
Abstract
Background:
Stigma toward people with serious mental illnesses (SMI), like schizophrenia, is a serious global public health challenge that limits the quality of life of those affected and poses a major barrier that keeps people from seeking professional help. There is an urgent need for novel, effective, and scalable interventions to decrease stigmatized perceptions of chronic psychotic disorders and to reduce the health burden imposed by them.
Method:
We conducted a randomized controlled trial to assess the impact of a new immersive virtual reality game (Inclúyete-VR) on the level of stigma toward people with SMI, measured by the Attribution questionnaire (AQ-27). Participants in the experimental group were exposed in an immersive way to hallucinations common in schizophrenia, then shown different psychosocial resources available for their recovery and social inclusion; those in the control group used VR software unrelated to mental health. VR sessions were delivered through Oculus headgear and lasted 25 minutes.
Results:
We randomly assigned 124 university students (55% female) to experimental or control conditions (n = 62 each). We used mixed ANOVA to compare outcomes before and after the intervention between the two groups. We found a significant intervention-by-time interaction (P < 0.001), with a reduction in the experimental group of overall stigma levels on the AQ-27 scale and its three subscales: dangerousness-fear, avoidance, and lack of solidarity (P < 0.001 for all).
Conclusions:
The Inclúyete-VR software proved effective in the short term in reducing stigma toward people with severe mental illness. The program's longer-term efficacy, scalability, and dissemination remain to be studied.
ClinicalTrials.gov Identifier:
NCT05393596.
Introduction
Stigma toward people with serious mental illness (SMI) represents a serious public health problem worldwide and is considered the main barrier for the inclusion and social participation of affected people. 1 Stigma has a negative impact on quality of life and contributes to lower life expectancy as compared with the unaffected population.1,2 As a consequence of prejudice, discriminatory acts, and negative attitudes toward people with SMI, it is common for those affected by them to have lower self-esteem and adherence to treatment, as well as a significant reduction in social network supports.3,4
The compounded effects of stigma pose a major barrier for those with SMI to achieve full social inclusion and interfere with their ability to find and maintain employment, continue or complete studies, achieve technical or professional goals, have adequate housing, and contribute to an increased risk of suicide.5,6 Societal discrimination, prejudice, and stereotypes affect the recovery process, quality of life, and wellbeing of people with SMI and their families. They also represent the main gap toward accessing mental health services for the general population, leading to a delay in diagnosis and lower adherence to specialized treatment.7,8
High levels of stigma are not only present in the general population, but also documented in university students and mental health professionals, which has been explained by the possible influence of limited knowledge about mental illness, along with cultural and media issues.9,10 The latter finding is notable, as it affects the level of quality of care provided, especially toward people with severe and highly stigmatized mental disorders, such as schizophrenia and bipolar disorder.11,12 Innovative and effective interventions among university students to reduce stigmatization of those with SMI have the potential to promote an inclusive and recovery-based mental health approach in future professionals.11,13
Technology-based interventions to reduce stigma
Given the high levels of stigmatization present in society, several initiatives have been carried out worldwide focused on its reduction. Initiatives that provide direct contact with people with SMI are effective interventions, especially when aimed strategically, as to professional and student groups.14,15 Direct social contact and interaction allow participants to share reflections and experiences around mental health, which have proven key to the success of these programs. 16
Adaptation of interactive interventions for implementation in virtual learning spaces is a more recent development, which has been particularly well suited for university students.10,17 Several international programs using technology-based interventions have been implemented, each seeking to reduce SMI-related stigma.17,18 Two recent meta-analyses have shown the efficacy of interventions involving the use of technologies in reducing SMI-related stigma.19,20 Innovative interventions using new technologies include the use of educational videogames21–23 and e-contact with other mental health users.10,18,24,25 These approaches promote skill development and provide tools to promote inclusiveness. 17
The uptake and effectiveness of technology-based approaches can be explained by their degree of interaction in an educational and immersive environment that favors learning and the change of attitudes and beliefs. 26 Indeed, the application of virtual and immersive reality in educational and mental health environments is becoming increasingly frequent. 27 For example, through the creation of 360° interactive virtual spaces, the impact of interventions has been demonstrated at a cognitive and emotional level, which can generate attitudinal and behavioral change through education, the promotion of empathy, and the reduction of explicit and implicit biases. 28 The efficacy of immersive and interactive virtual reality (VR) programs has been demonstrated in different clinical areas of mental health, including anxiety, depression, psychosis, and addictions. 29
Thus, immersive VR incorporates simulated and interactive virtual scenarios in 3D, which allows users to experience and understand in first person different experiences, at the same time that allows interaction with various socioemotional and educational resources, which has proven to be a promising tool to promote the development of empathy and attitude change.28,29 However, still lacking are experimental studies evaluating such programs in reducing stigma toward people with SMI.
In this experimental study we sought to evaluate the effect of an immersive VR program (Inclúyete-VR) on the stigma levels of healthy volunteer university students toward people with SMI. We hypothesized that participants in the experimental group would have significantly lower levels of postintervention standardized stigma scores when compared with participants in the control group.
Methods
Participants
The sample consisted of healthy volunteer students in the Universidad del Desarrollo, Chile. Students were recruited through a nonprobabilistic convenience sampling technique, through direct invitation to participate in the study by the research team in common spaces within the university, such as the library. The inclusion criteria were: (1) age 18 years or older; (2) matriculated as an undergraduate or graduate student; and (3) signing the informed consent form. Using G*Power software, we calculated a minimum sample size of 54 participating students per arm to find the required statistical power, 30 considering a statistical power of 80%, an alpha error of 0.05, and a medium effect size based on previous meta-analyses.19,20
The study was approved by the Ethical Scientific Committee of the Facultad de Medicina—Clínica Alemana Universidad del Desarrollo, Chile (ID 2022-43) and was registered in ClinicalTrials.org before the start of data collection (ID: NCT05393596). Data collection was performed confidentially; only the principal investigator had access to the encrypted and deidentified information. Participants did not receive any direct benefit from being in the research study.
Outcome instruments
Sociodemographic variables
Participants' background characteristics included the variables of age, gender (female, male, and nonbinary), and the university career to which they belonged.
Attribution questionnaire-27
This instrument has been widely used to measure levels of stigma toward people with mental illness in the general population.
31
It presents a vignette of a case of a person diagnosed with schizophrenia, where various stereotypes and prejudices are assessed and measured. For this study, we used the 14-item brief version, adapted and validated into Spanish by Saavedra et al.,
32
who obtained a four-factor structure:
Dangerousness-fear: It assesses the public stigma related to the attribution of dangerousness to people with serious mental illness and the fear and anger caused by them (e.g., “Harry would terrify me”). Lack of solidarity: It includes items related to lack of empathy and lack of help for people with severe mental illness (e.g., “How likely is it that you would help Harry?”). Coercion: It evaluates behaviors toward people with severe mental disorders, such as institutionalization and forced medicalization (e.g., “I think it would be best for Harry's community if he were put away in a psychiatric hospital”). Avoidance (Reverse score): This evaluates flight, escape or avoidance behaviors toward people with severe mental illness (e.g., “ If I were a landlord, I probably would rent an apartment to Harry”).
This instrument uses a 9-point Likert-type response scale, where higher scores represent higher levels of stigma. In the current study sample, the instrument showed adequate reliability (assessed using Cronbach's alpha) in the total score (0.89), and in its four factors (dangerousness-fear = 0.92, lack of solidarity = 0.84, coercion = 0.87, and avoidance = 0.82).
The full version of the Attribution questionnaire (AQ-27) and the abbreviated 14-item version are available as Supplementary Data S1.
VR intervention
Inclúyete-VR
Inclúyete (“Get Involved”) is a VR program designed in Spain to reduce stigma toward people with SMI, through an experiential and educational experience that favors empathy toward people affected by them. For the development of this program, several mental health users and professionals actively collaborated in the design and selection of scenarios and interactions within the software. The complete description of Inclúyete-VR, as well as images of its various levels, are available online at: https://incluyete.blog/incluyete-vr.
The software first provides a brief simulation of common hallucinations in schizophrenia, through which the player is intended to live an experience similar to that of a person suffering from an SMI and the psychological distress that this entails (e.g., feeling of anguish). Next, as shown in Figure 1, players find themselves in a “crisis center,” in which they must advance and overcome six interactive stages, each showing different psychosocial resources available for recovery and social inclusion (such as sports, work, artistic activities, etc.). Inclúyete-VR seeks to place the participant in a virtual world that shows how stigma toward people with SMI is experienced, and also to offer alternatives for rehabilitation and social inclusion, thus giving a less biased view of contemporary mental health treatment.
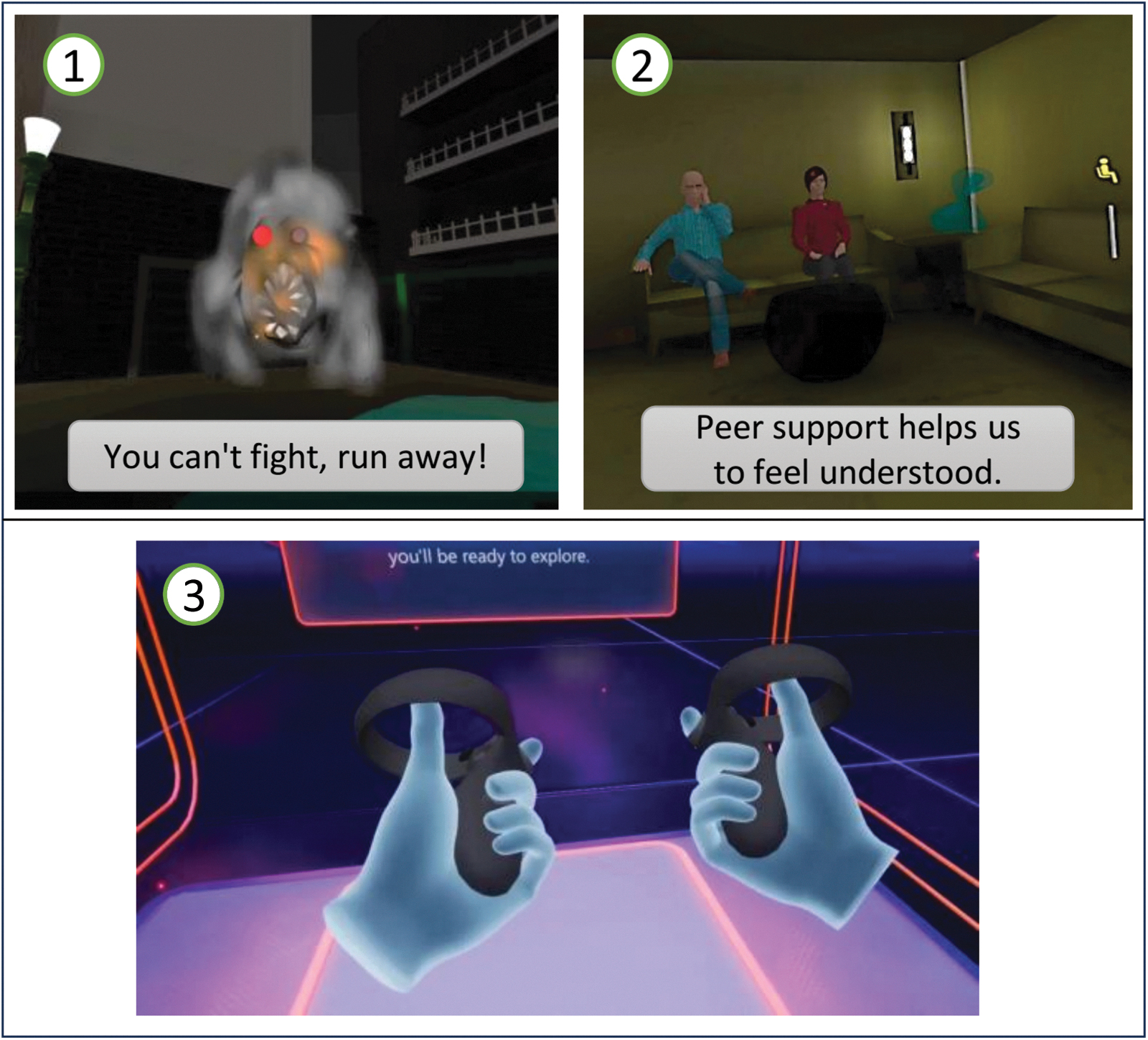
Screenshots of the virtual environment of Inclúyete-VR (1 and 2) and the control group Welcome software (3). (1) Brief simulation of hallucinations: Several monsters approach the player, who can eliminate them by shooting them, but finally a monster appears that cannot be eliminated with the phrase “You can't fight, run away!”; (2) Crisis center: Two people comment to the player that they have also experienced situations similar to his and that they can help him, they also inform the player that there are several rooms where can perform different activities. Then the following sentence is noted “Peer support helps us to feel understood.” (3) Playful interfaces and instructions for Oculus Quest 2®. Color images are available online.
Welcome software (First Step Oculus)
We used this program with participants in the control group. It presents a similarly interactive virtual environment, but one that is not related to mental health, where several playful interfaces and instructions for the Oculus Quest 2® VR headset are presented (Fig. 1).
VR delivery
After signing the informed consent, participants were randomized and assigned in equal parts to the experimental or control conditions, which was performed by the blocked randomization method using the Research Randomizer Software®. The experimental procedure was conducted in the Realitec-UDD laboratory, and the intervention delivered through Oculus Quest 2 VR headsets. The intervention was conducted individually and facilitated by research team staff trained in the use of both software, who provided general instructions and familiarization on the use of the VR controllers and headsets (e.g., basic functions and a general contextualization of each scenario). At the same time, the entire intervention of the virtual scenario was transmitted on a screen of the research team, to follow up and resolve doubts during its application.
In both groups, stigma levels were measured immediately before and after the intervention by accessing the online questionnaire through their smartphones. The procedure lasted between 20 and 30 minutes per participant, with similar duration between the control and experimental groups.
Statistical analyses
We used Student's t-test for independent samples to compare the means of preintervention stigma levels between the control and experimental groups. Next, we used two-way mixed model ANOVA to compare stigma levels across time points (pre- and postintervention) and intervention (Inclúyete-VR vs. control), and to evaluate the interaction effect between time and intervention. We used the Greenhouse–Geisser univariate test 33 to report significance on the main and interaction effects. We used the Bonferroni post hoc adjustment to account for multiple contrasts. We conducted all data analyses using SPSS® version 27.
Results
The study sample consisted of 124 university students from Santiago, Chile, who were between 18 and 35 years of age (M = 21.9, SD = 2.5). There were more female participants (n = 69, 55.6%) than male (n = 54, 43.5%); one participant did not identify within the gender binary. Students belonged to a health care field (e.g., dentistry, medicine, nursing; 29%), to psychology (29%), or to engineering (23%). The rest (19%) pursued careers such as architecture, law, political science, or graphic design, among others.
Regarding these variables, no significant differences were observed between the control and experimental groups with respect to age [t(122) = 0.72, P = 0.472] nor gender [F(1, 122) = 1.51, P = 0.222].
We summarize descriptive statistics for the pre/post stigma measure and its four dimensions of interest in Table 1. Of note, we found no statistically significant differences at baseline in any of the measures between the control and experimental groups.
Baseline and Pre-Post Mean on the 14-Item Attribution Questionnaire
For the total stigma score on the 14-item Attribution Questionnaire, we found a significant main effect of time (F1, 122 = 6.45, P = 0.01, η 2 = 0.05) and group (F1, 122 = 6.15, P = 0.01, η 2 = 0.05). Figure 2a displays the significant time-by-intervention interaction (F1, 122 = 13.29, P < 0.001, η 2 = 0.10). Specifically, mean differences are found between pre- and postintervention in the experimental group (P < 0.001), but not in the control group (P = 0.436).
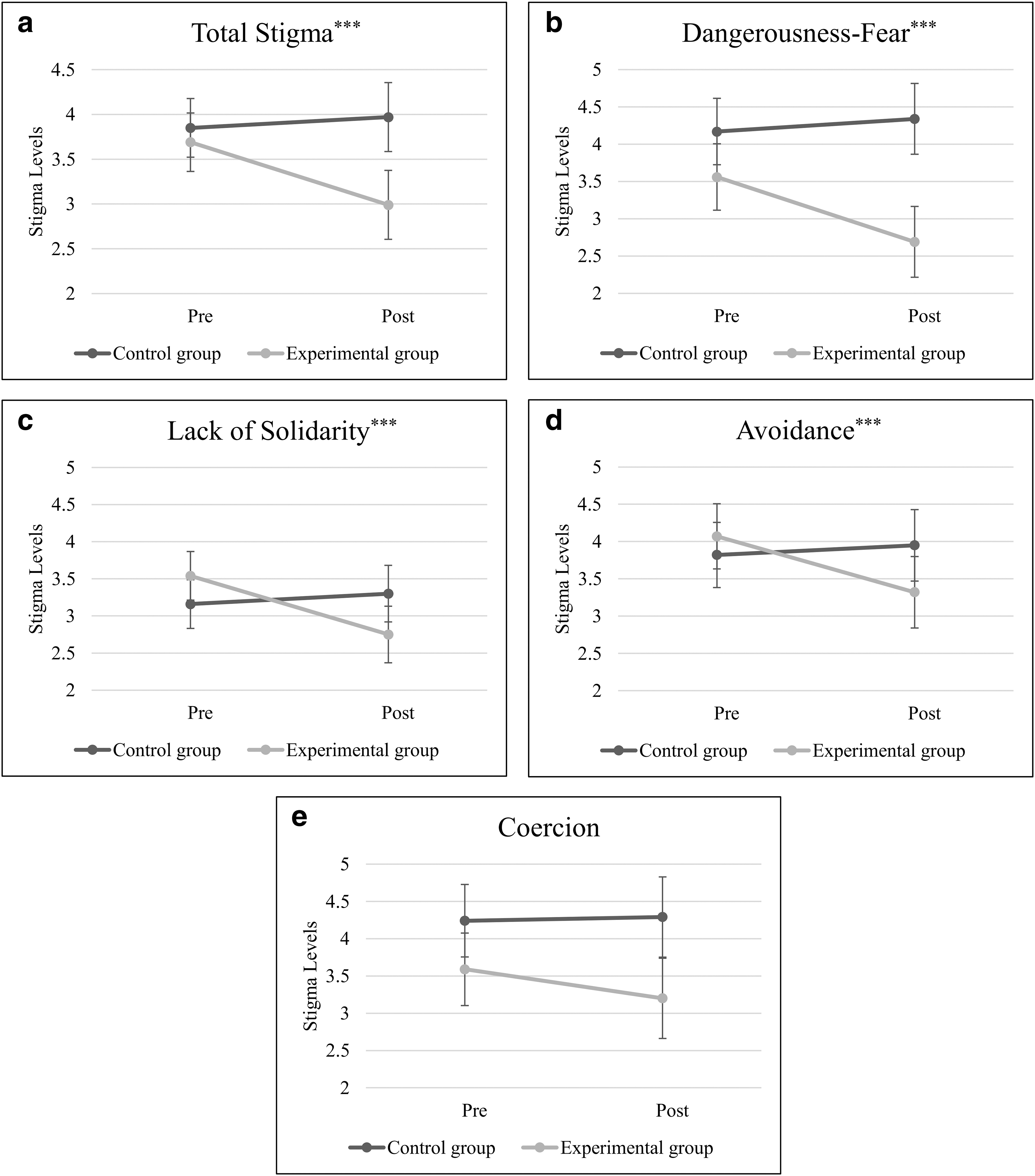
Attributions Questionnaire: marginal means across time and intervention.
The time-by-intervention interaction was significant across three of the Questionnaire's four component dimensions:
(1) Dangerousness-fear (main effect of time: F1, 122 = 8.51, P < 0.01, η 2 = 0.07 and group (F1, 122 = 13.69, P < 0.001, η 2 = 0.10), time-by-intervention interaction: F1, 122 = 18.56, P < 0.001, η 2 = 0.13, Fig. 2b), where mean differences are found between pre- and postintervention in the experimental group (P < 0.001), but not in the control group (P = 0.327); (2) Lack of solidarity (main effect of time: F1, 122 = 8.03, P < 0.01, η 2 = 0.06 and group F1, 122 = 0.13, P = 0.723, η 2 = 0.001, time-by-intervention interaction: F1, 122 = 16.89, P < 0.001, η 2 = 0.12, Fig. 2c), where mean differences are found between pre- and postintervention in the experimental group (P < 0.001), but not in the control group (P = 0.369); and 3) Avoidance (main effect of time: F1, 122 = 5.33, P = 0.02, η 2 = 0.04 and group F1, 122 = 0.42, P = 0.52, η 2 = 0.05, time-by-intervention interaction: F1, 122 = 11.30, P = 0.001, η 2 = 0.09, Fig. 2d), where mean differences are found between pre- and postintervention in the experimental group (P < 0.001), but not in the control group (P = 0.458).
By contrast, we found no statistically significant differences in the time-by-intervention interaction of Coercion dimension [F(1, 122) = 2.14, P = 0.15, η 2 = 0.02] nor main effect of time [F(1, 122) = 1.30, P = 0.26, η 2 = 0.01], but we found a main effect of group: [F(1, 122) = 6.64, P = 0.01, η 2 = 0.05; Fig. 2e].
Discussion
This study provides preliminary support for the Inclúyete-VR software as a useful tool to reduce stigma among university students toward people with SMI. Our findings are consistent with a growing international evidence base for the clinical use of new electronic technologies, ranging from videogames to online escape rooms.21,23 Indeed, the integration of an educational component in an immersive VR environment can promote change at the cognitive and emotional levels.17,34,35
Regarding the baseline levels of stigma assessed with the AQ-27 instrument in the present study (M = 3.77), these were slightly higher than in studies conducted in university populations in Chile 25 (M = 3.69) and Spain 23 (M = 3.54).
Previous meta-analysis has noted that simulation of auditory hallucination can increase stigma levels.20,36 Specifically, two studies37,38 that applied a 16-minute hallucination simulation showed that these interventions increased social distance, coercive attitudes, and negative emotions, along with a decreased willingness to help and interact with people with mental health problems. This may be explained by the lack of an educational component and adequate contextualization to the participants of these interventions; however, more studies are still needed to determine a dose–response relationship of the time of exposure to hallucinations that does not generate an increase in stigma. Within the Inclúyete-VR software, hallucinations are incorporated only briefly at the beginning, followed by educational and psychosocial components that are integrated to allow players to empathize, understand, and generate change in their stigmatized attitudes, beliefs, and behaviors. This represents a fundamental innovation in this field, as it incorporates the recommendations by several authors in relation to the use of simulation of hallucination symptoms, integrated instead with educational elements so as to not reify itemized and discriminatory views.39,40
Despite our positive results, the dimension of coercion did not change significantly with the intervention. The coercion factor, is understood as the belief and acceptance of forced measures toward people with mental health problems (e.g., forcing people to participate in the administration of medicines and treatments), especially when these are focused on people with SMI and psychotic symptoms. 41 Thus, the lack of effect on coercion in our study can be explained by the fact that this is a complex component to modify as it interacts at different cognitive, emotional, and cultural levels, associated with the lack of availability and knowledge of alternative treatment and noncoercive measures in mental health care. 41 Additionally, although the hallucination component was brief in the Inclúyete-VR software, previous studies37,38 have shown that the use of simulation with hallucinations has an effect of increasing stigma levels, especially coercive attitudes to force treatment in people with mental illness, so this component potentially could have interacted with the intervention and explained the lack of significant change in levels of coercion in our study.
New technologies constitute a dynamic novel resource for social change. As an alternative tool, they can complement efforts at stigma reduction around people with mental health problems. Since this area is of recent development in psychology and mental health, its implementation presents challenges for adaptation, dissemination, and scalability especially considering the cost in the development and application of virtual immersive software. Future adaptations of the software will benefit from incorporating participatory components of communities of users and key players and stakeholders in its implementation, including students and experts with experience in mental health, efforts that have proven critical to the success and sustainability of antistigma programs.15,42
We were deliberate in our choice of students as study participants, given the relevance and need for implementation at early stages of professional development, as well as in educational and community contexts that favor dissemination among the general population and university students.10,15,17 VR, game-based interventions represent an opportunity for the future integration of similar programs into university curricula at the national and international levels.
We recognize several limitations. First, our sample was relatively small and derived from a single educational institution, limiting generalizability to other populations. Replication through multicenter collaborative efforts could be the next step. Second, we did not collect follow-up measurements on stigma levels; future studies should assess sustainability of the effects of the VR program. Third, in our study only one stigma measurement instrument was used, and because stigma is a complex construct, future research should assess the effect on other cognitive, emotional, and behavioral components of the construct (e.g., by measuring implicit stigma). Fourth, our study did not include within the design and analysis mediating variables of the mechanisms of interaction, perception, and behavior in the VR environment that can affect and explain the effects of the intervention, such as the degree of immersion and sense of presence 43 nor the sequence and time of interaction with the virtual environments, 44 so future studies should include these variables. Finally, we did not account for the specific characteristics of the participants.
Factors that could influence results, such as sociocultural origin, level of knowledge of mental health, or the presence of personal or family mental health problems, are aspects that need to be incorporated in future research.
Despite these limitations, the Inclúyete-VR software proved to be effective in the short term in reducing stigma toward people with mental health problems. Future research on intervention that incorporate VR in an immersive way should address long-term efficacy and scalability, as well as design and implementation enhancements of new versions that incorporate technological advances in this area.
Footnotes
Acknowledgments
The authors would like to thank the RealiTec team, Universidad del Desarrollo, Chile, for their support in conducting the study and providing the technological tools for its application. This publication is part of the Project UAL202-SEJ-Di912 financed by FEDER “A way to make Europe.”
Authors' Contributions
M.E.R.-R.: Conceptualization, Methodology, Formal analysis, Investigation, Resources, Data Curation, Project administration, Supervision, Visualization, and Writing—Original Draft. A.J.C.: Conceptualization, Methodology, Software, and Writing—Original Draft. A.M.: Conceptualization, Methodology, and Writing—Review and Editing. J.R.: Formal analysis and Visualization. J.C.P.: Validation, Formal analysis, and Visualization. S.V.: Validation and Writing—Review and Editing. L.C.: Writing—Review and Editing. J.O.: Investigation and Resources. B.H.: Investigation and Resources. F.C.: Software and Validation; P.C.: Validation. P.C.: Conceptualization and Writing—Review and Editing.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.