
Abstract
Objective:
This study aimed to evaluate the effect of somatosensory interactive games in combination with pulmonary rehabilitation programs (PRPs) on exercise tolerance, balance function, pulmonary function, inflammatory markers, and healthcare utilization in individuals with acute exacerbation of chronic obstructive pulmonary disease over 12 months.
Design:
In a randomized controlled trial, 80 patients were divided into two groups. The control group participated in a lasted 30 minutes daily program composed of postural training for 10 minutes, limb movement for 10 minutes, and breathing exercises for 10 minutes based on regular oxygen therapy and medication. The experimental group received a once-daily, 20-minute somatosensory interactive game session based on the control group. Patients began treatment within 48 hours after admission and lasted for 6 weeks.
Results:
The time × group interactions on 6-minute walk distance (6MWD) and Brief Balance Evaluation Systems Test (Brief-BESTest) between the two groups were significant (P < 0.001). At the postintervention and each time point of follow-up, the 6-minute walk distance (6MWD) and Brief-BESTest of the intervention group were significantly higher than those of the control group (P < 0.05). The effects of time factor on forced expiratory volume in one second and forced vital capacity were statistically significant (P < 0.05). The 6MWD and Brief-BESTest of the intervention group peaked 3 months after the intervention and were higher than the control group within 12 months. C-reactive protein and procalcitonin were similar between the groups before and after intervention (P > 0.05). The readmission rates and mean length of time spent in the hospital were comparable between the groups at 12 months (P > 0.05).
Conclusions:
The addition of somatosensory interactive games based on a PRP was safe and feasible, and this benefit persisted for 12 months, peaked at 3 months after the intervention, and then gradually decreased.
Introduction
Chronic obstructive pulmonary disease (COPD) is a condition characterized by long-lasting respiratory symptoms and restricted airflow, leading to significant rates of sickness, mortality, and disability. 1 In China, COPD prevalence is 8.6% in people aged 20–40 years and can be as high as 13.6% in people older than 40 years. 2
Acute exacerbation is a major event in the pathogenesis of COPD and occurs approximately 0.5–3.5 times per year. 3 The primary reason for hospitalization is typically an enhanced systemic inflammatory response. 4 Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) has been associated with a higher risk for mortality as well as an impairment in exercise capacity, quality of life, and lung functionality, according to clinical data. 1 Patients with AECOPD may also experience varying degrees of decreased balance, which increases their risk of falling. 5 Furthermore, an impaired balance may also facilitate decreased muscle function, mobility, and exercise endurance. 5 Previous studies have shown that the mortality rate of AECOPD patients is approximately 3.6% within 90 days after discharge. However, this percentage can be as high as 31.0% within 2 years. 6 Therefore, to effectively manage the condition and enhance patient outcomes, developing intervention techniques or treatments for patients with AECOPD is crucial.
Pulmonary rehabilitation can enhance dyspnea symptoms, quality of life, exercise capacity, and endurance while promoting continued engagement in rehabilitation after being discharged.7,8 Pulmonary rehabilitation is recommended during AECOPD by the American Thoracic Society/European Respiratory Society and the British Thoracic Society to prevent further deterioration of the patient’s functional status.9,10 Moreover, increasing evidence suggests that prompt pulmonary rehabilitation during an acute exacerbation may be crucial for enhancing patient outcomes. 11 The optimum time for pulmonary rehabilitation intervention in patients with AECOPD is unknown.
Currently, respiratory muscle training, resistance training, endurance training, and other types of exercise are the only options available to AECOPD patients undergoing early pulmonary rehabilitation. Regretfully, many of these exercises have been identified as “boring” and “monotonous,” which frequently leads to decreased adherence and a lack of enthusiasm or desire, confusing any positive effects. 12 Previous studies have shown that recreational sports programs can enhance patients’ interest in exercise and improve initiative and adherence. 13 However, AECOPD patients frequently worry that these types of exercise therapies could worsen the original symptoms of dyspnea, resulting in avoidance of involvement and a fall in their exercise tolerance thresholds. 12
In recent years, somatosensory interactive games (SIGs) have become popular in physical therapy and rehabilitation. 14 One reason for the success of this method is that the treatment is naturally entertaining, causing participating patients to temporarily forget or disregard any fears or concerns they may have about exercise. This ultimately enhances the impact of exercise. SIGs involve the movement of a patient’s arms in various directions to counterbalance the shifting center of gravity in the body. This exertion can improve oxygen intake and usage, increase activity metabolism, and improve motor function. 14 To do this, patients train in a virtual environment where they can see the benefits of their exercises in real-time on a screen, motivating them to continue. SIG is a novel exercise intervention for rehabilitation that has been used with patients with Parkinson’s disease, moderate-to-severe COPD patients, patients with balance difficulties, and individuals with stable COPD. The use of SIG with these individuals has demonstrated that it can enhance daily activity performance, exercise endurance, balance, coordination, and overall quality of life.14–16 SIG showed similar benefits to traditional exercise in improving motor performance, reducing breathing difficulty, and improving quality of life. 17
The primary objective of the present study was to evaluate the impact of SIG on exercise tolerance, balance function, pulmonary function, inflammatory markers, and healthcare utilization in patients diagnosed with AECOPD. These patients were then monitored for 12 months.
Materials and Methods
Ethical approval
This study was approved by Research Ethics Committees of The First Affiliated Hospital of Soochow University, China. The aim of the study was fully explained to the participants, all of whom signed informed consent. This study was registered at chictr.org (ChiCTR1900027831). This study complies with all CONSORT guidelines and provides the necessary data following those guidelines (Supplementary Checklist).
Study design
This single-blind, randomized, controlled clinical trial design was used to develop this prospective, single-center investigation. The patient allocation and study hypothesis were unknown to the research assistants who collected the data. Outcomes were measured at preintervention, postintervention, 1, 3, 6, and 12 months after the 6-week program was concluded.
Study participants
The eligible participants had a primary diagnosis of AECOPD, as determined by the criteria outlined in the Guidelines for Diagnosis and Treatment of Chronic Obstructive Pulmonary Disease (Revised 2021), 18 developed by the Chinese Medical Association. To be included in this study, these AECOPD patients also needed to have been admitted to the respiratory ward at The First Affiliated Hospital of Soochow University between January 2020 and December 2020. Finally, the participants were limited to those who could complete the SIG motion intervention and provide their voluntary consent.
AECOPD patients whose physical condition increased the risk of serious injury during the exercise, such as those on anticoagulation therapy, joint disease, neuromuscular disease, patients with a Glasgow score less than 15 points, a recent fracture (< 6 weeks and/or unstable), pulmonary embolism, severe nerve system diseases (e.g., epilepsy, unstable angina, and myocardial infarction), and those patients that received noninvasive or invasive mechanical ventilation were excluded. Patients who participated in systematic exercise in the past 6 months were excluded. Within 48 hours of hospitalization, eligible participants were randomized into the control and experimental groups. Based on preliminary research, a group of 30 patients was considered suitable for providing proof of the viability and safety of combining SIG treatment with the pulmonary rehabilitation program (PRP).
Sample size
We hypothesized that adding SIG to the PRP intervention could maintain a higher level of exercise endurance in patients compared to the control group. Therefore, 6-minute walk distance (6MWD) was used as the study’s primary endpoint to estimate the sample size. The sample size for this study was determined using data from the pilot experiment. In the repeated analysis of variance, which was appropriate for the proposed approach and the nature of the variables in the study. Furthermore, the G*Power program calculated a 0.4 effect size, 0.01 significance level, and sample size required to achieve 0.8 power. There were a total of 50 participants. Considering a dropout rate of 20%, the aim was to recruit around 60 patients.
Randomization
The current study used purposive sampling. An independent researcher generated a block randomization allocation sequence using the SAS software and placed it in numbered sealed envelopes for randomization. Afterward, the researcher opened the envelopes and communicated to the physiotherapist the assigned group of patients who had consented.
Interventions
The control group participated in a lasted 30 minutes daily program composed of postural training for 10 minutes, limb movement for 10 minutes, and breathing exercises for 10 minutes based on regular oxygen therapy and medication. The experimental group received a once-daily, 20-minute SIG session based on the control group. The research team had developed a complete health education record, which was given to the patients before their discharge. This handbook offers comprehensive details on diseases, self-care, and workout recommendations.
The SIG session started within 48 hours after admission and lasted 6 weeks. Three games (“Kitchen Sharp Knife,” “Swimming Master,” and “Table Tennis Master”) were selected, and one-to-one instruction was implemented to ensure that the patients mastered the exercises correctly. The breakdown of daily 20 minutes session was as follows: The exercise begins with a 3 minutes “Kitchen Sharp Knife” warm-up, continues for 5 minutes with the left hand only, 5 minutes with the right hand only, takes a 3 minutes break, and concludes with a 4 minutes “Swimming Master” exercise. Patients can decide to sit or stand during exercise based on their comfort and overall health. During each session, if patients experienced dyspnea or fatigue, a 15–30 second rest period was encouraged before the patients were asked to continue. The exercise intensity was classified as appropriate by the Borg scale (score: 3–6). Before and after exercise, the participant’s heart rate, blood pressure, respiration, oxygen saturation, and Borg scale score were closely observed. Oxygen was administered if the patient’s oxygen saturation fell below 88%, and exercise resumed after stabilizing oxygen saturation. The exercise was discontinued if the Borg score exceeded 6 or adverse events occurred. Adverse events were defined as blood pressure and heart rate changing> 20% and oxygen saturation decreasing> 10% before and after intervention. 19 Objective signs such as arrhythmia, thoracalgia, cold sweat, and palpitation were considered adverse reactions after exercise intervention in patients with AECOPD. 20 Patients have the option to discontinue their exercise at any point. The intervention group performed the exercise in a separate room within a ward, using curtain walls to ensure privacy. Throughout the patient’s hospital stay, the project team evaluated the patient’s condition daily to ascertain whether the patient could engage in physical activity on that particular day. The collection of these assessment data was supervised and recorded on the daily rehabilitation nursing table (including pre-exercise evaluation, exercise items, completion situation, and postexercise evaluation). At the time of their discharge, all patients had successfully mastered exercise techniques and achieved their fitness objectives. Following the patient’s discharge, their daily exercise metrics were monitored by self-assessed physical condition and Borg score. The patients maintained a home exercise diary to document their improvement and other variables. During the home exercise period, we conducted telephone follow-up weekly and home visits every 2 weeks.
Measurements
A self-designed survey collected the patients’ general demographic and basic disease information. The demographic data comprised gender, age, body mass index (BMI), and residential status. The primary disease data encompassed the disease’s progression, complications, recent acute exacerbations, and GOLD stages. Exercise tolerance was evaluated using the 6MWD test, following the guidelines provided by the ATS. 21
Balance was assessed using the Brief Balance Evaluation Systems Test (Brief-BESTest). In 2012, Padgett et al. (2012) simplified the test and conducted further verification to ensure its reliability and sensitivity. 22 The authors showed that the Brief-BESTest had an excellent ability to distinguish between falling states. The higher the score, the stronger the balance function of the patient.
Pulmonary function was measured by spirometry (according to the ATS/ERS standards 23 ) using a Spirolab III spirometer (MIR, Italy). Forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) were recorded at six time points.
The levels of C-reactive protein (CRP), measured by transmission immunoturbidimetry, and procalcitonin (PCT), determined by chemical fluorescence, were selected to indicate the overall level of inflammation in the patients. The parameters were evaluated first and then again after six weeks from randomization.
Healthcare utilization was assessed as the length of days spent in the hospital, and the readmission ratio of 12 months after the exercise period of the study was completed.
Statistical analysis
After the data were collected, coded, inputted into the computer, and verified, it was analyzed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA). The intention-to-treat analysis was used for all subjects who had been randomized. Baseline measurements between the PRP and SIG groups were compared using a t-test or chi-square test where appropriate. Between-group changes trends in clinical parameters at 6 weeks from randomization and 1, 3, 6, and 12 months after the final exercise session were assessed using the repeated measures analysis of variance. Before data analysis, Maucly’s sphericity test had been conducted. If sphericity is violated, we would use Greenhouse–Geisser to correct it. At each time point, a single-factor analysis of covariance was used to explain the differences in observed indicators between the two groups of subjects. Baseline parameters were used as the covariates to indicate longitudinal changes in physiological outcomes. Differences less than P < 0.05 were considered significant.
Results
From January to December 2020, a total of 142 AECOPD patients were admitted. Of these, 62 patients were ineligible or did not consent to inclusion in the study. The remaining 80 patients were randomized into PRP or SIG + PRP groups (Fig. 1). A final follow-up was scheduled for December 2021. In the SIG + PRP group, 82.5% (33 out of 40) attended at least 70% of the sessions (Fig. 1). In addition, no statistically significant differences in personal characteristics and measures were observed between the groups at baseline (Table 1).

Flow of participants through study.
Characteristics of the Subjects at Baseline
Data are presented as mean ± SD or n (%).
BMI, body mass index; FEV1, forced expiratory volume in one second; FVC, forced vital capacity.
To assess the effect of SIG, the 6MWD, Brief-BESTest, FEV1, and FVC values of the PRP and SIG + PRP groups were compared during the intervention and follow-up (Table 2). These data indicated that the time*group interactions on 6MWD and Brief-BESTest between the two groups were significant (P < 0.001). Further tests were conducted to test the separate effects of within-subject factors (group and time) in the two groups. At the postintervention and each time point of follow-up, the 6MWD and Brief-BESTest of the intervention group were significantly higher than those of the control group (P < 0.05). Both groups had significantly higher 6MWD at the postintervention and during follow-up than preintervention, but this difference disappeared in the control group at 12 months of follow-up, while the benefit in the intervention group continued. Brief-BESTest of the intervention group at postintervention and during follow-up was significantly higher than preintervention, while that of the control group at postintervention and during follow-up was not significantly different compared with preintervention. The effects of time factor on FEV1 and FVC were statistically significant (P < 0.05). Both groups had significantly higher FEV1 at postintervention and during follow-up than preintervention, while there were no significant differences between the two groups in FEV1 at any time point. The intervention group had significantly higher FVC at postintervention and during follow-up than preintervention; however, this difference was not observed in the control group. The trend graphs of the mean values of 6MWD and Brief-BESTest over time are shown in Figures 2 and 3. The 6MWD and Brief-BESTest of the intervention group peaked 3 months after the intervention and were higher than the control group within 12 months. Inflammatory indicators represented by CRP and PCT were similar between the two groups before and after intervention (P > 0.05) (Table 3). The SIG + PRP and the PRP groups demonstrated a 38.7% and 28.1% risk of readmission at 12 months; however, the rates of readmission and the mean length of time spent in hospital at 12 months were similar (P > 0.05) (Table 4).

6MWD mean value trend graph over time. 6MWD, 6-minute walk distance.
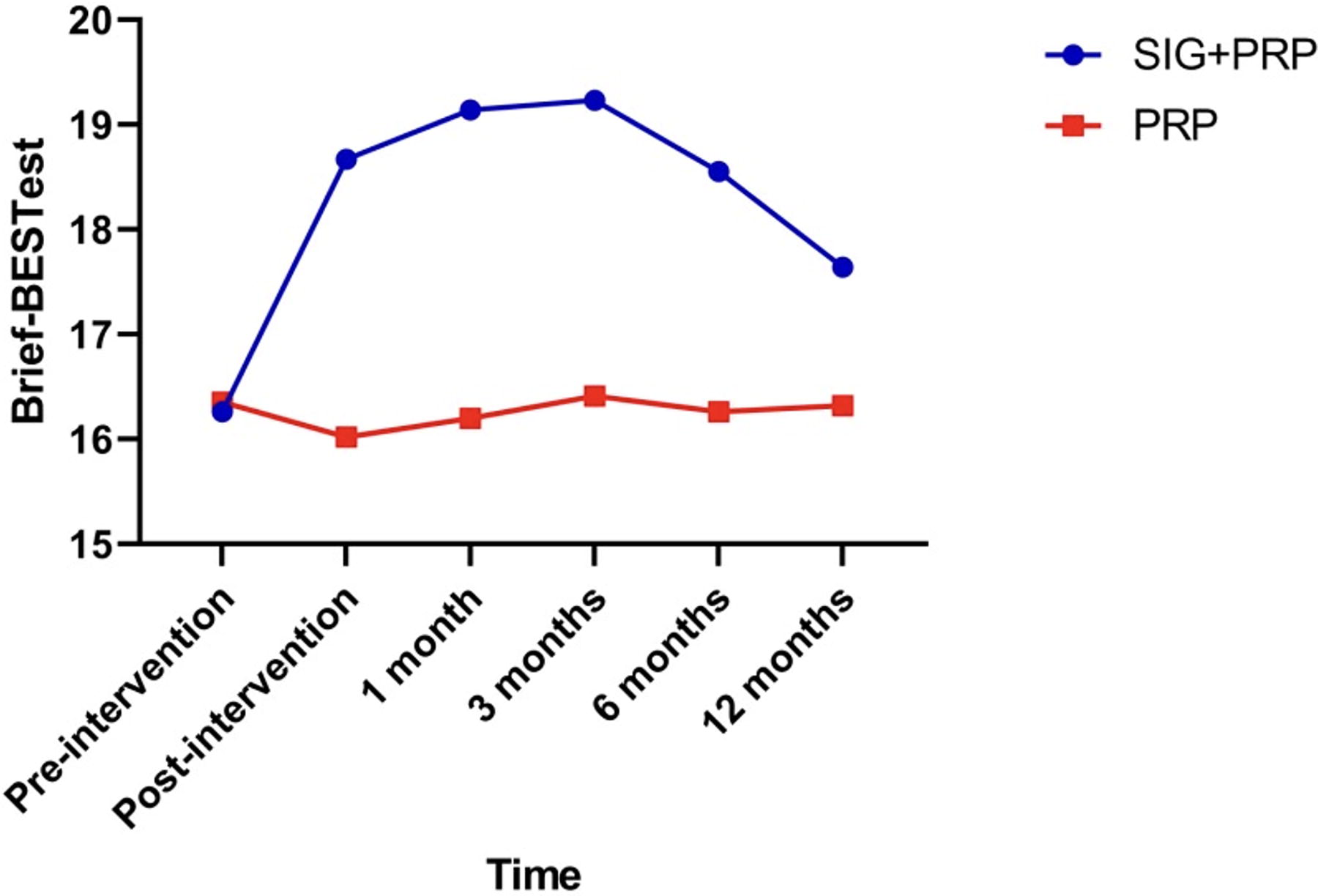
Brief-BESTest mean value trend graph over time. Brief-BESTest, brief balance evaluation systems test.
Results of Assessment and Multivariate Analysis of Variance at Preintervention, Postintervention, 1, 3, 6, and 12 Months
Compared to the Preintervention time point, P < 0.05.
Compared to the Preintervention time point, P < 0.001.
6MWD, 6-minute walk distance; Brief-BESTest, brief balance evaluation systems test; FEV1, forced expiratory volume in one second; FVC, forced vital capacity.
Comparisons of CRP and PCT Between Groups Before and After Intervention
CRP, C-reactive protein; PCT, procalcitonin.
Comparisons of the Healthcare Utilization between Groups at 12 Months
Discussion
This prospective study was an RCT that assessed the role of short-term SIG in combination with PRP therapy on patient outcomes following AECOPD. Current international guidelines recommend a minimum of 6 weeks for a PRP. Based on these recommendations, the present research demonstrates that patients’ 6MWD and Brief-BESTest scores were higher with SIG plus a PRP after 6 weeks than with PRP alone. In addition, in the SIG + PRP group, an improved 6MWD value (56.06 m) exceeded the postulated threshold of minimum clinically significant difference (36–54 m).24,25 It was superior to previously published work conducted by Rutkowski et al. (2020) (39.11 m). 26 The reason for this improvement may be that the intervention cycle in our study is longer than their study (i.e., 6 weeks vs. 2 weeks).
In recent years, attention has been paid to exercise endurance, quality of life, and skeletal muscle function in COPD patients; however, few studies have assessed balance function in the same patients, especially during acute exacerbations. 27 Previous studies have shown that virtual reality rehabilitation can significantly improve the balance function of patients. 26 In agreement with these data, similar improvements were observed in the current study. In addition, the data presented here indicate that the benefits of SIG in combination with PRP are consistent with those of Hill and Mkacher’s traditional balance training.28,29 SIGs have the following characteristics: moderate exercise intensity and full of rhythm. The games can make patients maintain a longer duration of target intensity to ensure the amount of exercise, but they are also very interesting and targeted. The performance feedback after the end can help patients strengthen the treatment results, improve their enthusiasm, and make the training effect persistent. For adults to keep their balance, tactile and proprioceptive information is the most essential input information. Vision primarily controls body balance when these senses are impaired or lost. Patients used the reference objects in the screen to obtain spatial information about themselves and the environment for targeted balance control training. The SIG in this study provided instantaneous visual feedback, which may assist patients in integrating somatosensory and visual information in static and dynamic activities. The SIG provides several realistic virtual scenes and game tasks of different difficulty levels, which enables patients to be guided by specific and clear tasks in training, and then repeatedly perform motor control training with clear goals, and finally integrate the acquired motor skills into functional activities of daily life. The addition of pulmonary rehabilitation-based balance training has yielded significant improvements; however, differences in the intensity, method, and duration of balance intervention among trials have thrown off the agreement. Therefore, more studies are required to develop an optimum, standard intervention practice program. Interestingly, the information presented here suggests that a 6-week intervention can sustain the effects of exercise at a high level for a maximum of three months, a critical time frame for transitioning from acute exacerbation to stabilization. However, the ability of SIG + PRP to delay functional decline in COPD patients’ needs to be explored further in future studies.
Pulmonary function was similar between groups and peaked 1 month after intervention before declining over time. In agreement with this observation, Mazzoleni et al. (2014) 15 showed that patients who underwent seven additional Wii Fit Plus exercise sessions (1 hour daily) in the last week of PRP did not exhibit improved respiratory muscle function.
Before and during each SIG exercise, the patients’ heart rates, blood pressure, respiration, blood oxygen saturation, and Borg scores were recorded in the current study. Consistent with Wardini et al. (2013)
30
and Mazzoleni et al. (2014
The present investigation revealed a lower risk of readmission in both groups compared with a previous study conducted by Ko et al. (2011) in Hong Kong, which had a smaller sample size. 34 However, a key difference is that the control group in our study received the traditional PRP, while the participants in the study by Ko et al. (2011) 34 did not receive any therapy. After 12 months of follow-up, the groups had no significant difference in healthcare utilization. This indicates that a short-term SIG program did not lead to better health outcomes related to COPD compared with the group that received only the PRP. In contrast to the majority of pulmonary rehabilitation research, the patients in this study showed a higher level of disease, comorbidities, more severe airway obstruction, and decreased exercise ability. We acknowledge that the short stay limited the number of closely observed rehabilitation sessions and that most treatments conducted at home rely on telephone follow-up with minimal supervision, which could potentially impact the reported results.
Limitations of the study
The current study had several limitations. First, the intensity of endurance per patient elicited during game training was not measured. Therefore, it is unclear whether the SIG exercises supplied the minimum level of intensity necessary to achieve a beneficial training effect. Furthermore, some participants lacked a saturation monitor equipped with an integrated alarm system, essential for preventing potential oxygen desaturation. This alarm system is a safety measure to evaluate the practicality of at-home testing. At the same time, based on the lack of a convincing degree of patient self-reported attendance, smart wearable devices are expected to be used for remote supervision. Finally, there was no qualitative evaluation of the patient’s emotions and level of satisfaction. Future use of standardized questionnaires could help to accomplish this objective.
Conclusions
In conclusion, this preliminary randomized controlled trial showed that adding SIGs based on a PRP was safe and feasible and that, under the right conditions, SIGs could enhance exercise tolerance and balance function in patients with AECOPD. This benefit persisted for 12 months, peaked at 3 months after the intervention, and gradually decreased.
Footnotes
Authors’ Contributions
(I) Conception and design: X.J.; (II) Administrative support: M.N.; (III) Provision of study materials or patients: M.J., B.Z.; (IV) Collection and assembly of data: X.J., Y.H., B.Z.; (V) Data analysis and interpretation: J.Q., Y.H.; (VI) Article writing: All authors; (VII) Final approval of article: All authors.
Availability of Data and Materials
The data in the current study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
Science and Technology Program of Suzhou (grant number: SKJY2021063).