
Abstract
Background:
Premature children are at increased risk of executive functions (EF) deficits and these difficulties persist into adolescence and adulthood, potentially undermining their development and academic achievements. The aim of the present randomized controlled trial (RCT) is to evaluate the efficacy of the Intendu trainer, an adaptive virtual reality platform, at ameliorating EF in preterm children.
Methods:
A single-center, RCT was conducted. The intervention group was exposed to game session with the Intendu software in addition to the standard of care in use in our center. The main outcome was the proportion of children with a 10-point increase in the processing speed quotient as measured by WPPSI–III after 4 weeks from the baseline assessment.
Results:
Forty-seven children born before 36 + 5 weeks were randomized to the experimental (n = 24) or control arm (n = 23). Five children were lost to follow-up. Thirteen of 23 children (56%) reached the main outcome in the experimental group and 5 of 19 (26%) in the control group (P = 0.049, per-protocol analysis) with an absolute benefit increase (ABI) of 30% reconfirmed by the intention-to-treat analysis (P = 0.022, ABI of 32%).
Conclusion:
Intendu brain-trainer showed promising short-term results on EF in pre-term children, however, larger studies with longer periods of follow-up are warranted to better investigate the role of this or similar technology in promoting better EF in preterm children.
Introduction
Prematurity, defined as birth before 37 weeks of gestation, makes up from 5% to 18% of births worldwide, with low-income countries accounting for more than half of all cases. 1 Although advances in maternal and newborn care have improved the preterm infants' survival rate, a large spectrum of developmental disorders is described in these children.2,3 Specifically, neuropsychiatric deficits, such as gross motor or cognitive deficits, and also “minor” impairments, that is, attention, language or learning disorders, and visual-perceptual/coordination disorders, are frequently observed in very preterm children (<33 weeks of gestation), also in the context of moderate and late prematurity, and are frequent a cause of disability and referral to the pediatric neurologist.2–4 In these children, executive function (EF) impairment has been recognized as causing school difficulties and failure, even in the absence of overt intellectual deficits.4–6
EF is an “umbrella term” encompassing a range of high-end cognitive processes essential for goal-directed behaviors, that is, working memory, planning, attention shift, inhibition, and persistence. 7 An increasing number of studies have shown that, despite improved neonatal care, preterm children are still at risk of EF impairment. 8 Moreover, these difficulties persist into adolescence and adulthood, potentially undermining the development and social integration of these individuals.9–11 For this reason, there is a growing interest in early interventions in preterm infants to prevent academic failure later in life.11,12 Several studies have investigated the role of new technologies in the rehabilitation of preterm children,13–17 but their specific effects and long-term benefits on academic performance are still debated. 18 Computerized interventions proposed in the literature are targeted on specific domains of EF, such as working memory.
However, they often lack an association with physical activity, and the children are usually engaged in a sitting position. According to recent studies, neuroplasticity in cognitive domains is enhanced when associated with physical activity.19,20 Virtual reality (VR) rehabilitation is increasingly recognized as a useful adjunctive tool in rehabilitations of various neurological conditions, in particular, cerebral palsy 21 and EF deficits in premature born children.13–17 Different VR platforms and exergames, 22 that is, videogames based on motion-sensing technology, have been developed, with the specific aim of coupling physical exercise with rehabilitation-oriented tasks and games. Intendu is an adaptive VR platform interacting with patients via video-monitoring and Kinect technology controlled by body movements focused on training EF (self-initiation, response inhibition, cognitive flexibility, sustained and divided attention, planning, persistence, and working memory).
The aim of the present randomized controlled trial (RCT) was to evaluate the efficacy of the Intendu trainer at ameliorating EF in preterm children.
Patients and Methods
Study design
This randomized, unblinded, parallel arm, controlled trial of the Intendu brain-trainer (Intendu, Herzlia, Israel) adaptive motion-interaction videogame platform was performed at the Vittore Buzzi Children's Hospital (Milan, Italy). The trial was approved by the Milano Area 1 Ethics Committees (Registration No. 2017/ST/077) and was performed in accordance with the Declaration of Helsinki (Fortaleza revision, 2013), and with European and Italian regulations about privacy. Written consent was obtained from the caregiver of participating children.
The trial was registered with Clinical Trials.gov (NCT03639298) and reported following the CONSORT guidelines for nonpharmacological interventions. 23
Participants
Children born at our hospital before 36 + 5 weeks of gestation were eligible for the study. All preterm children born at our hospital undergo a follow-up program, which includes an MRI at 40 weeks of gestational age and serial ophthalmological, pediatric, and neurological examinations, including the administration of neurodevelopmental tests. Children aged 1–3 years are assessed with the Bayley III scale, while older children with WPPSI–III. Inclusion criteria are the following: (1) age between 4 years to 0 month and 6 years to 11 months; (2) residence no further than 20 km from the hospital; and (3) processing speed quotient (PSQ) ≤91 at WPPSI–III. Exclusion criteria are the following: (1) epilepsy; (2) intellectual disability (WPPSI–III full-scale IQ score <70); (3) cerebral palsy (Gross Motor Function Classification System >2); and (4) severe sensory impairment (bilateral deafness and/or blindness). The trial's flow diagram is depicted in Figure 1.
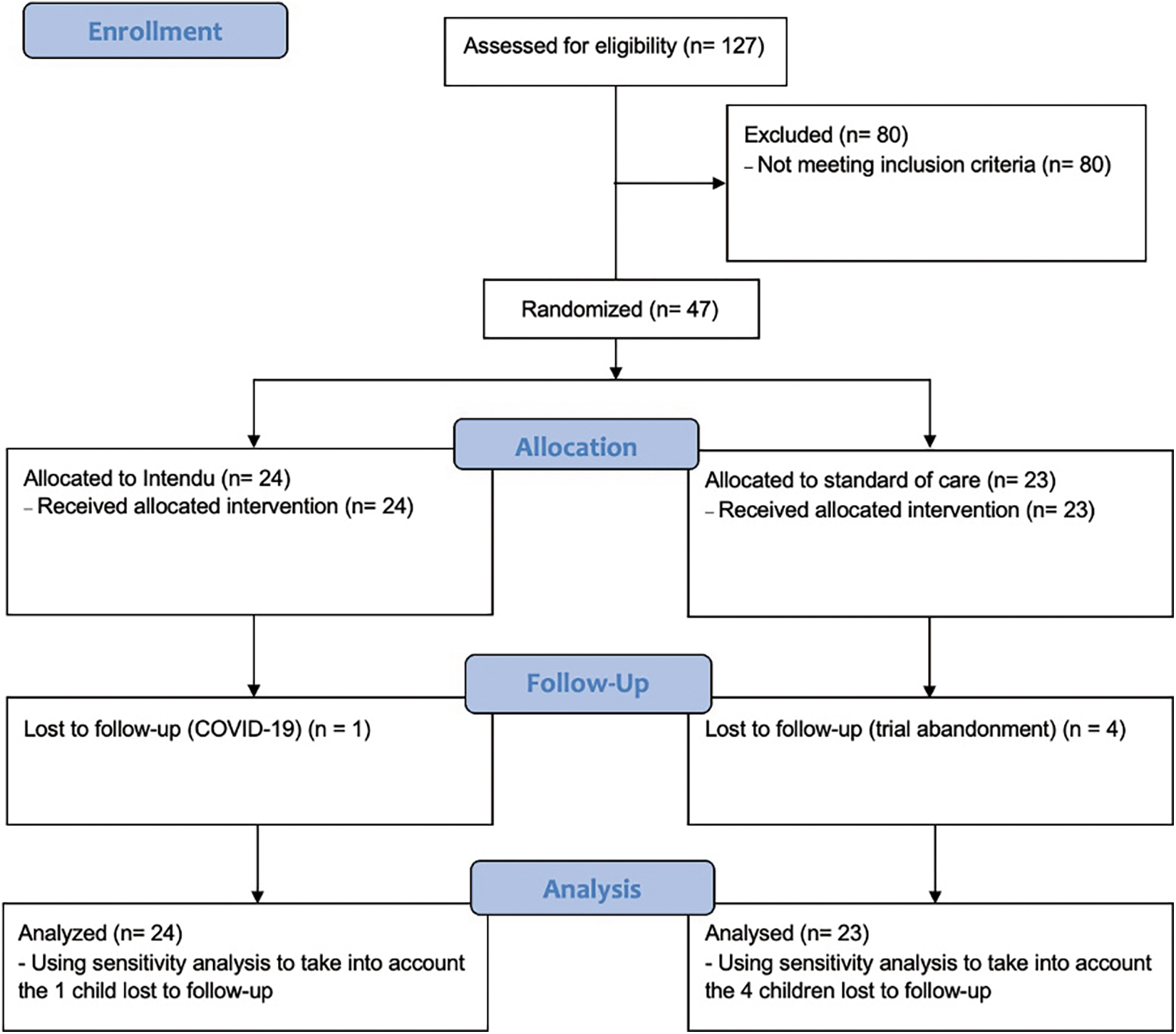
Flow diagram of the trial according to the CONSORT guidelines for nonpharmacological intervention (https://www.equator-network.org/reporting-guidelines/consort/). Color images are available online.
Intervention
The intervention administered to the experimental arm was a training with the Intendu software. The training consisted of 10 sessions, each lasting 20 minutes, 2 or 3 times per week for 4 weeks, and performed under the supervision of an expert psychologist. The number of sessions was decided according to preliminary tests with the Intendu software, in which the children generally reached a good confidence with every game and their score topped after five 20-minute sessions (Fig. 2). Therefore, we opted for five learning sessions followed by five additional sessions of reinforcement. The child stood at 3-meter distance from the 35 inches monitor and from the input device, with her/his avatar appearing on the monitor and moving consistently with him/her. Five Intendu games were selected for the present study corresponding to different real-life scenarios: (1) multitasking-food court, (2) response inhibition-food court, (3) multitasking-bus stop, (4) inhibition category-bus station, and (5) working memory-delivery service.
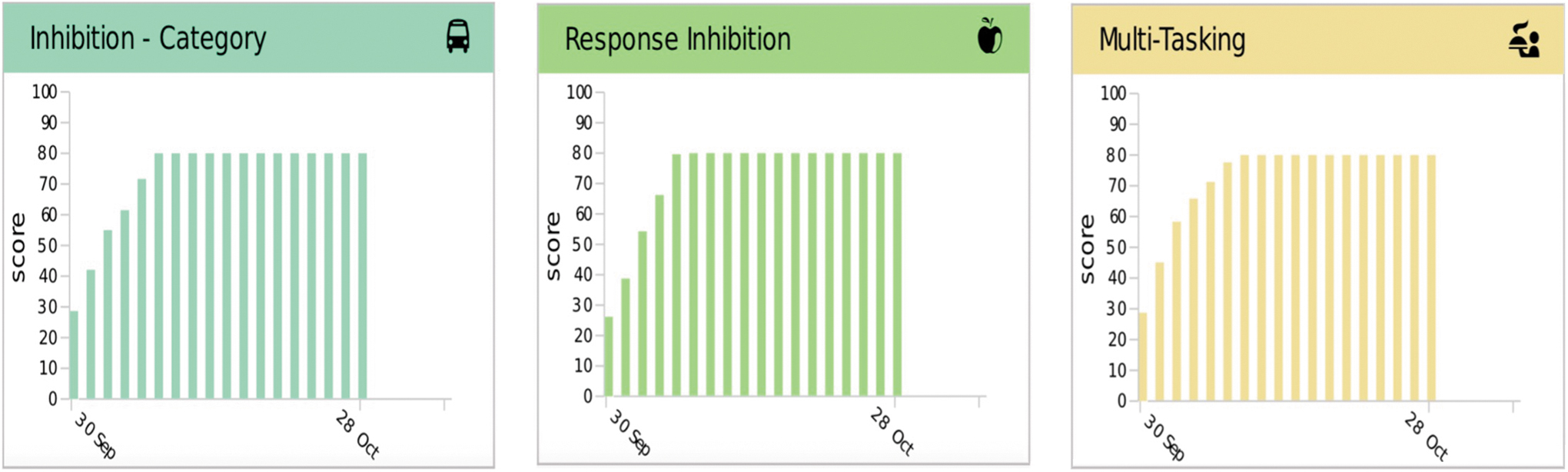
Graphs based on in-game performances generated by the Intendu software. Each bar represents the maximum score achieved by the child after every training session. The children generally reached a good confidence with every game and their score topped generally after five 20-minute sessions. Color images are available online.
In the multitasking food court game, the child is asked to serve as many customers as possible. Two movements are required: moving sideways to face the customer and swiping up to serve food. The game requires planning how to approach simultaneous stimuli. Adaptation parameters are the number of and the duration of intervals between concurrent stimuli, and the type of stimulus (customer's request/rotten food).
In the response inhibition food court game, the child must serve customers. Here, the child is required to give food only to customers wearing a shirt of a given color. Adaptation parameters are the number and duration of intervals between concurrent stimuli and changes of instructions during the game (shirt color determining serving/not serving).
At the multitasking bus stop game, the child must board as many passengers as possible, moving sideways to face the bus and swiping up to open the access gate. Adaptation parameters are the number of and time of intervals between stimuli, and stimulus type (passenger's request to load a specific bus).
At the inhibition-category bus station game, the child must move sideways and get as many passengers as possible on any public transportation vehicle. Here the child must move only specific passengers (in a similar manner to the response inhibition food court game). Adaptation parameters are the number of and time of intervals between concurrent stimuli, stimulus type (public transportation vs. other vehicles).
In the working memory delivery service game, the child must order a list of items and put them in the bag in the correct order. The child must move sideways to face and swipe up to pick up an item. The adaptation parameters consist of the numbers of items (from 2 to 7).
The intervention administered to the control arm was the standard of care at our hospital. The same standard of care was used with the experimental arm, in addition to the Intendu training.
Outcomes
The main outcome was the proportion of children with a 10-point increase in PSQ as measured by WPPSI–III. PSQ is a composite score obtained from two WPPSI–III subtests (coding and symbol search). The mean PSQ score is 100 (standard deviation: 15). The secondary outcomes were the changes in four NEPSY-II subsets (visual attention, statue, memory for designs, block construction). Outcomes were assessed at baseline and 4 weeks thereafter.
Acceptability
The Intendu platform was designed to train adolescents and adults with brain injuries. To date, children have never been trained with this platform. Therefore, we evaluated acceptability using a structured interview of caregivers and children in the experimental arm. The interview included questions regarding motivation, enjoyment, challenges, and adverse effects.
Sample size calculation
Sample size was calculated based on the primary outcome, that is, the proportion of children with a 10-point increase in the PSQ over baseline. We choose the 10-point threshold because a retrospective analysis of PSQ changes in a cohort of 41 premature children at our hospital showed that 10 of them (24%) had a yearly increase of PSQ ≥10 points (unpublished data). We considered the treatment effective if it was able to increase the proportion of children with the main outcome from 24% to 60%. Thirty-five subjects per arm are needed to detect an absolute difference of 36% (60%–24%) at an alpha level of 0.05 with a power of 0.88 (Pearson's chi-square test).
Randomization
Treatment was administered according to a computer-generated randomization list produced using Randomizer (www.randomizer.org). The study coordinator (B.S.) enrolled the children and assigned participants to the randomized group.
Allocation concealment
The treatments were consecutively numbered according to the randomization list, which was known only to the study coordinator.
Blinding
Blinding of the patients and of the outcome assessor (G.C., V.B., B.S.) was not possible because of the nature of intervention.
Statistical analysis
Most continuous variables were not Gaussian-distributed, and all are reported as median (50th percentile) and interquartile range (25th and 75th percentiles). Discrete variables are reported as the number and proportion of subjects with the characteristic of interest. The analysis of the main outcome, that is, the proportion of children with a 10-point increase in PSQ over baseline, was performed using the prespecified Pearson's chi-square (see Sample Size Calculation section). The 95% confidence intervals (CI) of the risk difference between the experimental and control arm were calculated using Newcombe 10 method 24 and those of the number needed to treat (NNT) using Bender's method. 25
A secondary analysis of the main outcome was performed using a random-effect generalized linear model (RE-GLM) using WWPSI–III (continuous, score) as response variable and treatment (discrete: 0 = control; 1 = experimental), time (discrete: 0 = baseline; 1 = 4 weeks), and a treatment × time (discrete × discrete) interaction. 26 Statistical analysis was performed using Stata 17.0 (Stata Corporation, College Station, TX).
Results
The study started in September 2019 and ended prematurely on November 2020 because COVID-19 pandemic rendered it impossible to recruit additional children in a reasonable time. The third inclusion criterion specified by the designed study (i.e., PSQ ≤91 at WPPSI–III) was not fulfilled, so we had to include children with a higher baseline score in the study protocol. A total of 127 children were assessed for eligibility. Eighty children were excluded because they did not meet the inclusion criteria. The remaining 47 children were randomized to the experimental (n = 24) or control arm (n = 23). One child in the experimental arm abandoned the study after randomization due to the COVID-19 pandemic; four children in the control arm were lost to follow-up before the final visit. Complete data were available for 23 children in the experimental and for 19 children in the control arm.
Baseline features
The baseline features of the children are given in Table 1.
Clinical and Demographic Characteristic of the Children
CB, construction blocks; FGR, fetal growth restriction; iqi, interquartile interval; IVH, intraventricular hemorrhage; MD, memory for designs; NEC, necrotizing enterocolitis; PPROM, premature rupture of membranes; PVL, periventricular leukomalacia; RDS, respiratory distress syndrome; ROP, retinopathy of prematurity; ST, statue; TTTS, twin-to-twin transfusion syndrome; VA, visual attention; WM, white matter.
Prespecified analysis of the main outcome
Thirteen of 23 children (56%) reached the main outcome in the experimental group and 5 of 19 (26%) in the control group (P = 0.049, Pearson's chi-square, per-protocol analysis). This corresponds to an absolute benefit increase (ABI) of 30% (Newcombe 10, 95% CI: 0.3%–53%). This suggests that Intendu is effective at training EF in premature children, but the precision of estimate is too wide to reach any definitive conclusion in this regard. The NNT (i.e., 1/ABI) is acceptable but again too wide to reach any definite conclusion (NNT = 3, Bender, 95% CI: 2–321). Refer to Figure 3 for the individual PSQ trajectory in the control group vs. treatment group.
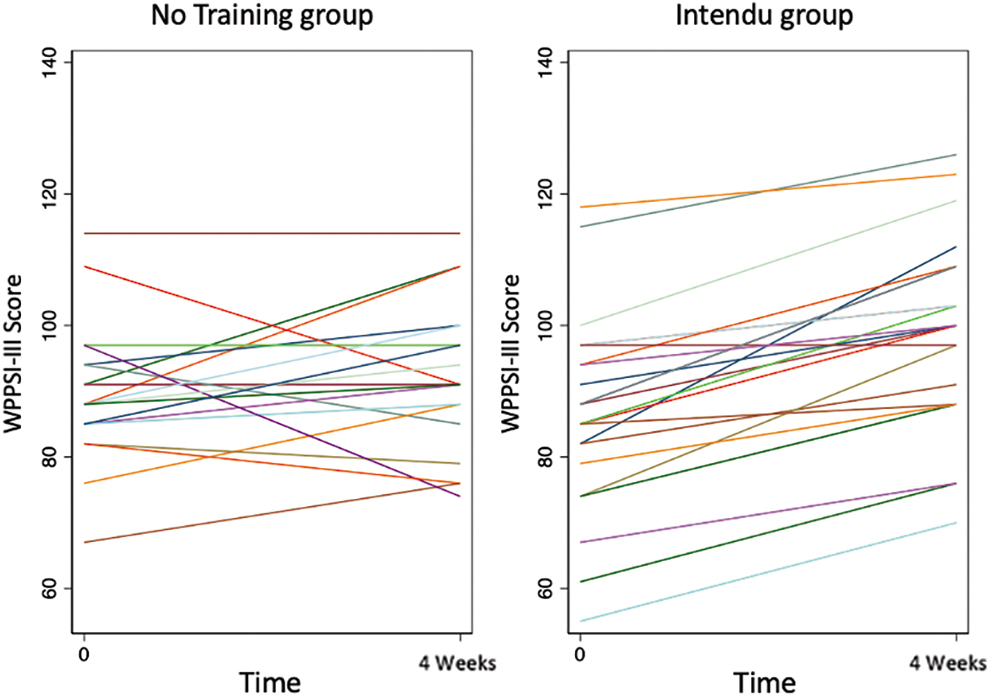
Plot of the individual PSQ trajectories in the experimental and control arms (per-protocol analysis). Prespecified analysis paragraph, see below. PSQ, processing speed quotient. Color images are available online.
Sensitivity analysis of the prespecified main outcome
Under the assumption that the children lost in the experimental (n = 1) and control arm (n = 4) had not experienced the main outcome, 13 of 24 children (54%) reached the main outcome in the experimental group, and 5 of 23 (22%) in the control group (P = 0.022, Pearson's chi-square, intention-to-treat analysis). This corresponds to an ABI of 32% (Newcombe 10, 95% CI: 5%–54%) and to a NNT of 3 (Bender, 95% CI: 2–21).
Secondary analysis of the main outcome
As estimated by RE-GLM, the mean (95% CI) baseline and final values of PSQ were 90 (84–95) and 92 (86–98) in the control group, and 92 (86–98) and 99 (94–105) in the experimental group. This corresponds to an increase of 10 (5–16) units of the PSQ score for the experimental versus the control arm.
Other outcomes
The secondary outcomes, that is, the changes in visual attention, statue, memory for designs, and block construction measured by NEPSY-II could not be evaluated because of the lack of compliance and fatigue of the participants. The test session, including both WPPSI–III and NEPSY-II, took, in fact, more than 90 minutes and most of our children study were unable to sit for that long. Moreover, most of the caregivers were unable to obtain additional leaves of absence from work to perform a second session of testing.
Acceptability
All caregivers and most children appreciated the training and would recommend it to others. However, three children expressed mild complaints: one claimed that the “video game was boring” and two children found the scenario “response inhibition” frightening due to the presence of “thieves.” No adverse effects or other issues were reported.
Discussion
We evaluated the efficacy of the Intendu Brain-trainer at ameliorating EF in preterm children. At per-protocol analysis, we found an ABI of 30% in the experimental versus control group at 4 weeks; however, the precision of such estimate was low (95% CI: 0.3%–53%). These findings were confirmed at intention-to-treat analysis where ABI was similar but more precisely estimated (33%, 95% CI: 6%–55%). This finding adds credibility to the per-protocol analysis performed only on the children available at follow-up. At the secondary analysis, we found an increase of 10 (5–16) units of PSQ for the experimental versus control arm at the end of the study adding to the idea that Intendu may be useful to promote EF in pre-terms. VR and videogames rehabilitation have been proposed as a potentially effective intervention for improving motor function in children with cerebral palsy. 21
Preterm children are at greater risk of developing, not only motor disabilities but also EF impairments, especially at school age.2–4 For this reason, infants are included in long-term follow-up programs, which are implemented to detect abnormal developmental trajectories. According to Miyake et al., 7 three axes constitute the core of EF: inhibition, working memory, and shifting. Other lower grade processes, such as processing speed, can control and regulate more complex EFs. In this regard, preterm children have been found to be slower than full-term controls to solve complex stimuli. It has been proposed a developmental “cascade model”, in which prematurity influences processing speed, which in turn, influences EF, and consequently academic achievements.27–29 It has been described that processing speed plays a pivotal role in preterms' academic failures.27–29
Several studies have focused on computer-based rehabilitation of EF. Aarnoudse-Moens et al. presented a small pilot study to examine the feasibility of a computerized instrument (BrainGame Brian) in a group of children born ≤30 weeks or with a birth weight ≤1000 g with attention problems. The authors found significant changes in visual working memory and speed variability 2 weeks after training. 15 However, a few years later, the same authors reported a double-blind randomized study which included 85 preterm children with attention problems reporting conflicting results. 13 The participants were allocated to three groups: EF training, placebo training, and waitlist condition. The children were also evaluated 5 months after the first follow-up assessment.
The authors concluded that EF training is not effective in improving attention, EF, and academic performance and, even though some beneficial effect was observed, it was not significant. Similar results were reported by Anderson et al. in a RCT investigating the effects of CogMed in very preterm children. 14 This instrument was developed to train working memory in full-term children with ADHD and autism. They found no positive effects of CogMed on attentional functioning, working memory, and academic performance. On the contrary, Di Lieto et al. has found that the CogMed platform in preterm children with diplegia and periventricular leukomalacia can improve not only working memory but also other nontrained skills, such as visuospatial skills, inhibition of automatic responses and phonological processing. 30
The authors suggest that, in this population, the integration of EF training in the rehabilitation schedule could be beneficial. It is well known that EF deficits are inversely proportional to gestational age. EF are also dependent on white matter integrity, which is often compromised in extremely preterm children. 31 Another recent placebo-controlled trial explored the effects of the CogMed program on brain connectivity networks in a group of children born extremely premature. The children exposed to CogMed had no significant change of brain structural connectivity networks compared to the placebo group. 32 Another study by Di Giusto et al. explored the potential effect of VR therapy in children with specific learning disorders. 17 They enrolled 24 children in a 6-week EF training protocol with VR games using a Kinect interface, showing an improvement in several NEPSY-II subscales at the end of the study.
Recent meta-analyses showed that these training programs may yield limited effects because they focus on a single domain.5,8,21 In this regard, rehabilitation guidelines for children at high risk of perinatal damages are now recommending early interventions that include multimodal learning, consisting of active tasks of increasing complexity with observable consequences. 33 Neuroplasticity in cognitive domains is enhanced when associated with physical activity.32,34,35 Children between preschool and preadolescence are probably the best candidate for attaining significant changes in EF. 36 Another metanalysis (Chen et al.) focused on the effect of exergaming intervention on EF training in children aged 4–12 years, including 11 RCT (n = 508), were included. Exergaming was found to be effective on children's cognitive flexibility, inhibitory control, and working memory; however, more rigorous randomized controlled studies are needed to establish their specific effect. 22
Intendu, an application for training functional cognitive skills, has been developed for adults with acquired brain injury. It focuses on training EF combining physical activity in interactive scenarios. Our study is the first application of the Intendu platform on a cohort of premature children. In our population, the training seems to yield a positive result on WPPSI–III PSQ on a significant proportion of patients. VR-based rehabilitation appears to be an effective and engaging strategy for these children. The interactive motion-sensitive approach couples processing skills-focused training with physical activity, potentially boosting the beneficial effect of rehabilitation. The role of computer-based cognitive training still lacks sufficient evidence to demonstrate the generalizability of skills acquired performing specific tasks during rehabilitation. 18
However, this line of research may open interesting perspectives not just for clinicians, that could integrate such instruments in a rehabilitative plan outside the hospital environment, but also for game developers or companies that may introduce in their mainstream products game dynamics able to challenge specific player skills.
Limitations
The trial presents several limitations. First, owing to the COVID-19 pandemic, we had to terminate it before recruiting the planned number of 70 children. Second, of the 47 randomized children, 5 were lost at follow-up, 1 in the experimental group and 4 in the control group, leaving 42 children for the analysis. Results of per-protocol analysis and intention-to-treat analysis, assuming the same negative outcome in children lost to follow-up, were coherent in suggesting a potential benefit of Intendu. Moreover, children were reassessed after a relatively short period of 4 weeks giving rise to a possible learning effect on retesting. In addition, most children born before 37 weeks of gestation are at greater risk of developing attention impairment and attention and PSQ are intimately connected. WPPSI–III as used in our study to measure PSQ may have been contaminated by attention difficulties.
Conclusion
In the first RCT performed on preterms and more generally in children, the Intendu brain-trainer showed promising short-term results on EF. Larger studies with longer periods of follow-up are warranted to better investigate the role of this or similar technology in promoting better EF in preterm children.
Footnotes
Acknowledgments
The authors thank OBM and Fondazione Buzzi for their support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors would like to thank OBM and Fondazione Buzzi for their unconditional support.