
Abstract
This study examines the effectiveness of a new multi-domain multimodal cognitive training game platform, COGNIPLAT, in improving cognitive performance in elderly with mild cognitive impairment (MCI). The platform combines standard serious games and cognitive stimulation leveraging virtual and augmented reality technologies. A double-arm, evaluator-blinded randomized controlled trial was conducted with 21 elderly participants in the MCI spectrum, with 11 in the intervention group (INT) and 10 in the control group (CTL). Feasibility was assessed in terms of adherence, effective learning, and perceived usefulness. The INT attended 24 training sessions, 60 minutes long, twice a week, whereas the CTL engaged in normal daily activities and usual care. Results showed that the INT had a statistically significant change in the Montreal Cognitive Assessment score, stages List B Recall, Short-term delayed Recall, and Long-term delayed Recall of the Rey Auditory Verbal Learning Test (RAVLT), Trail Making Test-A and B test scores, Digit Span Test (DST) Forward Span, and Functional Activities Questionnaire score. A trend level difference was also found for the RAVLT Recognition and the DST Backward Span. No significant differences were found for the CTL in any of the metrics. The completion rate of the INT was 91%, and the attendance rate was 100% for participants who completed the follow-up segment of the study. The engagement level was high, and effective learning was observed between the participants. The perceived usability and usefulness of the game platform was assessed as high. This study provides evidence of a positive effect of a multi-domain multimodal-based cognitive training program in elderly with MCI, with broader benefits on cognition by inducing more cooperative transfer effects over different domains.
Introduction
Mild cognitive impairment (MCI) is recognized as a major preclinical stage in the development of progressive neurocognitive disorders such as dementia and Alzheimer's disease, and in this state people usually experience a moderate decline in cognitive skills such as memory, attention, language, executive or visual function. 1 The long phase of MCI provides a pivotal window for potential interventions that might suspend the cognitive decline process.
In recent years, the use of computer-based cognitive training has become particularly popular in the field of elderly care, including MCI interventions, because it is affordable, safe, and scalable in sustaining cognition in older adults. 2 Cognitive training typically represents a sequence of recurring and established tasks with intrinsic trials that focus on particular cognitive domains. 3 It draws on the neuroplasticity theory, which argues that external or internal stimuli can arouse the brain to adaptively modify its form and operation throughout life, including older age and during aging-related neurocognitive disorders. 4
Many of the existing computer-based training programs, including popular commercial cognitive training programs, are targeted at healthy older adults with evidence of positive results on cognitive performance whereas limited effects were reported when the same programs were applied to cognitive impaired people.2,5 On the other hand, researchers have suggested that specially designed serious games providing cognitive training activities are associated with improved cognitive function in elderly with MCI and early dementia. 6 These observations serve as motivation to research and develop new and effective intervention tools for improving cognition in such populations.
Many of the earlier studies exercised cognitive training on MCI subjects engaging a single domain, including those focused on working memory,7,8 episodic memory,9,10 executive functions, 11 and processing speed. 12 For instance, Weng et al. informed that after 8 weeks of working memory training two times per week with four main computer-based tasks, subjects with MCI presented a strong improvement in working memory function. 8
On another example, Herrera et al. disclosed that MCI subjects who attended 24 memory training sessions, twice per week for 12 weeks, significantly improved their working and episodic memory. 9 Despite the fact that loss of memory is the basic evidence of MCI, other cognitive skills such as attention, command of language, perceptual sharpness, and executive functions are commonly disturbed, and these have been linked with the detected memory shortfalls.
Although cognitive interventions based on a single domain could have their own significance as they enable the direct exploration of cognitive training gains, a multi-domain training could conceivably have broader benefits on cognition. This is due to the fact that a multi-domain cognitive training, which includes memory and other domains such as attention and execution, could induce more cooperative transfer effects over different domains than cognitive training on a single domain. 13
Such effects came to light in healthy older adults, plausibly because of the synergy across different domains for the sake of improving or protecting global cognition. For example, a study on the effects of a multi-domain cognitive training in healthy elderly reported improvements mainly on short-term memory and executive functions, and a tendency to an improvement on global cognition and non-verbal reasoning after a 3-month intervention with a frequency of one session per week. 14
Another study performed a multi-component cognitive training, which combined executive function training and memory strategy training (i.e., method of loci and face-name mnemonic) for 16 sessions over a period of 6 weeks. 15 The results showed broader training effects, including improved performance on both memory and executive function.
MCI is characterized by a reduced ability to store and retrieve information from memory and a reduced response of cognitive executive functions, such as selective attention. The ability to focus on one part of the environment and ignore irrelevant information, as well as the corresponding switch in focus when prompted, appears quite impaired in cases of MCI. For this reason, it is important for digital game design to consider the reduced ability of ignoring unnecessary information by the targeted users. Additional factors that should be considered in game design in relation to MCI include attention span, hand-eye coordination, and orientation in time and space.
This study introduces a novel cognitive training tool, known as the COGNIPLAT game platform, which has been developed specifically for elderly individuals with cognitive impairments. The game platform was designed using a human-centered approach and established learning principles, and it combines various approaches to provide a mixed multi-domain cognitive training program. An adaptation mechanism has been incorporated into the platform to tailor the training experience to the individual user.
A pilot randomized controlled trial was conducted on elderly individuals within the MCI spectrum, with the intervention group (INT) using the COGNIPLAT game platform for 24 training sessions, approximately twice per week. The results of the trial indicate that the cognitive training program resulted in statistically significant improvements in global cognition, attention, memory, and executive functions. Further, the program was found to have positive effects on mood, functional abilities, and self-efficacy.
Materials and Methods
COGNIPLAT game platform
The COGNIPLAT game platform includes serious games designed to enhance cognitive functions through exercises that focus on a variety of cognitive areas including memory, attention, perception, and executive functions. In particular, memory training is provided by games organized in cognitive domains such as short-term memory (e.g., recall exercises), working memory (e.g., calculations), semantic memory (e.g., language exercises), episodic memory (e.g., naming tasks), auditory memory (e.g., listen and remember exercises), and visual memory (e.g., memory cards). In principle, the platform was designed to support adaptive and personalized multi-domain cognitive training interventions in older adults with MCI.
A multi-domain training approach has advantages over a single-domain one, as it can match more efficiently the cognitive mechanisms supporting daily activities and thus maximize the likelihood that the outcomes of the training will be applicable in activities of daily living. 13
The cognitive training in the COGNIPLAT game platform leverages on theoretical foundations aiming at stimulating the neurobiological processes (e.g., neural network activation) that can reinforce cognitive functions. In this context, the platform design embraces well-established learning theories, including learning in context and errorless learning along with gamification learning principles, including the dynamic adjustment of the exercise's difficulty, the personalization of the training experience, and the provision of visual and vocal cueing as well as performance feedback.
The approach also includes an effective enforcement of mnemonic strategies, such as association, classification, reiteration, and naming since relevant research has shown that the use of mnemonic strategies in intervention schemes addressed to MCI patients could benefit their cognitive functioning. 16
Considering the impairment of cognitive, physiological, and sensory functions in elderly people with MCI, principles of learning in context theory 17 were explored in the design of the games. Contextual learning is associated with the implicit memory and the experiences it carries, which is believed to be better retained in older people with MCI compared with the explicit memory, which requires the conscious recall of information. 18
Therefore, there are game screens that are focusing on sociocultural memories and experiences stored in implicit memory and training is provided by simulating everyday tasks (e.g., shopping, cooking, cleaning, etc.) in an enjoyable, absorbing, and age-adapted visualization. Visual or vocal cueing is also employed as another learning in context form to facilitate task completion or object recognition. In other cases, context-based recognition in the form of a forced choice procedure (e.g., memorize images and recognize them after a while among other distracting images) is used to leverage on the reserves of memory retrieval mechanisms. 19
Another learning theory that is suitable for older people with MCI is the errorless learning theory. 20 This theory refers to a training technique in which learners are prevented, as much as possible, from errors while acquiring new knowledge. In this case, it is advisable to use various hints and appropriate aids to make the requested task as feasible as possible to be successfully completed by the subject. This approach is based on eliminating any errors during the training process and successfully completing the requested task makes the learning more robust and durable over time.
In COGNIPLAT, a more conservative approach is endorsed in the form of error reduction. Accordingly, a process was employed to reduce errors based on repetitive guidance during initial practicing with the platform and using helpful cues upon an error occurrence. Further, to minimize errors, training begins with quite feasible tasks, and exercise difficulty is increased gradually by the platform based on performance metrics.
For the design of the game screens, a human-centered design approach was followed, as this methodology is suitable for developing serious games in the domain of mental health. 21 The game design process followed an iterative approach that began with in-person meetings between the development team, domain experts in elderly and social care, cognitive psychology, and game design, as well as elderly individuals themselves.
During these meetings, the participants collaboratively identified possible interactive activities and basic mechanisms related to the interventional goals of each game. A focus group was utilized to further refine the characteristics of each game and the interactions that would empower elderly individuals during gameplay. Subsequently, rapid prototyping of game ideas and mechanisms was conducted, and the resulting prototypes were evaluated by end-users. Feedback from users regarding the game concepts and design was analyzed by the development team to determine the suitability of the prototypes. A redesign cycle was implemented to refine the game rules and interactions before final prototype development.
Each game screen was designed by following a systematic process, which involved: (1) determining the cognitive domain to be targeted; (2) selecting an appropriate interaction design method, considering the cognitive and physiological changes associated with MCI and aging; and (3) identifying the relevant variables to be monitored during gameplay. For example, impairments in vision and hearing can directly affect a player's ability to manage the game.
To address such challenges, the use of multimodal cues (i.e., visual and auditory) was considered, along with adjustments to color settings and screen lighting. In addition, feedback from the participants regarding issues such as the layout of interaction elements, colors, button sizes, and font styles was taken into consideration during the design process.
The platform development combined multiple enabling technologies, including cognitive training through stimulus in touch screens and everyday activities simulation using virtual and augmented reality (AR), to provide the user with a greater variety of interactions and exercises. By providing multimodal interactions (such as touch, voice, and movements), the platform can facilitate the implementation of game scenarios in a way that motivates and enhances users' experience while making the platform friendly to use.
In the “Supplementary Data” section, a graphical abstract is included that illustrates the fundamental components of the game platform, along with a summary of the available training tasks that are grouped based on the implementation technology that is utilized.
A cognitive training approach explored in the COGNIPLAT platform was the modeling of daily tasks in game scenarios that take place in naturalistic virtual reality (VR) worlds with a low degree of immersion. Scenarios include tasks such as preparing meals in the kitchen, picking the right bus for transportation, handling a shopping list in a virtual supermarket, performing calculations when buying everyday goods, and executive functions such as arranging clothes in a closet or books in a bookcase. It is suggested that the resemblance of such practices with actual world activities might improve training applicability by expanding the transfer of cognitive improvements to daily life. 22
The AR is used also in the form of image recognition where the camera of a mobile device (e.g., smartphone, tablet) is used to detect specific patterns (markers). With the detection of a marker, the position of the object of interest is detected and, considering the orientation of the camera, a reference point is defined, based on which digital graphics can be superimposed on the point of interest. The game scenarios developed with AR take place in the familiar space of a home and include objects and activities that are known to seniors.
In one such scenario, the elderly with cognitive impairment gets a list of items (e.g., coffee machine, milk, hand/dish soap, trash can, toothpaste, etc.) that typically have a specific location at home and the goal is to find each item in the right place using the application. For this game a marker replaces each physical object, and the user is asked to find the correct position of any object in the given list using the camera of a portable device so that the equivalent digital object appears on the screen. Moreover, the application provides helpful cues in case there is a difficulty in the progress of the game. In this game, the marker is attached to the physical object itself and operates as an indicator of the correct order of its use for the specific task.
An adaptation engine has been developed to personalize the training experience by customizing game elements such as difficulty and content. The customization mechanism is based on both static features, such as user preferences and demographic data, and dynamic data collected during the game to reflect user performance. The system adjusts task parameters such as stimuli presentation duration and volume based on user performance to keep the tasks challenging yet not overwhelming.
This mechanism leverages on a knowledge base that was developed in the form of an ontology to organize stimuli by allowing the exploitation of classifications, relationships, and properties that characterize training resources, such as images and sounds, thus facilitating the automatic creation of new exercises. 23 By combining the ontology of stimuli with the user profile, the approach allows the configuration of the difficulty of the exercises and, more generally, the personalization of the exercises. 24
Study design
This study aims at exploring the feasibility and effects of the COGNIPLAT game platform in elderly with MCI. In particular, the study compares cognitive training with the COGNIPLAT games versus usual care to investigate whether the use of the platform can lead to improved cognitive performance. The study was designed as a randomized control trial. Sample size was not estimated as the plan was to perform a pilot testing by recruiting a small sample of participants, a situation aggravated also by the consequences of the COVID pandemic. The eligible participants were randomly assigned to either the control or INT.
The study conformed to the Helsinki Declaration principles and was approved by the Ethical Research Committee of the University of the Aegean (reference no. 70682). All the participants provided their written informed consent. No reimbursement was provided to the participants to avoid any potential bias regarding the acceptance level of the intervention.
Participant flow
The participants were recruited by an elderly health care organization providing nursing, social, and caregiving services in Patras Greece. Participants were invited through social media advertisements, elderly organizations and community centers, website announcements, and telephone calls. Subsequently, potential participants were screened by qualified research assistants based on the following eligibility criteria:
Sixty-five years of age or older; MCI diagnosed in line with the Petersen criteria
25
; Cognitive assessment by means of the Montreal Cognitive Assessment (MoCA) scale
26
; with a score <26 for educational level over primary and with a score <23 up to primary, according to MoCA normative data for the Greek population
27
; Normal general cognitive functioning assessed by means of the Mini-Mental State Examination (MMSE) scale
28
; with a score ≥2429; No evidence of severe functional impairment on everyday routine activities as measured by the Instrumental Activities of Daily Living (IADL) scale
30
; with a score ≤2631; Absence of major depression symptoms as attested by the 15-item Geriatric Depression Scale (GDS-15) with a score ≤832; Absence of irreversible problems such as hearing and vision loss or any other severe disease; No recent participation in other cognitive training programs.
Depression was an exclusion criterion since it affects negatively, as an independent factor, the neuropsychological functionality (e.g., executive functions and contextual memory) and the IADL capacity in people with MCI. 33
In total, 40 subjects were assessed for eligibility and 19 were excluded due to not meeting the inclusion criteria (n = 17) or not providing written consent (n = 2). All qualified participants (n = 21) were randomly allocated to the two groups: INT (n = 11) and control group (CTL) (n = 10). The INT used the game platform on a tablet device in their home with the presence of a caregiver.
Training was performed one to two times per week until each participant completed 24 sessions. For each session, 10 tasks were allocated based on a personalized sequence to focus on relative cognitive weaknesses and lasted 60 minutes. The CTL engaged in normal daily activities and usual care. During the follow-up process, one participant dropped out early of the study (9%) due to personal reasons and was excluded from data analysis. From all the other participants, there were no missing data and cognitive and functional status assessments were recorded at the baseline and the week after the intervention was completed for comparison. The participant flow diagram is shown in Figure 1. The pilot trial from enrollment to follow-up completion was conducted between June and September 2021.
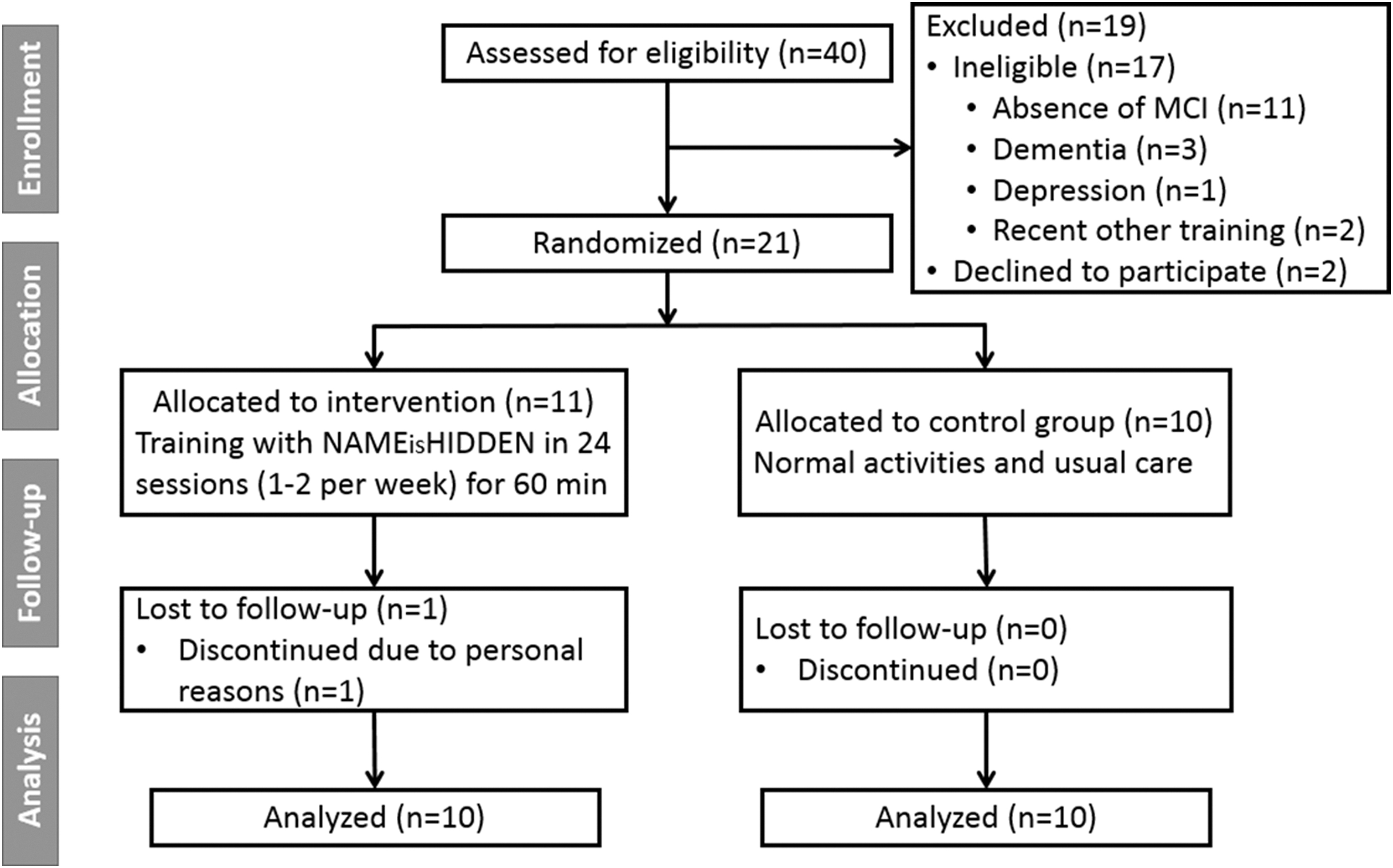
Participant flow diagram.
Feasibility assessment
Feasibility was assessed in terms of adherence, effective learning, and perceived usefulness. Adherence was evaluated by attendance and completion rates and also by the engagement level over the intervention period. Effective learning was evaluated based on the tendency of the completion time of the game tasks over time. A gradual decrease in completion time implies effective learning, as evidence that after repeated training the participants can learn to be more efficient in completing the involved cognitive tasks.
Perceived usability and usefulness were assessed using the System Usability Scale (SUS) questionnaire. 34 The questionnaire includes 10 statements, with answers on a five-point scale from 1 (strongly disagree) to 5 (strongly agree). Half of the statements have a positive meaning, and the other half have a negative meaning. The rating for each statement was transformed so that the original total scores on the 0–40 scale were converted to the 0–100 scale according to best practices. 35 An above average SUS score suggesting a good usability is a score above 68. To evaluate the usability and acceptance of the platform, qualitative data were also collected using a semi-structured interview with the participants.
Neuropsychological assessment
To evaluate the effect of the game platform on the participants, a variety of cognitive assessment diagnostic tools were employed to explore potential improvements. Except from scales evaluating global cognition, tests focusing on more specific cognitive domains such as memory, attention, and executive functions were also used. Alternative versions of tests were handled whenever available for the post-intervention assessment, to minimize learning or other transfer effects.36,37 The following battery of neuropsychological tests were used:
MoCA, 26 and MMSE, 28 which assess global cognition. According to relevant studies, MoCA is more efficient in screening for MCI in the elderly adults26,38 whereas MMSE may be more efficient in screening for dementia. 39 Therefore, in this study, MMSE is used as a supplementary cognitive assessment tool to exclude subjects with dementia.
Rey Auditory Verbal Learning Test (RAVLT), 40 which assesses episodic memory and its various components. In this study, an adaptation of RAVLT was applied in which the instructions and words are given in the Greek language. 41
Trail Making Test A and B (TMT-A/B), 42 which assesses multiple cognitive functions, including processing speed and cognitive flexibility. The TMT-A primarily measures visual-motor speed and task switching ability, whereas the TMT-B additionally assesses cognitive flexibility and working memory. The standard testing procedure was followed, with slight modifications reflecting the use of Greek language instructions and letters. 43
Clock Drawing Test (CDT), 44 which assesses cognitive functions including space perception and orientation, attention, planning, visual-motor coordination, comprehension, and execution of verbal commands. A 10-point scoring system was used with the criteria specified by Rouleau et al. 45
Digit Span Test (DST), 46 which assesses short-term and working memory, consisting of two subsections: forward digit span and backward digit span.
A comprehensive explanation of these tests is presented in the “Supplementary Data” section.
Functional and emotional status assessment
Functional status scales have a key role in assessing the effect of cognitive impairment on everyday activities in older adults as well as in evaluating potential improvements on their functional abilities as a result of cognitive training. Emotional assessment is also important to measure since higher levels of depression put the elderly at a greater risk for cognitive decline. 33 The following scales were applied:
Functional Activities Questionnaire (FAQ), 47 a self-reported questionnaire that includes ten items to measure the ability of the cognitive impaired person to handle daily activities such as managing personal finances, remembering events, and preparing balanced meals.
IADL, 30 a test of functional status examining more complex daily living tasks beyond basic ones. The validated Greek version of the IADL scale was used in the study, 48 and the scoring system applied was based on a polytomous scale. 31
GDS, 49 a self-reporting depression inventory. In this study, the short form of the scale was used, which consists of 15 questions (GDS-15) focusing on emotional states of psychological distress such as lack of help, unhappiness, and lack of satisfaction in life. The validated Greek version of the scale was applied. 50
Statistical methods
Statistical analysis was performed using SPSS Statistics (version 28.0; IBM Corp). The profile data of the participants are reported in terms of the demographic and cognitive characteristics at their measurement level. Given the limited sample size, continuous variables are stated as the median with interquartile range (IQR) whereas categorical variables are stated as frequency analysis. Differences in the profile data between the groups were compared using the Mann–Whitney U test for the continuous variables and chi-square test for the categorical variables.
To examine the difference in the cognitive measures assessed between the baseline and after the intervention, that is, the within-group effects, the nonparametric Wilcoxon signed-rank test was employed due to the small sample size. The Z-score is reported to characterize the within-group effect size. Further, the effect size of the test scores was calculated using the Cohen's d metric, adjusted for repeated measures designs (dRM), 51 with the aid of the Psychometrica program. 52
The traditional classification of Cohen's d as small (d ≥ 0.2), intermediate (d ≥ 0.5), and large (d ≥ 0.8) is used as a guide to interpret the magnitude of the effect size of dRM. The significance level of the statistical analysis was defined at a 0.05 threshold.
Results
Table 1 shows the demographic and cognitive characteristics of the randomized participants at the baseline. Most participants had a primary education and low technology familiarity. The median (IQR) age was 73.0 (5.0) years, and the median (IQR) scores for cognitive tests were MMSE 25.0 (3.0), MoCA 22.0 (3.0), GDS-15 4.0 (3.0), and IADL 10.0 (2.0). Gender was almost evenly split, and there were no significant differences between the two groups. For better understanding the characteristics of the sample, the descriptive statistics of the subjects who were not eligible for the study are also presented.
Baseline Characteristics of the Participants
Differences in the profile data between the intervention and control groups.
Mann–Whitney U test.
Chi-square test.
GDS, Geriatric Depression Scale; IADL, Instrumental Activities of Daily Living; IQR, interquartile range; MMSE, Mini Mental State Examination; MoCA, Montreal Cognitive Assessment.
Feasibility outcomes
Participants who successfully completed the follow-up had a 100% attendance rate, whereas the completion rate for the INT was 91%. Engagement was assessed using platform data, which showed an average of 24.7 (standard deviation [SD] = 0.8) sessions per participant, with an average session time of 59.9 (SD = 1.3) minutes per participant. In total, participants played 5552 games during the intervention. Illustrative snapshots of the intervention where participants were using the COGNIPLAT games are provided in the “Supplementary Data” section.
The study found that participants showed effective learning as completion time for cognitive tasks decreased progressively during the intervention period. Data did not follow a normal distribution, so median completion time was used and shown in Figures 2 and 3 for different technologies and reference time periods in the pilot study, that is, T1 (after two sessions), T2 (after four sessions), and T3 (after eight sessions). Wilcoxon signed-rank tests showed significant differences in completion time between time periods, indicating that the game tasks and screens were well designed and engaging for older adults, resulting in improved performance.
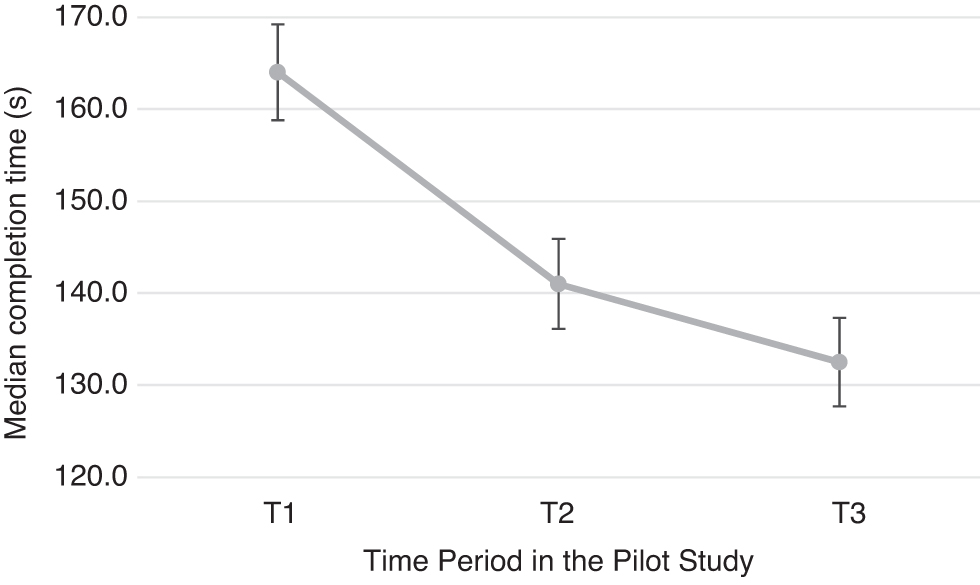
Median completion time of cognitive tasks for the intervention group in line with time. Error bars correspond to median absolute deviation divided by the square root of the number of measurements. The Wilcoxon signed-rank tests showed significant differences between T1 and T2 (Z = 4.087, P = 0.00004), T2 and T3 (Z = 3.774, P = 0.00016), and T1 and T3 (Z = 4.272, P = 0.00002).

Completion time analysis per period in the pilot study and technology. The bold line in the box of a boxplot represents the 50% percentile (the median). The top of the box represents the 75% percentile and the bottom of the box the 25% percentile.
Table 2 shows the results of the SUS for the COGNIPLAT platform, which had a mean score of 80 (SD = 8.2), indicating high user acceptance. Participants found the game tasks engaging and their objectives clear, and the platform easy to understand and use with low complexity. However, some concerns emerged regarding the need for technical support, suggesting low technological familiarity and anxiety about new technology among older adults.
System Usability Scale Results in Terms of Basic Descriptive Statistics
SD, standard deviation.
Qualitative data were obtained from a short interview with each elderly participant, which showed that the participants were highly motivated to train and enjoyed using the games. They found the games to be stable and expressed a desire to continue using them. Most of the participants (7 out of 10) believed that their cognitive function had improved, leading to a positive impact on their daily lives after the intervention.
Effects outcomes
The results of the pilot study regarding the cognitive and functional characteristics of the participants are presented in Table 3. Compared with the CTL, the INT showed a statistically significant change in the MoCA score (Z = −2.144, P = 0.032), in the stages RAVLT BR (Z = −2.126, P = 0.034), RAVLT SR (Z = −2.368, P = 0.018), and RAVLT LR (Z = −2.157, P = 0.031) of the RAVLT, in the TMT-A (Z = 2.789, P = 0.005) and TMT-B (Z = 2.772, P = 0.006) test scores, in the DST Forward Span (Z = −2.087, P = 0.037), and in the FAQ score (Z = 2.333, P = 0.020).
Effects of the Pilot Study by Group
Bold values indicate statistical significance level.
Z-score from the nonparametric Wilcoxon signed-rank test.
Effect size using the Cohen's d metric, adjusted for single-group pretest-posttest designs (dRM).
P < 0.05; **P < 0.01.
CDT, Clock Drawing Test; CTL: Control Group; dRM, repeated measures designs; DST, Digit Span Test; FAQ, Functional Activities Questionnaire; INT, Intervention Group; RAVLT, Rey Auditory Verbal Learning Test (BR: List B Recall; SR: Short-term delayed Recall; LR: Long-term delayed Recall); TMT, Trail Making Test.
A trend-level difference for the within-group effect of COGNIPLAT training with respect to the INT group was also found for RAVLT Recognition (Z = −1.701, P = 0.089) and DST Backward Span (Z = −1.800, P = 0.072) assessments. The magnitude of change is expressed by the effect size presented in Table 3. Considering that the effect size for test scores within the INT group falls into the large range, this implies that the observed differences in test scores between the pre- and post-intervention measurements are considerably meaningful and relevant in practice.
These results are indicative of the positive effect of the COGNIPLAT platform on the cognitive functions of the participants in the INT group, on the enhancement of positive emotions (as demonstrated by a 15.15% reduction in the average score of the GDS-15), and on the sense of self-efficacy (reflected in a positive attitude in the FAQ and IADL scores). The evidence that the improvement in cognitive functioning is due to the use of the COGNIPLAT platform is reinforced by the fact that the corresponding measurements in the CTL group did not show any statistically significant difference.
Discussion
The COGNIPLAT game platform improved the MoCA index for the INT, which includes tasks covering cognitive functions such as attention, memory, language, orientation, and executive functions. The game platform involves training in multiple areas, practicing various cognitive skills, which may explain the positive cognitive effect. The exercises also simulate situations that activate cognitive processes similarly to cognitive assessments.
These results are in line with the theories of cognitive plasticity, 53 according to which the elderly can improve their cognitive functions through practicing exercises that are provided by appropriately designed interventions. It can also be argued that the adaptive and personalized allocation mechanism of task difficulty in the COGNIPLAT platform serves as an additional facilitator of these neuronal plasticity processes.
A significant part of the platform's games focus on memory exercises. Memory impairment is a major symptom of MCI and therefore memory restoration is an important goal of any treatment intervention. The pilot evaluation study shows that the use of the COGNIPLAT platform improved the memory of the elderly with MCI as shown by the results of the RAVL and DST metrics. In tasks such as Image Recall, List Recall, Color Recall, Pattern Recall the participant is asked to memorize an image/word/color/pattern that appeared on the screen and then recall it immediately.
The platform operates so that if the trainee succeeds in recalling what is asked of her, the difficulty of the recall increases in subsequent rounds of the game. For example, the retention time may be reduced, or a specific image/word may be recalled after a longer period. Conversely, if the response is not successful, the retention time is increased, or the recall of a particular image/word is requested in a shorter interval.
This approach has features in common with widespread memory recovery methods such as spaced retrieval training, which is a method of learning and retaining information by retrieving them over ever-increasing intervals. 54 Such methods have been applied efficiently to patients with moderate cognitive impairment. 55 In addition, during memory training, mnemonic strategies such as word association, mental visualization, and articulation were suggested to be used by the participants.
The use of the COGNIPLAT platform had a measurable positive effect on auditory-verbal memory assessed with both the short-term and the long-term delayed recall of RAVLT. On the other hand, the evaluation showed an improvement but not statistically significant on RAVLT Recognition. Although memory training exercises were mainly based on short-term recalling, it is possible that the improvement of long-term recalling could be justified using the spaced retrieval approach, which enabled the promotion and maintenance of information.
Given that common neural mechanisms are shared between short-term and long-term memory processes, 56 it is projected that short-term memory training may have contributed to information maintenance in long-term memory. Further, the evaluation study shows also that the positive contribution of the intervention to the improvement of memory could be characterized by generality as the performance in the RAVLT test is based on the use of a set of words that are generally different from those used by the COGNIPLAT platform.
This finding is consistent with other studies that reported measurable post-intervention improvements in episodic memory and global cognition due to computerized cognitive training by means of serious games.9,57 In contrast, a study that combined cognitive and physical training for a duration of 40 weeks found measurable improvement on global cognition but not in verbal memory in patients with MCI. 58 In this case, only the long-term delayed recall was assessed and cognitive training was in the form of typical word games without specifically designed game tasks.
The effectiveness of the platform in improving memory was also assessed with the DST. DST is primarily considered a measure of working memory, although additional factors such as attention and comprehension may also contribute to performance. The Forward version of the DST assesses short-term memory, as it requires participants to recall a series of digits in the order they were presented.
In contrast, the Backward version of the DST involves active memory processing, as it requires participants to recall a series of digits in reverse order, which places a greater demand on working memory. In the evaluation, the DST Forward span metric showed a statistically significant difference for the INT, indicating an improvement in short-term memory. This effect may derive from the constant progression in cognitive training with respect to the number of stimuli to memorize.
However, the Backward span metric showed an improvement trend, which may be due to a partial transfer of the training benefits when the task is in working memory. Other studies on game-based interventions in elderly adults with MCI have also reported statistically significant improvements in the DST.7,8
Executive functions and processing speed are skills that also weaken with age and are an important area of practice for the COGNIPLAT platform, as these cognitive functions are linked to the ability to perform activities of daily living. The platform's contribution to the improvement of core executive functions was measured mainly by the TMT and secondarily by the FAQ index.
The TMT provides information on visual search speed, scanning, processing speed, and cognitive flexibility as one of the core executive functions.59,60 While the TMT can provide valuable information about cognitive flexibility, it should not be relied upon as the sole measure of all executive functions. In the evaluation study, the TMT-A and TMT-B metrics showed a statistically significant difference.
Similarly, the FAQ score showed a statistically significant difference for the INT. On the other hand, CDT scores improved only slightly. This can be attributed to the sufficiently high baseline scores together with the relatively small size of the sample.
The evaluation study showed a measurable improvement in the executive functions of the elderly with MCI when using the COGNIPLAT platform. This result may reflect the fact that the games require concentration, attention, management of information and external stimuli, and generally cognitive flexibility to complete each game successfully.
All games practice skills that include hand-eye coordination, language skills (reading, comprehension), comprehension and execution of instructions, praxis (i.e., the ability to perform handy movements indicating the function of primary sensory and motor organs), memory, constant attention, and object recognition. All these activities contribute to the mobilization of cognitive reserves in the brain, resulting in the strengthening of executive functions.
This is aligned with the results communicated in a meta-analysis studying the effect of computer- and VR-based cognitive training programs, which presented a positive impact in global cognition and executive function. 61
Overall, the findings of this study are in accordance with recent data on the effects of computer-based training interventions in MCI subjects, denoting improvement of short-term and episodic memory (RAVLT), working memory (DST), executive functions (TMT-A/B), and global cognition (MoCA), as well as a positive impact on depressive symptoms (GDS). 62
A wider perspective on the value of multiple domain cognitive interventions in the MCI population is presented by a recent systematic review and meta-analysis that reported benefits in memory, attention, and global cognition. 63 These results, which are in line with our effects outcomes, enrich the argument that computerized cognitive training in MCI subjects, which is an encouraging prospect against neurodegeneration. 64
Limitations and future perspective
Although this pilot study provides promising evidence on the feasibility and effects of the COGNIPLAT game platform, there are a number of limitations that must be considered. First, the size of the sample is small, thus limiting the ability to generalize the outcomes despite the rigorous and methodological approach followed for the study design. Due to the limited sample size, the within-group effect is only explored using a nonparametric statistical test whereas the interaction effect between group and time is omitted.
Consequently, a validation study with a larger sample size is crucial to substantiate the present findings. Second, the lack of follow-up data, due to time and financial limitations, does not allow us to draw any conclusions concerning long-term effects after the intervention. Third, the use of a non-active CTL has the limitation that it may not fully account for non-specific intervention effects, which can affect the accuracy of the results.
By including an active CTL, such as one that receives a different type of game that is not designed to improve cognitive functioning, the study would be able to differentiate with a higher degree of certainty whether the attained outcomes were caused by the effects of the COGNIPLAT game tasks used in the intervention or whether a placebo effect was obtained. Therefore, an active CTL would increase the internal validity of the study by controlling for the non-specific factors that can affect the outcomes of interest.
Finally, confounding variables that may affect the correlation between cognitive gains and cognitive training were not examined, including motivation and present activity at physical, cognitive, and social level. Novelty may confound the relationship between sleep quality and duration, as well as cognitive performance, making it difficult to distinguish the effects of the intervention from extraneous factors. This could make it challenging to establish a clear causal link between the platform and the observed improvements in cognitive function.
The COGNIPLAT platform is expanded with a VR-based cognitive-motor training that combines physical and cognitive exercises to potentially enhance cognitive function more than either type of exercise alone.
Conclusions
The objective of this study was to examine the efficacy of a multi-domain multimodal cognitive training game platform in elderly with MCI. The hypothesis was that the COGNIPLAT platform, which targets cognitive processes that are typically impaired in elderly individuals, would enhance cognitive functions. The results suggest that technology-based cognitive exercise and rehabilitation interventions, such as the COGNIPLAT platform, hold promise for delaying cognitive decline in the pre-clinical stage of neurodegenerative disorders.
The cognitive training program yielded positive outcomes in both the global cognitive index and specific cognitive domains, such as memory and executive functions, while also having a beneficial impact on mood, functional abilities, and self-efficacy. These findings align with prior research that applied cognitive exercise to rehabilitation interventions for individuals with MCI, despite sample size, duration, and methodological differences.
Footnotes
Acknowledgments
The authors wish to extend their heartfelt appreciation to the individuals who generously volunteered their time and effort to participate in the evaluation study, as well as the research assistants who contributed to the successful completion of this research. They also express their sincere gratitude to the reviewers for their rigorous evaluation of their work, which has helped to improve the quality and clarity of the manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research has been co-financed by the European Regional Development Fund of the European Union and Greek national funds through the Operational Program Competitiveness, Entrepreneurship and Innovation, under the call ERA-NETS 2018 (project code: T8EPA2-00011, grant MIS:5041669).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.