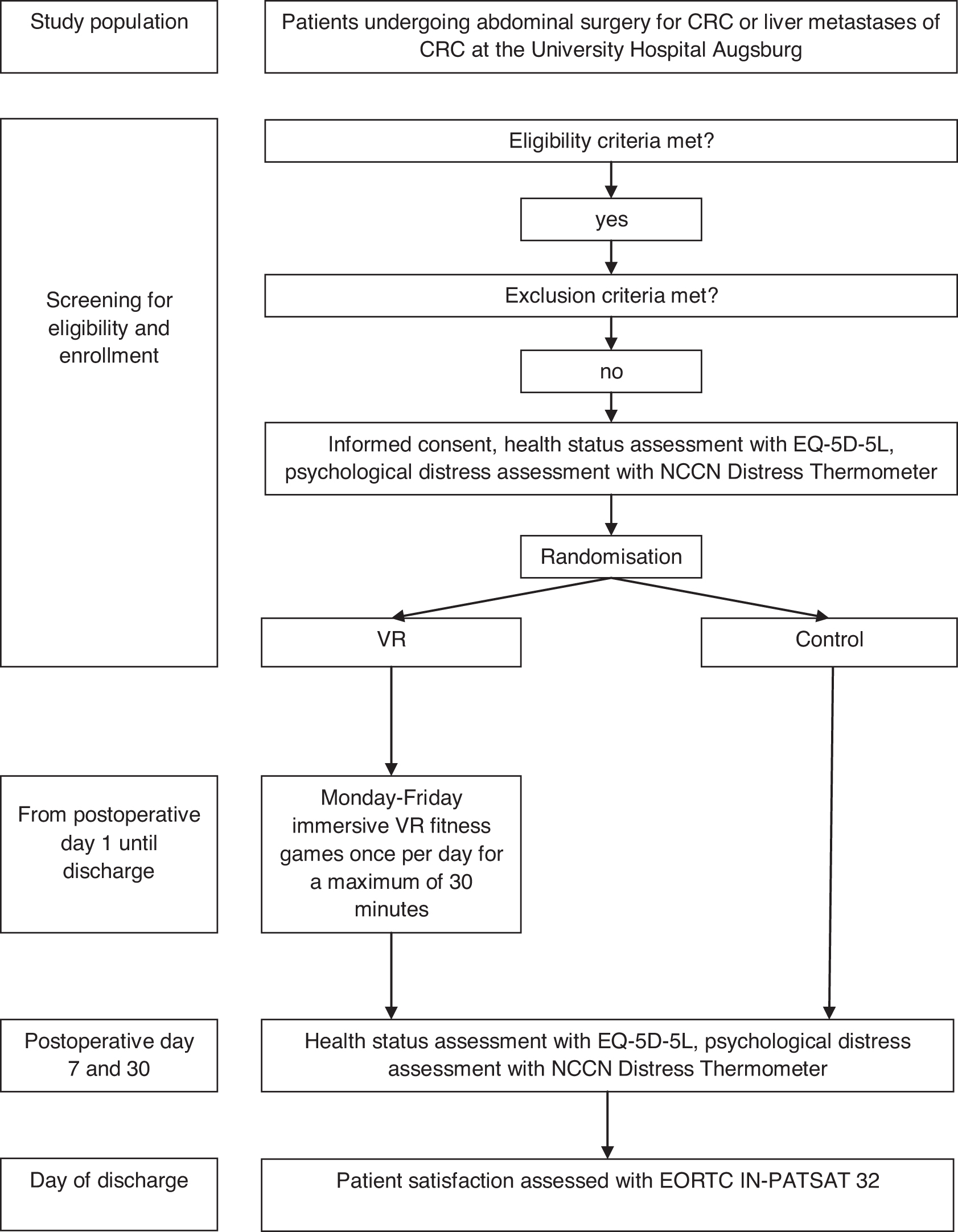
Trial flow chart. CRC, colorectal cancer; EORTC IN-PATSAT 32, European Organisation for Research and Treatment of Cancer inpatient satisfaction questionnaire; EQ-5D-5L, European Quality of Life 5-Dimension questionnaire; NCCN, National Comprehensive Cancer Network; VR, virtual reality.
Participants
All participants provided written informed consent before their participation. Adult patients undergoing curatively intended surgery for biopsy-proven or clinically suspected colorectal cancer, Union for International Cancer Control (UICC) stages I–IV, with a maximum age of 75 years, were eligible for participation. Exclusion criteria were inability to provide written informed consent, pregnancy, and participation in other intervention studies with a possible influence on the endpoints of this study.
Patients with a history of dementia, schizophrenia, hallucinations, panic attacks, or epileptic seizures and wearers of pacemakers or defibrillators, as well as patients taking neuroleptics or antiepileptic drugs, were excluded from the study. Further exclusion criteria were active alcohol and/or drug abuse, heart failure New York Heart Association (NYHA) class ≥3, chronic obstructive pulmonary disease (COPD) ≥GOLD 3, myocardial infarction within the last 3 months, untreated cardiac or pulmonary disease, and musculoskeletal conditions that limit the age-appropriate range of motion of the upper body, arms, shoulders, and neck.
To ensure adequate exercise capacity, patients who were unable to climb 1 floor without interruption preoperatively (metabolic equivalent threshold ≥4) or who were unable to perform light housework/gardening were excluded. 33
Randomization and blinding
Participants were randomized after written informed consent had been provided and exclusion criteria had been reviewed. Randomization was performed through an online randomization service with an allocation ratio of 1:1. 34 Block randomization with a variable block size was performed to ensure equal-sized groups.
Randomization was performed by staff not involved in data collection and the care of the study patients. The study design did not allow for blinding of participants and staff conducting the VR sessions. However, staff involved in the treatment and medical care of patients were blinded to the intervention, as were the staff assessing the outcomes, which were not recorded during the VR sessions.
VR group
Starting on the first postoperative day, participants assigned to the VR group were offered a VR-based, activity-promoting fitness session on weekdays, in addition to their standard physiotherapy. The VR sessions were conducted in a seated position, with participants wearing an Oculus Quest 2 VR headset (Facebook Technologies LLC, Menlo Park, CA, USA) and an Oculus controller in each hand, using the Holofit app from Holodia (Holodia, Strasbourg, France).
Game tasks such as rowing or cycling in a virtual environment required active movement of the upper body, arms, shoulders, and hands, promoting active mobilization. VR sessions were supervised for the first 10 minutes to ensure participants performed the game tasks correctly, and vital signs were measured at the beginning of each session and after 10 minutes to ensure appropriate exercise intensity in accordance with American Heart Association recommendations (www.heart.org).
A more detailed description of the intervention has been published in the Methods section of the published protocol. 32
Control group
Participants in the control group did not receive any additional VR sessions besides standard physiotherapy, which is described in the published protocol. 32
Outcomes
Feasibility outcomes
Feasibility outcomes included participation, recruitment, and adherence rates; questionnaire compliance; and occurrence and nature of adverse events.
Clinical outcomes
Clinical outcomes included differences in perioperative surgical outcomes, length of hospital stay, overall health, distress, and patient satisfaction between the two study groups, as well as changes in vital signs, mood, and feelings before and after each session within the VR group. General health and distress were assessed at admission and on postoperative days 7 and 30. Patient satisfaction was evaluated at discharge.
Mood, feelings, and vital signs were measured immediately before and after each intervention. Health status, also referred to as health-related quality of life (HRQoL), was assessed with the use of the European Quality of Life 5-Dimension (EQ-5D-5L) questionnaire. 35 The EQ-5D questionnaire comprises a descriptive system with five dimensions and a visual analog scale (0–100, 100 indicating the best health status).
The National Comprehensive Cancer Network® (NCCN®) Distress Thermometer (scale 0–10), version 2.2020, was used for assessment of distress (available online at www.nccn.org). Patient satisfaction was measured using the European Organisation for Research and Treatment of Cancer (EORTC) inpatient satisfaction 32-item questionnaire and scored in accordance with EORTC recommendations.36,37
Sample size estimation
Given the lack of data to accurately calculate the sample size, the recommendations for calculating the sample size in pilot studies were followed and based on mean and standard deviation (SD) of the length of stay in our own patient population. 38 A target reduction in the length of stay of 2 days results in a standardized effect size of 0.21.
Whitehead et al. recommend having n = 28 cases per group for pilot studies, with a standardized effect size of 0.2 and a subsequent study with a power of 90%. 38 To account for possible dropouts, 3 additional patients per group were recruited, resulting in a total number of 31 patients per group (total number n = 62).
Statistical analyses
Continuous data are presented as mean ± SD or median with interquartile range (IQR), depending on distribution. Categorical data are presented as numbers with percentages. Approximately normally distributed continuous variables were compared using the independent t-test. Non-normally distributed continuous variables were compared using the Mann–Whitney U test.
Categorical data were analyzed using the chi-squared test. Fisher's exact test was used for categorical data if the requirements for the chi-squared test were not met. For a comparison of non-normally distributed continuous variables before and after the intervention, the Wilcoxon signed rank test was used. Binary data (such as the presence of a feeling) were compared before and after the intervention using McNemar's test. 39
Analysis of clinical outcomes was performed with averaged data per participant to control for the difference in number of measurements resulting from a different length of hospital stay in addition to the analysis of unaveraged data. A two-sided P < 0.05 was considered significant. Statistical analyses were undertaken using SPSS® for Windows®, version 28 (IBM, Armonk, NY, USA), and R, version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study population and feasibility outcomes
Between May 2021 and June 2022, 169 patients were screened for participation in the study. Of these, 69 patients did not meet the eligibility criteria. Of 100 patients eligible for participation, 29 patients did not give informed consent, resulting in a participation rate of 71% and a recruitment rate of 7.1 patients per month.
Of the remaining 71 patients, surgery was canceled for 5 patients or rescheduled at a different hospital, 1 patient was not randomized for organizational reasons, 1 patient died before the scheduled surgery, 1 patient withdrew consent before participation, and 1 patient did not undergo curative surgery. Therefore, 62 patients (25 women and 37 men) were analyzed.
A total of 176 VR sessions were scheduled in accordance with the protocol. Medical reasons and organizational reasons were responsible for 9 and 7 sessions not taking place, respectively. Of the 160 VR sessions offered, 27 sessions were declined by participants. Thus, 75.6% of the scheduled sessions were performed, and of the sessions offered, 83% were performed. There were no adverse events attributable to the VR intervention.
Questionnaire compliance for the entire study population at admission, postoperative day 7, and postoperative day 30 was 98.4%, 95.2%, and 96.8%, respectively.
Demographic, medical, and surgical data
Demographic characteristics and medical and surgical outcomes are shown in Table 1.
Demographic Characteristics and Medical and Surgical Outcomes
Data are mean ± SD or n (%) or median (IQR).
ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Comprehensive Complication Index; ECOG, Eastern Cooperative Oncology Group; IQR, interquartile range; SD, standard deviation; UICC, Union for International Cancer Control; VR, virtual reality.
Median length of stay was 7.0 days (IQR 6–12) in the VR group compared with 9.0 days (IQR 7–13) in the control group, but the difference (2.0 days) missed statistical significance (95% confidence interval [CI] −0.0001 to 3.00; P = 0.076). There were no differences in demographic characteristics, cancer stage, Eastern Cooperative Oncology Group and Karnofsky performance status, type of surgery, operative time, rate and severity of postoperative complications, and mortality.
Mood, feelings, and vital signs
The mean changes in vital signs and overall mood per participant are shown in Figure 2. In the VR group, the averaged measurements of vital signs revealed an increase in heart rate of 11.6 beats per minute (bpm) (95% CI 8.3 to 15.0 bpm; P < 0.001), an increase in systolic blood pressure of 9.2 mmHg (95% CI 7.0 to 11.3 mmHg; P < 0.001), and a slight increase in diastolic blood pressure of 4.0 mmHg (95% CI 2.1 to 5.9 mmHg; P < 0.001) after 10 minutes of exercise compared with pre-exercise measurements.
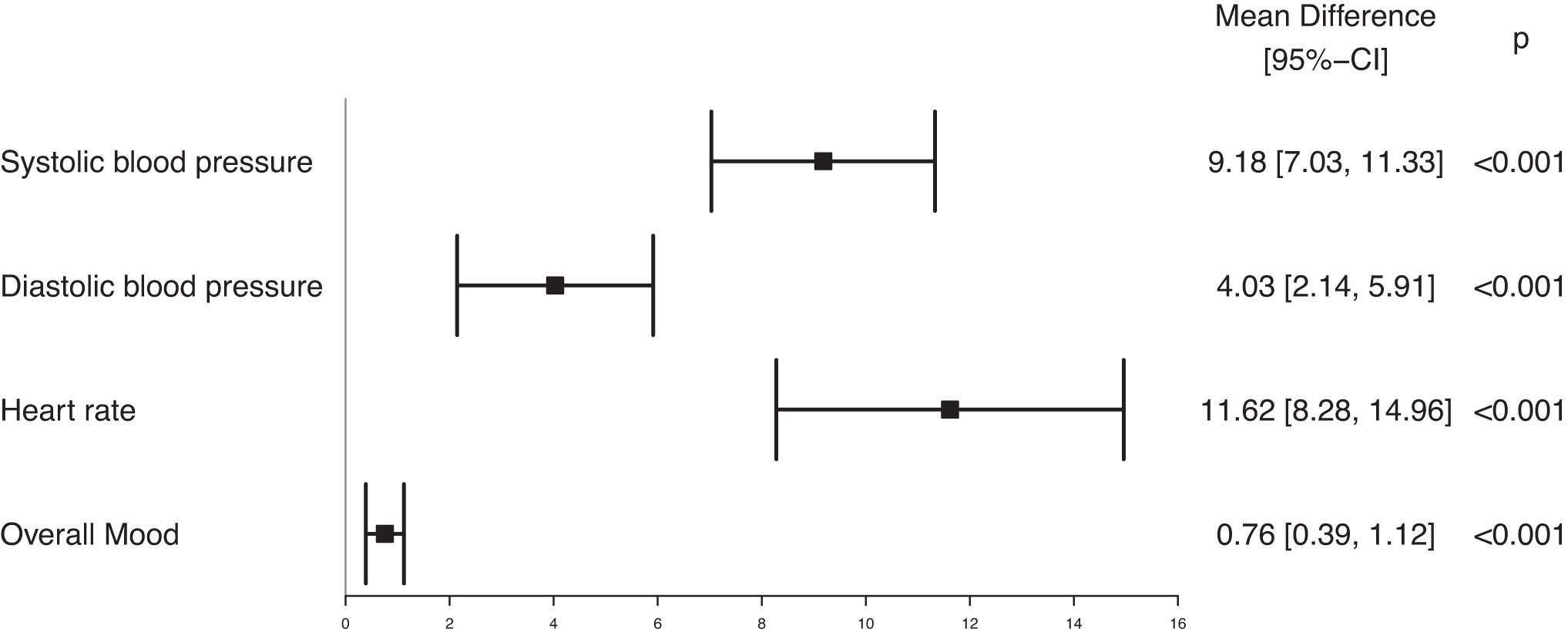
Averaged change in overall mood and vital signs after the intervention. CI, confidence interval.
Overall mood improved by 0.76 points (1–10 higher scores indicate better mood) after exercise (95% CI 0.39 to 1.12; P < 0.001). The averaged difference in the frequency of feelings per participant before and after the intervention is shown in Figure 3. On average, 20.6% of participants felt more relaxed and less tense after the VR intervention (95% CI 7.0 to 34.2%; P = 0.004), 21.6% felt more inspired and less bored (95% CI 9.2 to 34.1%; P = 0.001), and 15.9% felt calmer and less worried (95% CI 5.8% to 26.0%; P = 0.003).
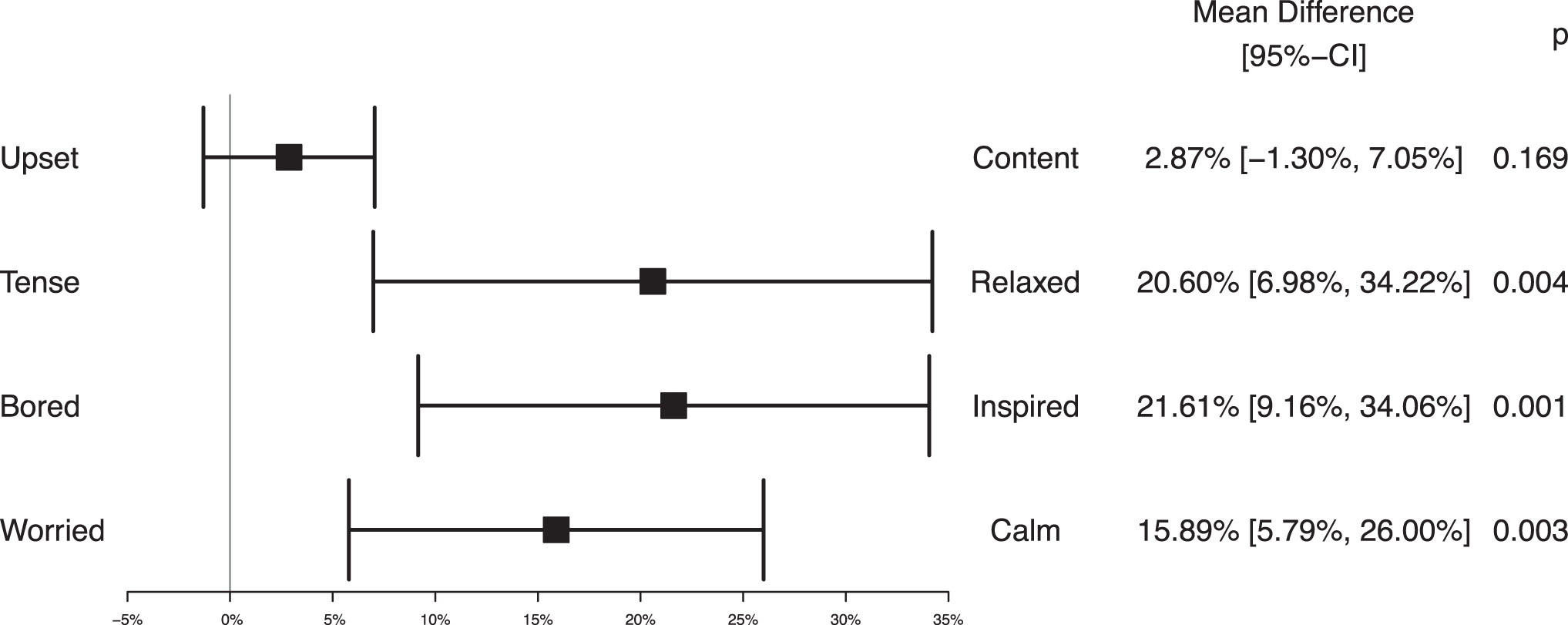
Averaged change in frequency of feelings after the intervention.
Participants did not feel more content and less upset after the intervention (P = 0.17). Similar effects in terms of vital signs, overall mood, and feelings were observed in the analysis of unaveraged data (Supplementary Figs. S1 and S2).
Health status, distress, and patient satisfaction
The mean health status on the visual analog scale was 73.6 (SD ±21.1) on admission for the overall study population. There were no differences between the VR and control groups on admission (73.7 vs. 73.5; P = 0.53), postoperative day 7 (63.3 vs. 64.3; P = 0.93), and postoperative day 30 (65.0 vs. 72.4; P = 0.28). Mean EQ-5D-5L index scores derived from the EQ-5D descriptive system did not differ in the VR group (0.90 ± 0.14) and the control group (0.90 ± 0.10) on admission (P = 0.96). Mean index scores were 0.79 ± 0.22 in the VR group compared with 0.70 ± 0.28 in the control group (P = 0.18) on day 7 and 0.83 ± 0.16 compared with 0.83 ± 0.22 on day 30 (P = 0.99).
The NCCN distress thermometer showed no differences in distress between the VR and control groups on admission (4.3 vs. 4.6; P = 0.78), day 7 (5.2 vs. 4.5; P = 0.42), and day 30 (3.8 vs. 3.9; P = 0.91). Regarding the NCCN problem list, there were no differences between the two groups in terms of practical problems, spiritual/religious concerns, family issues, emotional concerns, and physical problems.
There were no differences in overall patient satisfaction between the VR (72.6) and control (68.3) groups (P = 0.49) and in all other items of the patient satisfaction questionnaire at discharge.
Discussion
This pilot trial demonstrated the feasibility of an intervention aimed at providing additional mobilization and increasing motivation for self-mobilization by using VR technology and an immersive, activity-enhancing videogame experience.
Our self-set feasibility targets were met with a participation rate of 71% regarding recruitment and a compliance rate of 83% regarding VR interventions. Questionnaire compliance was greater than 95% at all three time points, and no adverse events attributable to the VR intervention were observed. Although not defined as an endpoint, we did not experience any difficulties in handling the VR equipment even among the oldest participants.
Although patients participated in 83% of the sessions offered, we believe there are several strategies to further increase this rate and thus patient mobilization. The extensive supervision during this study, which was necessary due to the limited experience in safety and handling of devices in this patient group, could be reduced to support as needed in further studies.
This could create a more comfortable overall experience and allow patients to decide for themselves what time of day they would like to attend their VR session as some patients refused to participate, for example, if they had a visit from family members. In addition, patients could perform the exercises at home, which is particularly important in health care systems that promote earlier postoperative discharge and shorter hospital stays compared with this study setting.
Although apps designed for mass entertainment are generally not intended as rehabilitation adjuncts, one of their strengths is that they generate motivation and fun to keep players engaged. 40 Because one of our hypotheses is that activity-promoting videogames increase motivation for mobilization by providing fun and enjoyment, compliance could be further increased by offering more game options that match personal preferences.
Interestingly, we found a significant positive change in overall mood and a shift toward more positive feelings after the intervention, with significantly more patients feeling relaxed, calm, and inspired, as opposed to tense, worried, and bored. These positive effects have been described previously for videogames as well as meditative VR applications.26,41,42
VR is known to provide a powerful distraction even during medical procedures, and it seems likely that the effect of distraction can contribute to reduction in worries.22,24 In addition, exercise itself is known to have beneficial effects on mental health and mood state, therefore it seems likely that the VR environment, gameplay, and exercise contributed to the observed changes in mood and feelings. 43
Although we found no differences in health status between the two groups, we found that the overall health status at admission among participants of this study (73.6; SD ±21.1) was lower than the published mean of an age-matched, German reference population (82.6; SD ±12.6), 44 underlining the impact of colorectal cancer on HRQoL.
In our opinion, an interesting finding is that the median length of hospital stay was 7.0 days in the VR group (mean 9.0) compared with 9.0 days in the control group (mean 12.7). Although this finding is not statistically significant, it suggests that this outcome measure should be investigated in a sufficiently powered trial.
Since this study was a pilot study, it was not sufficiently powered to test for superiority of the VR intervention with respect to clinical endpoints. This study was conducted in a selected patient population and the VR software used was not specifically designed for this scenario. Therefore, it is possible that the effects may vary in a different patient population. The exact duration of training in the VR group was not recorded as participants were allowed to train without supervision after 10 minutes of guided training.
All sessions ended after a maximum of 30 minutes with collection of the VR headsets, although some patients had already completed their sessions by this time. Of the 31 patients in the VR group, only 2 patients were physically unable to exercise for more than 10 minutes. It should be noted that although the change toward a more positive mood by 0.76 points (on a scale of 1–10) in the VR group was significant (95% CI 0.39 to 1.12; P < 0.001), the standard error of measurement of the test is unknown.
Considering the relatively low cost of the intervention, a trend toward a reduction in the length of hospital stay, an improvement in overall mood, and a shift toward more positive feelings for patients are worthwhile goals. Although activity-promoting apps and technological solutions cannot currently replace professional physiotherapy, this pilot trial suggests that there are scenarios that benefit from incorporation of activity-promoting videogames into early postoperative rehabilitation to achieve a higher level of mobilization and motivate patients to self-mobilize, as professional physiotherapy is a scarce and expensive resource in many health care systems and demand far exceeds supply in inpatient settings.
Conclusions
The study demonstrated feasibility and provided clinical outcomes for a VR intervention aimed at improving early postoperative recovery after colorectal cancer surgery. The VR intervention improved overall mood and showed a favorable effect on feelings. Although not statistically significant, there was a trend toward shorter length of hospital stay in the VR group.
The results should encourage larger, randomized controlled trials and further research investigating the potential of VR-based fitness apps as adjuncts to improve early mobilization after major cancer surgery.
Footnotes
Authors' Contributions
M.C.S. developed the study concept. M.C.S., J.Z., and S.W. designed the study protocol. M.C.S., S.W., T.T.A., G.M., and J.Z. developed the evaluation plan and conducted the statistical analysis. Data were collected by J.Z. M.C.S. drafted the initial manuscript. D.V., M.A., F.S., and S.W. critically revised the manuscript for important intellectual content. Final approval of the version to be published was given by all authors. M.C.S. and S.W. take responsibility for the work and controlled the decision to publish. The corresponding author attests that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted.
Ethics Approval and Registration
The study has been approved by the Ethics Committee of the Ludwig Maximilian University, Munich, Germany (reference number 20-1042). The trial was prospectively registered in a primary registry of the WHO Registry Network (German Clinical Trials Register, registration number DRKS00024888) on April 13, 2021. The full WHO trial registration dataset is available through the WHO ICTRP search portal (![]() ).
).
Informed Consent
Written informed consent has been obtained from all participants before participation.
Availability of Data and Materials
A fully anonymized data set and the statistical code can be made available upon justified scientific request and after ethical approval has been granted. Depending on the extent of data use and the planned research, either appropriate credit or co-authorship must be granted to the authors of this study. Any requests should be addressed to the corresponding author.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
The study was funded by a grant from the University of Augsburg (Grant No. 19034) without external funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.