
Abstract
Purpose:
To investigate the effectiveness of virtual reality (VR)-based interventions for functional rehabilitation of the upper limb in breast cancer patients through a systematic review and meta-analysis.
Methods:
The PubMed, Cochrane, Web of Science, CINAHL, Scopus, CNKI, Wanfang, and VIP databases were systematically searched for relevant literature published from the establishment of the database to June 2023. Differences in the effectiveness of VR-based interventions and other intervention therapies were compared using random effects model meta-analysis and standard deviation (SMD).
Results:
Seven eligible articles were identified and included in the meta-analysis. The combined analysis found that VR-based interventions had a positive impact on patients' upper limb mobility in terms of flexion (SMD = 1.33, 95% confidence interval; CI [0.48–2.19], P = 0.002), abduction (SMD = 1.22, 95% CI [0.58–1.86], P = 0.0002), and external rotation (SMD = 0.94, 95% CI [0.48–1.40], P < 0.0001). In addition, VR-based interventions could significantly improve the postoperative pain of patients with breast cancer. However, in grip strength (SMD = 0.43, 95% CI [−3.05 to 3.92], P = 0.81), shoulder muscle strength in flexion strength (SMD = 0.05, 95% CI [−2.07 to 2.18], P = 0.96), abduction strength (SMD = −0.10, 95% CI [−1.32 to 1.12], P = 0.88), external rotation strength (SMD = 0.46, 95% CI [−1.96 to 2.88], P = 0.71), and lymphedema, VR was as effective as other intervention treatments. A subgroup analysis showed that patients younger than 55 years had more benefit with VR-based rehabilitation than with other interventions and showed improvements with the intervention within 2 weeks. The intervention effect of using auxiliary equipment such as robotic arms is better than VR exercise based solely on games.
Conclusion:
The results of meta-analysis show that the intervention measures based on VR have positive effects on the improvement of upper limb mobility and pain relief in breast cancer patients. However, considering the low quality of evidence and small sample size, more clinical studies should be conducted to improve the credibility of the results.
Background
Female breast cancer has surpassed lung cancer as the most common cancer worldwide, with 2.26 million new cases of breast cancer in 2020. 1 Breast cancer is characterized by both high incidence and high survival rates. For example, in the United States and Australia, the predicted 5-year survival rate of breast cancer has reached nearly 90%. 2 Although the high survival rate has led to an increasing number of breast cancer patients living longer after treatment, the long-term progression of the disease and its treatment have also brought about many adverse effects. 3 In particular, the incidence of upper limb dysfunction can reach 55.4%. 4
The process of limb rehabilitation for breast cancer patients is usually carried out through traditional physical therapy, 5 such as passive movement, exercise, and manual stretching, which have been shown to be effective in the recovery of upper limb function after surgery. 6 However, these traditional methods are time-consuming, cumbersome, and place an additional financial burden on the patient. Therefore, the limitations of traditional rehabilitation training have prompted the emergence of alternative rehabilitation approaches.
Virtual reality (VR) is a new rehabilitation approach for breast cancer patients. VR is a kind of computer simulation system that can create a virtual world for simulated experiences. 7 Users can interact with the virtual environment created by computers in many ways and achieve an immersive feeling. 8 VR can be divided into immersive, semi-immersive, and nonimmersive systems according to the different devices and systems used. Immersive systems mainly integrate users into the virtual environment through multisensory inputs, such as head-mounted displays and VR cave automatic virtual environments. Nonimmersive or semi-immersive systems include a screen or television (TV) as the output device. 9
In recent years, VR has been widely applied in many fields, such as promoting patient anxiety relief, improving poststroke motor disorders, and improving cognitive impairment. 10 For breast cancer patients, the existing systematic review focuses on the analysis of the application of VR therapy to alleviate the anxiety, depression, pain, and other emotional and psychological aspects of breast cancer patients, and the research on the recovery of upper limb function mainly focuses on stroke patients. There are still arguments and doubts about whether the VR treatment method for breast cancer upper limb rehabilitation can be equal to or even better than other physical treatment methods.
Therefore, a meta-analysis was conducted in this study to confirm whether nonimmersive VR training is effective in the management of upper extremity rehabilitation in breast cancer patients through statistical results.
Methods
Literature search strategy
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses standard guidelines for meta-analyses of experimental studies. Articles on the application of VR technology for physical training in breast cancer patients were systematically searched from the Web of Science, PubMed, Cochrane, CINAHL, Scopus, CNKI, Wanfang, and VIP databases from the time of construction to December 2022, and references of included articles were manually retrieved. The search was conducted using a combination of subject terms plus free words in a snowball search. The specific search strategy is shown in Supplementary Appendix S1.
Literature inclusion and exclusion criteria
The inclusion criteria were as follows: (1) Eligible randomized controlled trials or quasiexperimental studies that have been published. (2) Study subjects were patients with a diagnosis of breast cancer by pathology or cytology. (3) The experimental group was treated with a VR-based intervention, and the control group included any form of rehabilitation intervention such as shoulder and neck exercises or handgrip training. (4) The outcome index was any data evaluating the functional status of the upper limbs.
The exclusion criteria were as follows: (1) Duplicate published literature. (2) Unpublished articles. (3) Literature that cannot provide valid data. (4) The outcome indicators do not meet the needs of the literature.
Literature screening and data extraction
Two investigators independently conducted a primary screening based on the inclusion and exclusion criteria by reading the text title and abstract, excluding literature that did not match the study content, and then reading the full text for rescreening. When disagreements arose, the two researchers resolved them through discussion. If no consensus could be reached after discussion, a third investigator made an independent decision. After the inclusion of the literature was determined, the two investigators independently extracted and summarized the data from the literature through an Excel sheet, which included basic information about the article, trial setting, outcome indicators, and study results. Any disagreements or discrepancies regarding data extraction were resolved through discussion.
Literature quality evaluation
The quality of the included literature was assessed by two investigators independently using the Cochrane Risk of Bias tool, which assesses the literature for bias in the following six areas: selection bias, implementation bias, measurement bias, missed visit bias, reporting bias, and other biases. The evaluation criteria were seven entries, and each entry used low bias, uncertain risk of bias, and high bias to judge the quality of the studies. The evaluation of literature quality was finalized through discussion or consultation where there was doubt.
Statistical methods
All studies were statistically analyzed using RevMan 5.4 and Stata 17.0 statistical software. I2 was used to assess the size of heterogeneity; if I2 <50%, heterogeneity was small, and a fixed effects model was used; if I2 >50%, heterogeneity was large, and a random effects model was used. Sensitivity analysis was performed using the one-by-one exclusion method to compare the change in effect sizes before and after exclusion. Publication bias was evaluated using Begg's and Egger's tests, and P < 0.05 was considered the presence of publication bias. Because of the different participant characteristics and confounding factors in the study, the study was further stratified for analysis. Pooled effects were calculated using 95% confidence interval (CI) and standard deviation (SMD), and P < 0.05 was considered statistically significant.
Results
Literature search results
A total of 319 articles were obtained by systematic searches in 8 databases; 276 irrelevant articles were excluded after reading the title and abstract, 29 duplicate articles were excluded, 7 articles were excluded after reading the full text, and 7 articles11–17 were finally included for the meta-analysis. The detailed selection process of the literature is shown in Figure 1.

PRISMA flow diagram for the study selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Basic characteristics of the included literature
The basic characteristics of the included studies are detailed in Table 1. A total of 7 articles were included, published from 2016 to 2022, with 324 included cases and intervention durations ranging from 30 minutes to 3 months. Choosing to rely on VR for physical intervention, these studies assessed the impact of VR-based interventions on outcomes related to upper limb function, and due to the type as well as the number of studies, only upper limb mobility, muscle strength, and grip strength were selected for the meta-analysis in the article, and for qualitative analysis of pain as well as lymphedema.
Intervention Details and Related Results of Experimental Group and Control Group of Breast Cancer Patients
3D, three-dimensional; DASH, Disability of the Arm, Shoulder, and Hand; EAV, Arm swelling volume; KBRG, Kinect-based rehabilitation group; ROM, range of motion; SF-36, Short Study-Form; SPTG, standard physiotherapy group; TKS, Tampa kinesiophobia scale; VAS, visual analog scale; VR, virtual reality.
Results of the quality evaluation of the included literature
Figures 2 and 3 show the quality assessment of the included studies. Due to the nature of intervention implementation, the main source of bias is the implementation of the participant blinding method. Most studies did not specify the method of inclusion of study participants.

Overall risk-of-bias analysis of the included studies. Color images are available online.
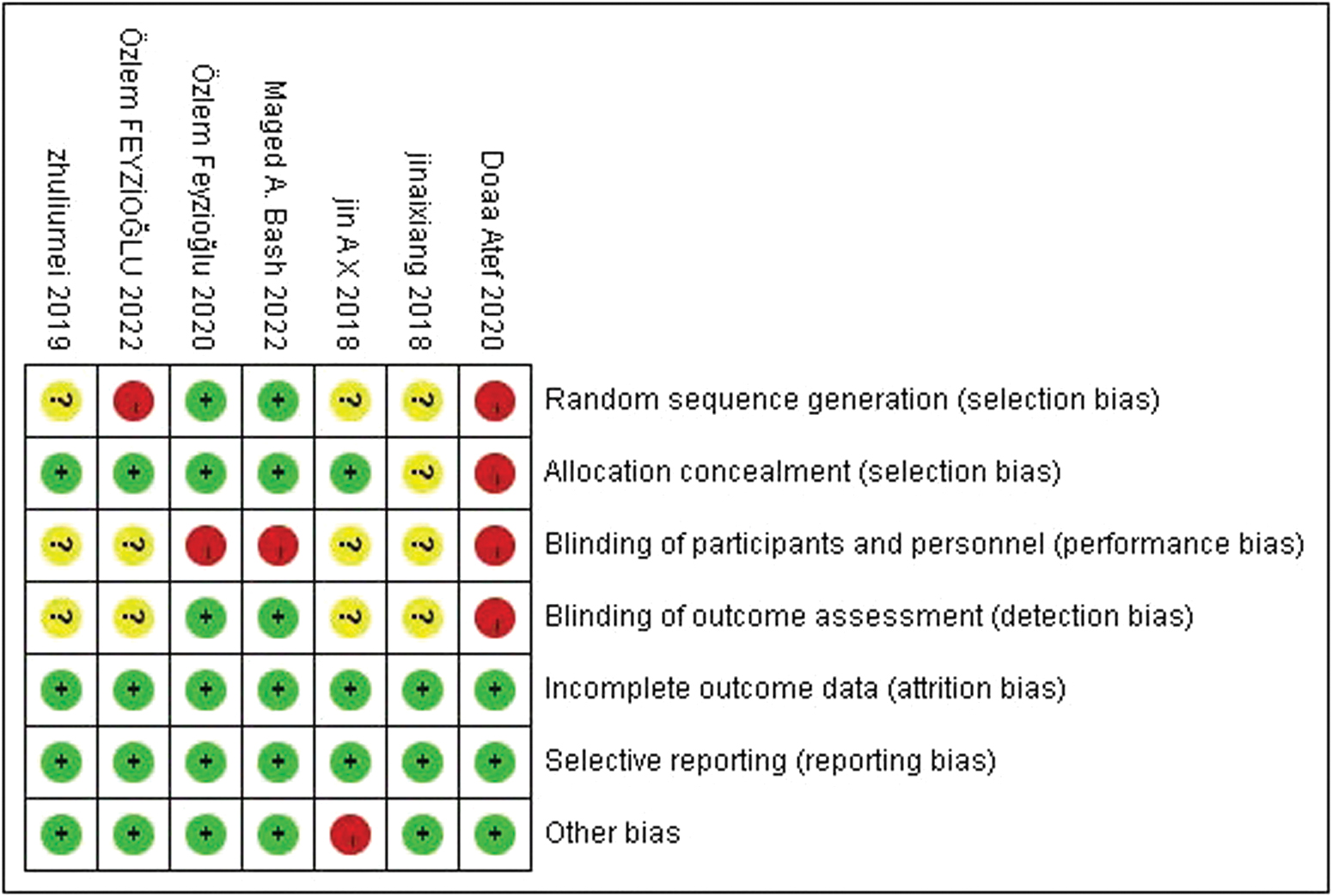
Risk-of-bias analysis of the included studies. Color images are available online.
Analysis of results
Due to the limitation of the number of studies, this study selected upper limb mobility, grip strength, and shoulder muscle strength for the meta-analysis and pain and lymphedema for qualitative analysis. For the measurement of upper limb mobility, a digital goniometer was used. For muscle strength, such as grip strength and shoulder muscle strength, a dynamometer was used for measurement in kilograms, pain was measured by a visual analog scale, and lymphedema was judged by circumferential measurement of upper arm volume.
Upper extremity mobility
Six articles were found to evaluate the relationship between each movement direction in the upper limb range of motion (ROM) and VR-based interventions. In one study, the upper limb ROM was assessed according to whether pain was present in the limb. Therefore, a total of seven studies were evaluated. The results showed that VR-based interventions had a statistically significant effect on upper limb ROM recovery. Statistical analysis indicated significant heterogeneity and positive significance in upper limb flexion (SMD = 1.33, 95% CI [0.48–2.19], P = 0.002, I2 = 89%), abduction (SMD = 1.22, 95% CI [0.58–1.86], P = 0.0002, I2 = 82%), and external rotation (SMD = 0.94, 95% CI [0.48–1.40], P < 0.0001, I2 = 68%, P = 0.004) (Fig. 4). These results are consistent with the previous review.
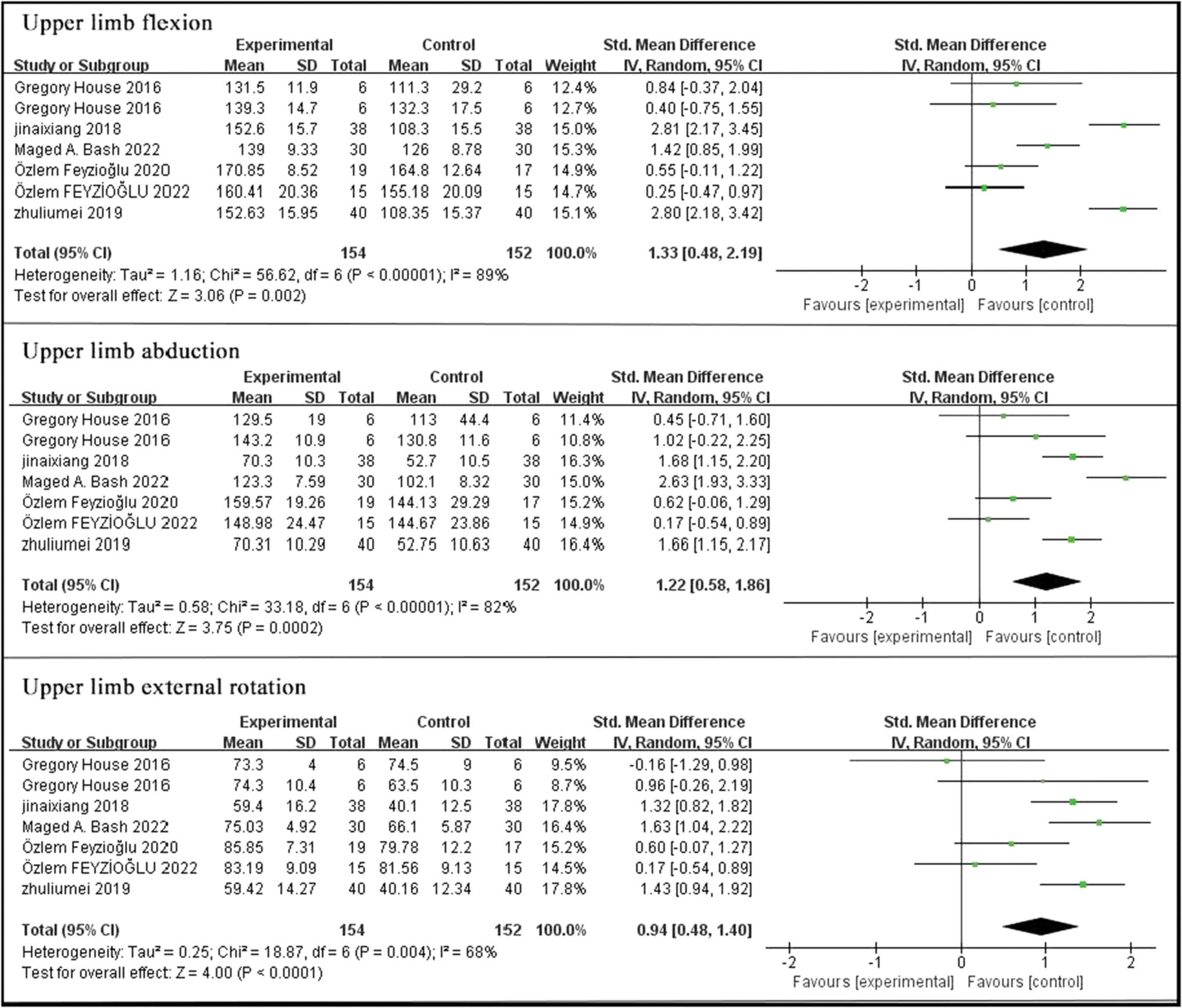
Forest plot of the effect of VR on shoulder range of motion. VR, virtual reality. Color images are available online.
Grip strength
Three studies assessed grip strength by a dynamometer and showed no significant correlation between grip strength and VR-based interventions (SMD = 0.43, 95% CI [−3.05 to 3.92], P = 0.81), with significant heterogeneity (I 2 = 71%, P = 0.01) (Fig. 5).
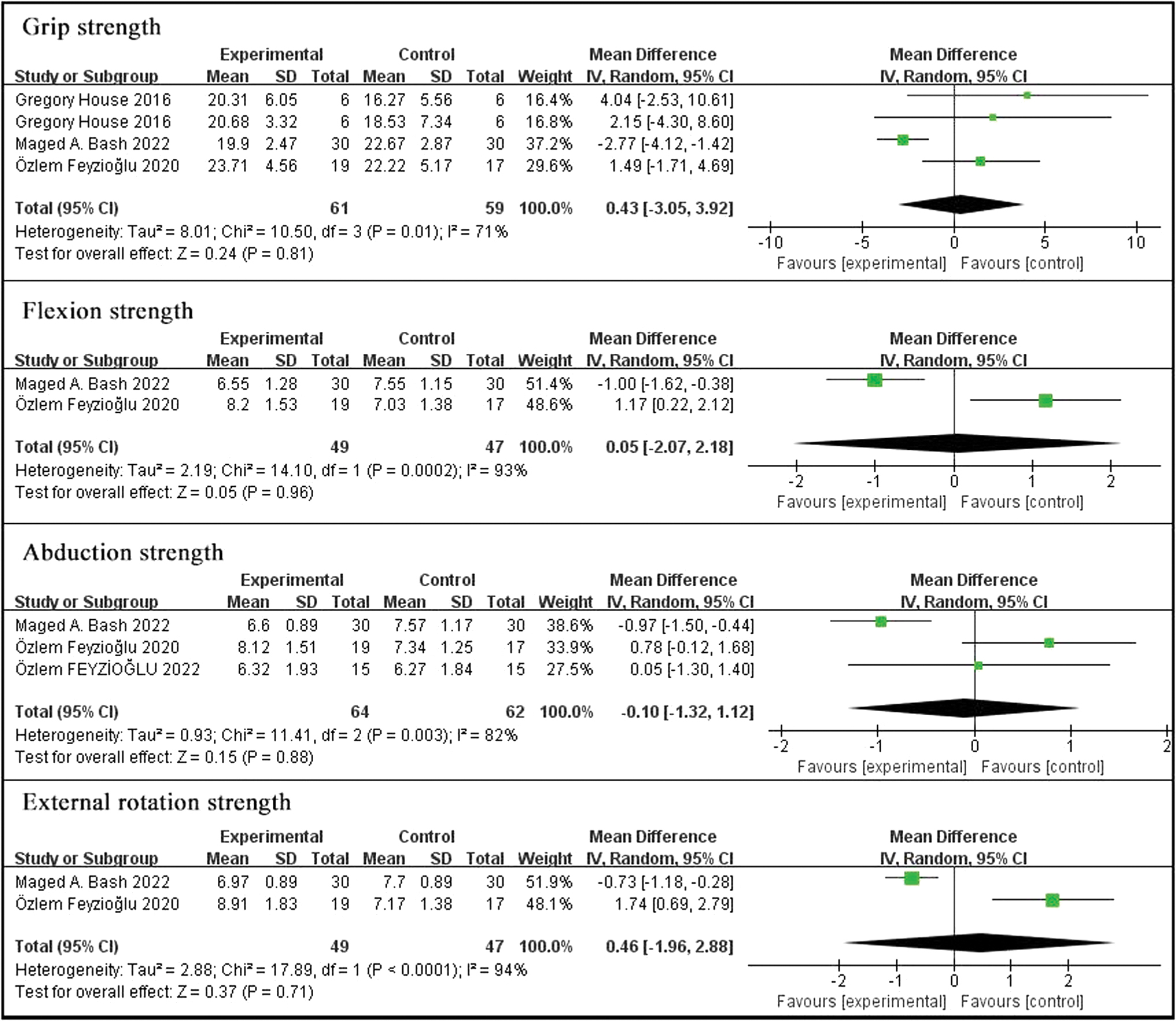
Forest plot of the effect of VR on grip strength and shoulder strength movements. Color images are available online.
Shoulder muscle strength
Shoulder flexion muscle strength was included in two studies and showed no significant correlation between flexion muscle strength and VR-based interventions (SMD = 0.05, 95% CI [−2.07 to 2.18], P = 0.96), with significant heterogeneity (I 2 = 93%, P = 0.0002). Abduction muscle strength, on the contrary, was included in three studies, again showing that VR was not helpful for abduction muscle strength (SMD = −0.10, 95% CI [−1.32 to 1.12], P = 0.88), with significant heterogeneity (I 2 = 82%, P = 0.03). The two articles on external rotation muscle strength also showed no significant correlation (SMD = 0.46, 95% CI [−1.96 to 2.88], P = 0.71), with significant heterogeneity (I 2 = 94%, P < 0.0001) (Fig. 5).
Pain
The results are mixed regarding pain. Basha et al. 13 confirmed the decrease in pain level by the visual analog scale of pain (mm), which shows a more significant reduction in VR for pain (P = 0.0001).
However, Feyzioğlu et al. 15 found in their study that in the pain levels assessed by the visual analog scale (0–10) P = 0.065 between VR and standard physiotherapy, there was no difference in the level of reduction in pain values between both, although both were reduced.
Lymphedema
Regarding the results of lymphedema, it is currently believed that either VR-based training or other physical training can reduce the degree of lymphedema, but there is no difference in the effect of the two. A study by Atef et al. 12 showed that the effect of VR-based interventions is equivalent to proprioceptive neuromuscular facilitation, except that VR is superior to proprioceptive neuromuscular facilitation in motivating patients and providing visual feedback. Likewise, Basha et al.'s 13 study determined the level of lymphedema by measuring limb volume, indicating that there was no significant difference between the two (P = 0.15).
Subgroup analysis
A subgroup analysis was conducted to test whether the association between VR-based training and upper limb mobility was different due to differences in age, the time of starting exercise after surgery, and the intervention methods of VR. 1 in the age group represents those younger than 55 years, and 2 represents those older than 55 years. 1 in the postoperative time group represents VR intervention that begins within 2 weeks after surgery, and 2 represents intervention that begins 2 weeks after surgery. Among the different intervention methods for VR, 1 represents purely game-based VR intervention, and 2 represents VR intervention using other auxiliary devices, such as robotic arms.
Age subgroup analysis
A total of seven studies were included in the upper limb mobility subgroup analysis, dividing the age groups into two classes.
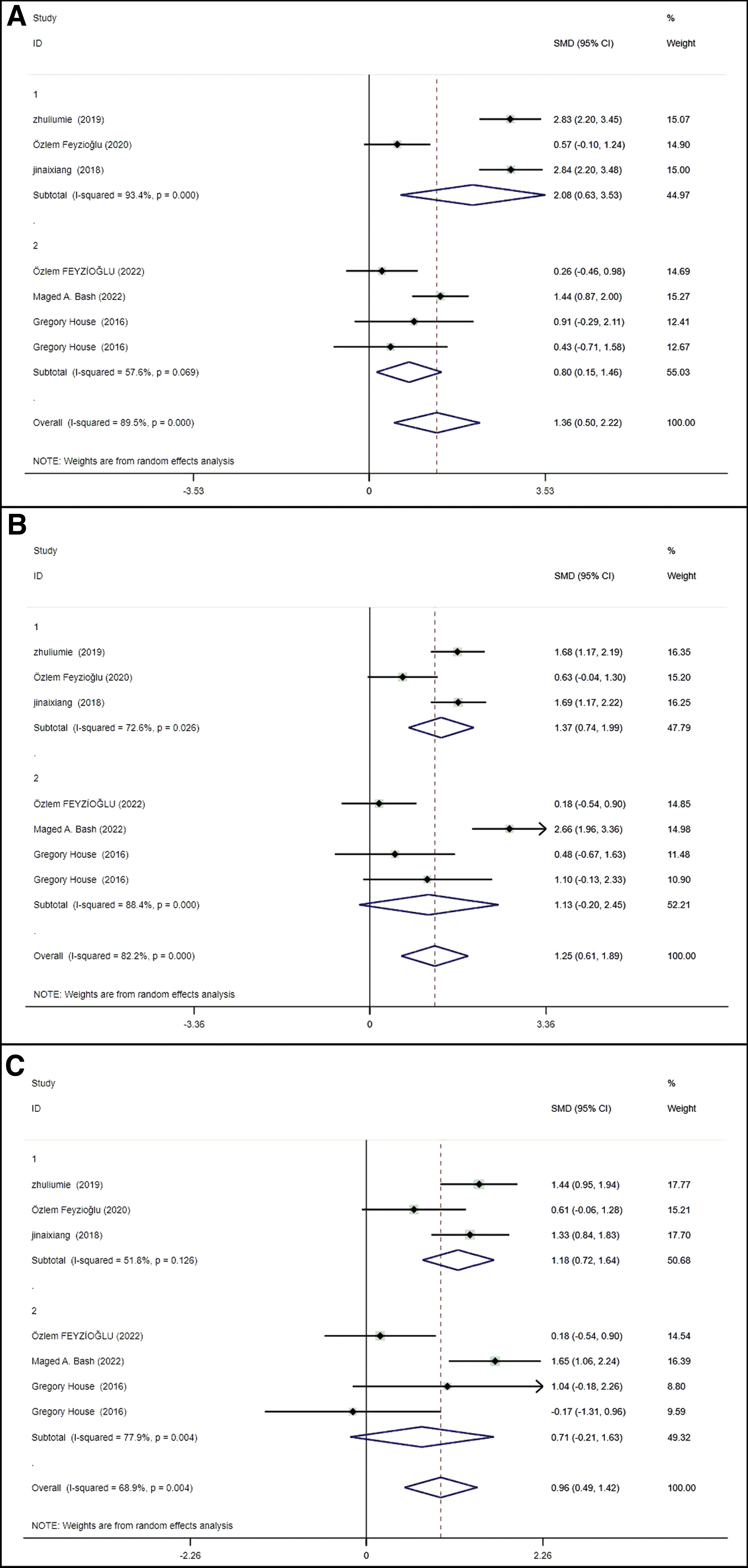
The results of the age subgroup analysis of flexion showed that the effect of VR-based rehabilitation training for patients younger than 55 years was better than that of standard physical therapy (SMD = 1.28, 95% CI [0.18–2.39], P < 0.023), and there was no significant difference between the two training methods for patients older than 55 years (SMD = 1.45, 95% CI [−0.20 to 3.09], P = 0.085) (Fig. 6A).

Forest plot shows the association between VR and upper limb by patient age.
Abduction was significant at both ages, <55 years (SMD = 1.30, 95% CI [0.28–2.32], P = 0.013) and >55 years (SMD = 1.24, 95% CI [0.51–1.97], P = 0.001) (Fig. 6B).
External rotation in the <55 years age group for VR-based interventions (SMD = 0.98, 95% CI [0.35–1.60], P = 0.002) was significantly superior to standard physical therapy. It was not positively significant at >55 years (SMD = 0.86, 95% CI [−0.12 to 1.84], P = 0.085) (Fig. 6C).
Postoperative time subgroup analysis
In the subgroup analysis of postoperative time of flexion, the experimental group that received VR intervention within 2 weeks of surgery and 2 weeks after surgery had positive significance, and the combined effect amount was (SMD = 1.36, 95% CI [0.50–2.22], P = 0.002) (Fig. 7A).
Forest plot shows the association between VR and upper limb by postoperative time.
In the subgroup analysis of postoperative time of abduction, the results showed that the experimental group with VR intervention within 2 weeks after surgery had positive significance (SMD = 1.37, 95% CI [0.74–1.99], P < 0.0001). There was no significant correlation between the experimental group with VR intervention 2 weeks after surgery and upper limb activity (SMD = 1.13, 95% CI [−0.20 to 2.45], P = 0.097) (Fig. 7B).
In a subgroup analysis of postoperative time of external rotation, there was a positive significance in the experimental group with VR intervention within 2 weeks of surgery (SMD = 1.18, 95% CI [0.72–1.64], P < 0.0001) and no significance between the experimental group with VR intervention after 2 weeks of surgery and upper limb mobility (SMD = 0.71, 95% CI [−0.21 to 1.63], P = 0.128) (Fig. 7C).
Different VR intervention methods subgroup analysis
In the subgroup analysis of upper limb mobility, both game-based VR intervention and VR intervention using assistive devices have significant positive effects, and the effect of using assistive devices is superior to that of game-based VR intervention.
The combined effect amount of upper limb flexion subgroup analysis was (SMD = 1.55, 95% CI [1.28–1.82]). The VR intervention using assistive devices (SMD = 2.34, 95% CI [1.95–2.74]) was significantly superior to the game-based VR intervention (SMD = 0.85, 95% CI [0.48–1.22]) (Fig. 8A).

Forest plot shows the association between VR and upper limb by different VR intervention methods.
The combined effect amount of upper limb abduction subgroup analysis was (SMD = 1.38, 95% CI [1.12–1.64]). The VR intervention using assistive devices (SMD = 1.54, 95% CI [1.20–1.88]) was significantly superior to the game-based VR intervention (SMD = 1.16, 95% CI [0.75–1.56]) (Fig. 8B).
The combined effect amount of upper limb external subgroup analysis was (SMD = 1.10, 95% CI [0.86–1.35]). The VR intervention using assistive devices (SMD = 1.24, 95% CI [0.92–1.56]) was significantly superior to the game-based VR intervention (SMD = 0.92, 95% CI [0.54–1.29]) (Fig. 8C).
Sensitivity analysis and publication bias
Sensitivity analysis: studies were excluded one at a time to determine if the results would change when a study was removed. The analyses all showed little difference in effect size change, suggesting robust results.
Estimates for upper limb flexion sensitivity analysis were 1.36 (95% CI 0.50–2.22) (Supplementary Fig. S1), abduction sensitivity analysis was 1.25 (95% CI 0.61–1.89) (Supplementary Fig. S2), and external rotation sensitivity analysis was 0.96 (95% CI 0.49–1.42) (Supplementary Fig. S3).
Publication bias
To test this meta-analysis for publication bias, Begg and Egger's tests and funnel plots were performed.
The results showed Begg's test P = 0.230 > 0.05 and Egger's test P = 0.124 > 0.05. The data showed no publication bias in the articles, but the results should be interpreted with caution because of the small number of included studies (Supplementary Fig. S4).
Discussion
This systematic review and meta-analysis evaluated the effectiveness of VR-based interventions in breast cancer patients. A total of seven studies were included in the article, and based on the results, it can be concluded that VR-based interventions are more effective in improving upper extremity mobility as well as pain in breast cancer patients, and are as effective as other interventions for upper extremity muscle strength and lymphedema.
Bleeding, fluid accumulation, flap necrosis, and upper limb edema often occur after radical breast cancer surgery, resulting in upper limb dysfunction, such as limited shoulder movement and limb weakness, and significantly reduce the patient's quality of life. 18 The results showed that patients recovered positively in terms of upper limb mobility compared with standard conventional breast cancer treatment, and these results are in line with previous results by Zhang et al.'s 19 review.
The difference in upper limb mobility can be explained by the fact that the virtual environment increases patient compliance and distracts patients due to its novelty and fun nature. Virtual reality combined with physical therapy reduces patients' fear of movement compared with physical therapy alone, 20 reduces pain, gives patients a pleasant emotional experience, and improves the effectiveness of interventions during their interaction with VR. 21
Pain associated with cancer can be a harrowing experience. 22 The prevalence of persistent postoperative pain in breast cancer survivors ranges from 2% to 78%. 23 Fear of exercise further increases the risk of decreased upper extremity function. 15 The research results show that intervention measures based on VR are indeed effective, but there exists doubt as to whether they are superior to other intervention methods. This is in line with Zeng et al. 24 who reported the same. However, Ahmad et al. 25 and Chow et al. 26 reported suggesting that VR-based interventions may be more effective in managing pain in cancer patients.
One possible explanation for this discrepancy is that immersion and nonimmersion systems have different intervention effects, and in addition, survivors may have different physical and psychological symptoms, pain sites, thresholds for pain perception, and levels of tolerance, leading to discrepancies in study results. Therefore, there is a need for controlled trials between different interventions and populations.
In addition, impaired grip strength due to postoperative breast cancer is one of the most common long-term sequelae in surviving women, lasting up to 6 years after surgery. 27 Decreased muscle strength can lead to impaired function and reduced quality of life. Therefore, a major goal of cancer treatment is to increase muscle strength. 28 The present study showed that VR-based training was equivalent to other physical therapies in terms of strength. This is consistent with Tian et al., who concluded that VR-based training has no effect on grip strength recovery. 29 However, contrary to the results of Obrero-Gaitán et al., 30 the discrepancy may be limited by the small sample size and the small number of studies, combined with the variability due to the different training methods of VR.
Breast cancer survivors have a lifetime risk of developing breast cancer-associated lymphedema (BCRL) 31 with an incidence of 21.4%. 32 BCRL is a chronic, potentially debilitating disease that includes progressive swelling, restricted ROM, pain, and numbness, and requires lifelong symptom management. 31 The findings suggest that VR treatment is equivalent to other interventional therapies, which is consistent with the results of previous reviews.
In addition, the degree of recovery using VR was shown to be inversely proportional to age in the subgroup analysis, and the results can be explained by the decreased physical ability and worse comprehension in older patients, and the better effect of the intervention on recovery immediately after 2 weeks postoperatively. Because the functional recovery of the affected limb after breast cancer surgery is a long-term process, early functional exercise can shorten the time of functional recovery of the shoulder joint and improve patients' motor endurance. 33 Interventions based on auxiliary devices such as robotic arms have better effects than VR interventions based solely on games. This may be because auxiliary devices can control patients' limb training process, 34 making their movements more standardized, monitoring the patients' rehabilitation trajectory, and real-time generation of various data can adjust the rehabilitation plan at any time. 35
The results of this review should be interpreted with caution due to the limited number of studies analyzed, the small sample size, and the low methodological quality. Most previous review analyses suggest that higher quality evidence is needed to determine that VR-based interventions are effective in the management of recovery in breast cancer survivors.
Limitations
The number of included studies was small, with small sample sizes, poor methodological quality, and heterogeneity. Patients also received different forms of VR treatment.
For randomized controlled trials, the nature of the intervention results in most studies is nonblind for participants and investigators, thus having a high risk of bias.
Heterogeneity was present due to inconsistency in device use, frequency of intervention, and duration among patients receiving VR interventions.
The qualitative analysis should be interpreted with caution, as it is not supported by quantitative analysis data.
Multicenter randomized controlled trials are recommended in the future to seek higher quality evidence on the effect of VR on breast cancer patients.
Conclusion
The research results indicate that VR-based interventions have improved upper limb function, such as mobility and pain levels, in cancer patients, and the improvement effect is superior to standard physical therapy. However, although there have been improvements in upper limb muscle strength and lymphedema, it is equivalent to standard physical therapy.
According to the above results, it can be concluded that VR-based interventions can help patients with breast cancer recover upper limb function in clinical practice, because VR is superior to standard physical therapy in terms of recovery of activity and pain relief.
Footnotes
Acknowledgments
We would like to thank the authors who participated in the study.
Authors' Contributions
Y.L. and W.N. contributed equally to the study conception and design, literature search, study selection, data extraction, risk-of-bias assessment, data analysis, and drafting of the article; S.Y. made substantial contributions to the conception and design of the literature search and risk-of-bias assessment; W.N., S.Y., and L.Z. participated in the study selection, data extraction, and the risk-of-bias assessment; Z.J. made contributions to the conception and design of the study selection and data analysis; P.X., as the corresponding author, made substantial contributions to the conception and design, literature search, and revision of the article for critically important intellectual content. All authors have read and approved the final version of the article and agree with the order of the presentation of the authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Jilin University Graduate Education Teaching Reform and Research Project, project number 2021JGY32. Jilin Province Health Technology Capability Enhancement Project, Project Number 2023GL006.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.