
Abstract
Introduction:
Playing together increases social connectedness, and it may be a tool to reduce loneliness. Research into the mental health benefits of board games is underdeveloped.
Objectives:
The study aims to examine the effects of the Kioku board game on well-being outcomes. The Kioku board game was developed in order to enable small group interactions with a focus on encouraging participants to create stories through mutual attention and interaction. We hypothesized that following a weekly intervention for 12 weeks, players would report a decrease in loneliness and an increase in well-being, compared with nonplayers.
Methods:
During the summer of 2022, participants in groups of 4–5 players, chose a cube word and narrated a story. A sample of 151 older adults (Mean age = 75.05 ± 6.46 years) recruited from seven community activity centers in Israel was assigned by block randomization to an intervention (n = 72) or a control group (n = 79), awaiting 4–6 weeks for future participation. Loneliness (UCLA loneliness scale) and well-being (World Health Organization 5-item scale) were evaluated at baseline and at 12 weeks.
Results:
A two-way repeated measures analysis of covariance (ANCOVA) (Group × Time) controlling for age, country of origin, and marital status revealed significant interaction effects for loneliness [F(1, 146) = 178.04, n2 = 0.549, P < 0.001] and well-being [F(1, 146) = 69.14, n2 = 0.321, P < 0.001]. Loneliness decreased in the intervention group (mean difference: 0.62 points, P < 0.001), and increased in the control group (mean difference: 0.18 points, P = 0.001). Well-being increased in the intervention group (mean difference: 0.79 points, P < 0.001) and decreased in the control group (mean difference: 0.20 points, P < 0.001).
Conclusions:
Our findings support the effectiveness of the Kioku board game intervention for decreasing loneliness and promoting well-being in older adults, who might still be coping with the effects of the COVID-19 pandemic.
Introduction
Loneliness is associated with reduced quality of life, decreased well-being, increased morbidity, suicidality, and mortality.1–3 Loneliness is commonly defined as “a distressing discrepancy between desired and actual levels of social contact” and affects people of all ages. 4
In the United States, an annual mortality of 162,000 Americans is reported to be due to social isolation, exceeding the number of deaths from cancer or stroke. The COVID-19 pandemic has caused an increase in the number of socially isolated older adults not only in nursing homes but also in the community, and currently, it is estimated that about a quarter of community-dwelling older adults in the United States suffer from social isolation. Moreover, the economic toll of loneliness on the UK business economy was estimated at around $3 billion annually, and these profound facts have led the UK government to establish a Ministry of Loneliness. Studies have shown that social capital and loneliness have profound effects on older adults’ well-being. Social capital has been found to be positively related to well-being,5,6 while negative connections were found between loneliness and well-being.2,7 Three conceptual pathways connecting loneliness and well-being have been suggested. The first is social exchanges on a day-to-day basis, which elicit emotional reactions and reduction in stress. The second is social networks, which stimulate or restrict the individual’s behavioral repertoire. The third is the mental representations that older adults have about how social ties can satisfy their social needs. 8 We suggested that such pathways correspond well with board games, which may instigate social exchanges on a day-to-day basis, develop the individual’s behavioral repertoire, and create such mental representations.
Recent research emphasizes loneliness as a public health hazard because of its association with a wide range of conditions, including hypertension, cardiovascular disease, cerebrovascular disease Alzheimer’s disease, depression, and insomnia.1,9 The association between loneliness and poor health is unclear—which factor comes first, how loneliness and poor health interact, and whether unknown confounding variables also play a role.4,10 A recent systematic review across 113 countries reported loneliness prevalence among older adults in the range of 6.5% to 24.2%. 5
These alarming reports led to a growing body of research into interventions to reduce social isolation and loneliness, with thousands of publications in the last decade, including board games.11,12 A recent scoping review of three electronic databases (CINAHL, Embase, and Medline) identified a total of 33 reviews evaluating a range of interventions targeted at older people residing in the community or institutionalized settings. The authors concluded that, although many interventions have been developed to combat loneliness and social isolation among older people, the individuality of the experience of loneliness may cause difficulty in the delivery of standardized interventions. 11 An important example of the complexity of the field is the failure of befriending interventions to reach significance in reducing loneliness, despite its enthusiastic adoption by the voluntary sector, with over 3500 schemes existing in United Kingdom alone. 13
More than 40 years ago, the discussion-stimulating board game called “Angels and Devils” was used in nursing homes to try and reduce social isolation among residents. Findings were interpreted as indicating the need for more research in the application of board games to ameliorate negative effects emerging in institutional environments. 14 Over the years, focus on the impact of board games on loneliness in older adults was sparsely studied with a growing focus on video games and digital applications. 15 However, several recent publications support rekindling interest in board games. The Chinese Longitudinal Healthy Longevity Survey CLHLS, conducted in 2005, 2008, and 2011, showed that respondents who frequently played cards or Mah-Jong at baseline were less likely to feel persistent loneliness at follow-up. 16 Similar findings were reported for a different set of games among Portuguese older adults, as well as for four themes of life, “thanks, sorry, love, and farewell,” board game to decrease loneliness in Taiwan.17,18
The Kioku board game was developed to enable small group interactions with a focus on encouraging participants to create stories through mutual attention and interaction. 19 The aim of this study was to examine the effects of the Kioku board game on well-being outcomes. We hypothesized that following a weekly intervention for 12 weeks, players would report a decrease in loneliness and an increase in well-being, compared with nonplayers.
Methods
Participants
Participants were recruited from seven community activity centers by the Department of Senior Citizens in Pardes Hanna, Israel. Inclusion criteria for the study were age 61 years of age or older, reporting no significant cognitive decline, as assessed by research assistant in a short interview, and proficiency in Hebrew.
All participants were given a detailed description of the study beforehand, and after providing written informed consent. We used Block random assignment for participation or waiting-list arms. Eighteen participants (11.9%) did not complete the required procedures before the start of the study intervention; 11 participants from the intervention group and 7 from the control group. Since the attrition rate was minor, no statistical comparison was required. The analyzed sample thus consisted of 151 participants: intervention group (n = 72) and control group (n = 79). Participants in the control group engaged in continuous regular activities at the same-day centers in which the intervention took place. Group differences and descriptive statistics are presented in Table 1.
Means, Standard Deviations, and Group Differences for the Study Sociodemographic Variables
Statistically significant differences are marked in bold.
n = 151.
1, no formal education, 2, elementary education, 3, partial high-school level, 4, high-school education, 5, partial academic education, 6, BA degree.
Intervention
The Kioku board game is a kit with 105 words, each printed on one small wooden block. A group of 3–6 people sit around a table, participants take turns picking a block word in a random manner, then reveal the printed word and use it in a way that provides semantic meaning to the word, by placing it sequentially after the word of the previous player. Thus, by using these block words, the group members become engaged in a collaborative story-building effort. In other words, the group creates new narratives, in the form of a novel and unique story without a predetermined planned direction, so that when associating his or her word block to the story that is being formed, each participant is free to advance the story’s plot in his or her desired “direction.” After the creation of the story, the group is asked to participate in retrieval memory games, in which they use their invented story as the anchor for their retrieval. Players are encouraged to help one another, if necessary, through verbal and nonverbal clues. This methodology of the game makes Kioku a scoreless game and as such not competitive.
Kioku is a storytelling board game that enhances social connections and cognitive engagement, with a focus on enriching the lives of elderly participants. The gameplay unfolds in three stages: Stage 1, free associations: a pivotal in fostering personal connections and setting the stage for collective creativity. As players draw blocks/words at random, they are prompted to share the first thoughts or memories that come to mind. This act of sharing spontaneous associations not only breaks the ice but also creates an intimate atmosphere. This process is instrumental in building trust and camaraderie among players, laying the groundwork for the collaborative storytelling to follow. In stage 2, narrative construction and play come into being: Participants construct a narrative by sequentially adding to the story using the word they have picked in the previous stage. For instance, a player who selects “whale” could contribute: “and suddenly, the sky was filled with clouds shaped like whales,” provided it flows with the narrative thread. The trained peer coach ensures the continuity of the narrative progression.
The number of words contributed is tailored to the group’s cognitive level and familiarity with Kioku, with each player, including the peer coach, contributing at least one word. The peer coach has the discretion to determine the number of stories that will be created and the number of words each will contain. With a noncompetitive spirit, players engage in memory games that challenge them to recall and reconstruct the story. Through collaborative cues, whether verbal or nonverbal, participants work together to piece the narrative back together, reinforcing memory and cooperative problem-solving. Finally, stage 3 represents reflective closure: The game concludes with players sharing personal reflections, facilitated by the peer coach. This encourages a collective debriefing and deepens the social experience.
For this study, 15 volunteers from the seven community activity centers were trained as Kioku facilitators. Each facilitator was assigned a group of 4–5 players. The intervention was conducted in 16 groups in three cities in Israel and took place in community and day centers on a weekly basis for 12 consecutive weeks. It included a between-session weekly contact with the facilitators who further engaged the group with riddles around the group story, through text and pictures, and were sent to the group’s WhatsApp messenger.
Measurements
Participants provided sociodemographic data concerning their age, gender, country of birth, marital status 1 (not married) or 2 (married or cohabitating), education on a scale ranging from 1 (elementary school) to 7 (MA education and above), self-rated health and economic status (not good at all/not so good/pretty good/good/very good), and level of religiosity (secular, traditional, religious, ultra-orthodox, and other).
In this study, loneliness and well-being were the primary and secondary outcomes, respectively. We used the revised shortened 8-item version of the UCLA Loneliness scale to quantify loneliness and the World Health Organization 5-item (WHO-5) well-being scale to quantify well-being.
UCLA Loneliness scale
The UCLA Loneliness scale, containing 20 items, is one of the most commonly used loneliness scales. Due to the length of the questionnaire, its administration is not always practical. Short versions vary in items and were developed with classical test theory and using factor analysis. Loneliness was assessed by the ULS Loneliness Scale-8-item version. 20 The ULS Loneliness Scale-8 items (ULS −8) is a shortened version with 8 items, which was shown to preserve the original psychometric properties of the UCLA-20 items scale. 20 The ULS-8 meets the criteria of unidimensionality and local independence without differential item functioning due to age or sex, and is specifically centering on older adults. 21 The ULS−8 scale measures the frequency by which people usually feel the feelings that are described by each of its items (“How often do you feel each of the following?”). The scale includes items such as “I feel I do not have enough friends,” and “I feel isolated from others,” with two reversed items. Each item is rated on a 4-point scale from 0 = never to 3 = often, with a higher score indicating greater frequency of feeling loneliness, and a mean score is calculated for the eight items. In this study, this measure was used twice, and its internal reliability ranged between 0.76 and 0.77.
WHO-5 well-being scale
The WHO 5-item Well-Being scale (WHO-5) is a short screening instrument for use in the general population. WHO-5 demonstrates good internal and external validity in older adults. 22 In addition, the WHO-5 has been used to quantify self-reported mental well-being in a large comparative survey across 15 countries and regions in Europe. 23
WHO-5 captures emotional well-being as a unidimensional measure, based on five positively worded items such as “My daily life has been filled with things that interest me.” Respondents rate the degree to which these positive items were present in the last 2 weeks on a 6-point Likert scale ranging from 0 = never to 5 = all the time. A questionnaire score is computed by the sum of its items, and ranges from 0 = worst estimated well-being to 25 = best estimated well-being. The scale has adequate validity as an outcome measure in clinical trials and has been applied successfully across a wide range of study fields. 24 In this study, this measure was used twice, and its internal reliability ranged between 0.87 and 0.86.
Statistical analysis
A power analysis for detecting a medium effect size (0.15) with two groups and two measurements required a sample size of 148 participants.
Analyses were conducted by the SPSS 27 software. First, baseline group differences were examined using Chi-square tests for categorical variables and t-tests for continuous variables (Table 1). Since the groups differed in age, country of origin, and marital status, the hypotheses were then examined by two repeated measures analysis of covariance (ANCOVA of Group × Time) controlling for these variables, with loneliness and well-being as the dependent variables. It should be noted that the results of the WHO-5 remained unchanged when we examined the hypotheses with repeated-measures ANOVAs as well. Finally, we conducted simple main effect tests (paired t-tests for each group) to break significant interactions and compare between before and after means of the outcome variables of each of the two groups and ANCOVAs to compare between the two groups at baseline (Time1) and at the end of the intervention (Time2).
Ethics
The study received ethical approval (No. 08–22) by the IRB of University of the first author, Bar-Ilan University, Israel.
Results
Data were collected from a sample of 151 community-dwelling older adults (age range = 61–96, Mean age = 75.05 ± 6.46 years). Sample size calculation indicated that this sample was sufficiently large for the study model. The participants were mostly women (88.7%), about half (55.6%) were born in Israel, and all were living in Israel for an average of 62.5 years (SD = 11.7, range = 28–74). More than half were married (55.0%), and 72.0% defined their religiosity as secular. The participants reported having an academic (45.7%) or high-school education (40.4%). Participants reported good (47.9%) or very good (19.7%) health, and good (51.0%) or very good (17.2%) economic status.
Two two-way (Group × Time) repeated-measures ANCOVAs were conducted, because the intervention and the control groups differed in age, marital status, and country of birth. In line with the two hypotheses, the analyses revealed significant interaction effects for loneliness, F(1, 146) = 178.04, P < 0.001, n2 = 0.549 and well-being, F(1, 146) = 61.06, P < 0.001, n2 = 0.295.
Simple main effects analyses demonstrated that loneliness decreased in the intervention group [mean differences of 0.62 points, M = 2.24, SD = 0.48 in T1; M = 1.62, SD = 0.39 in T2; t(71) = 13.59, P < 0.001, Cohen’s d = 1.60], and increased in the control group [mean differences of 0.18 points, M = 1.92, SD = 0.58 in T1; M = 2.10, SD = 0.56 in T2; t(78) = −5.36 P < 0.001, Cohen’s d = −0.60]. Well-being increased in the intervention group [mean differences of 4.03 points, M = 18.60, SD = 3.63 in T1; M = 22.63, SD = 4.10 in T2; t(71) = −8.81, P < 0.001, Cohen’s d =−1.04, P < 0.001] and deceased in the control group [mean differences of 0.79 points, P < 0.001, M = 20.28, SD = 5.16 in T1; M = 19.49, SD = 4.98 in T2; t(78) = 3.38, P = 0.001, Cohen’s d = 0.29].
When examining the differences in loneliness between the two groups at baseline and after the intervention, significant differences were found in loneliness between the two groups in both measurements. More specifically, the control group reported lower loneliness at the first (baseline) measurement (M = 1.92, SD = 0.58) than the intervention group (M = 2.24, SD = 0.48). A one-way analysis of covariance comparing the two groups on loneliness at baseline was significant, F(1, 146) = 7.72, P < 01, n2 = 0.050. In similar, a one-way analysis of covariance comparing the two groups on loneliness at time 2 (after the intervention) resulted in significant results, F(1, 146) = 43.01, P < 0.001, n2 = 0.228. After the intervention, the intervention group reported lower loneliness at baseline (M = 1.62, SD = 0.39) compared with the control group (M = 2.10, SD = 0.56).
In addition, when examining the differences in well-being between the two groups at baseline and after the intervention, significant differences were found in well-being between the two groups only after the intervention. More specifically, although the control group reported higher well-being at the first (baseline) measurement (M = 20.28, SD = 5.16) than the intervention group (M = 19.00, SD = 3.63), a one-way analysis of covariance comparing the two groups on well-being at baseline was insignificant, F(1, 146) = 1.57, P = 0.213, n2 = 0.011. Nevertheless, when a one-way analysis of covariance comparing the two groups on well-being at time 2 (after the intervention) was conducted, it resulted in significant results, F(1, 146) = 20.51, P < 0.001, n2 = 0.123. After the intervention, the intervention group reported higher well-being at baseline (M = 22.63, SD = 4.10) compared with the control group (M = 19.49, SD= 4.98). These two interactions are depicted in Figures 1 and 2.

The interaction between time and group for the effect of the Kioku board game on loneliness.
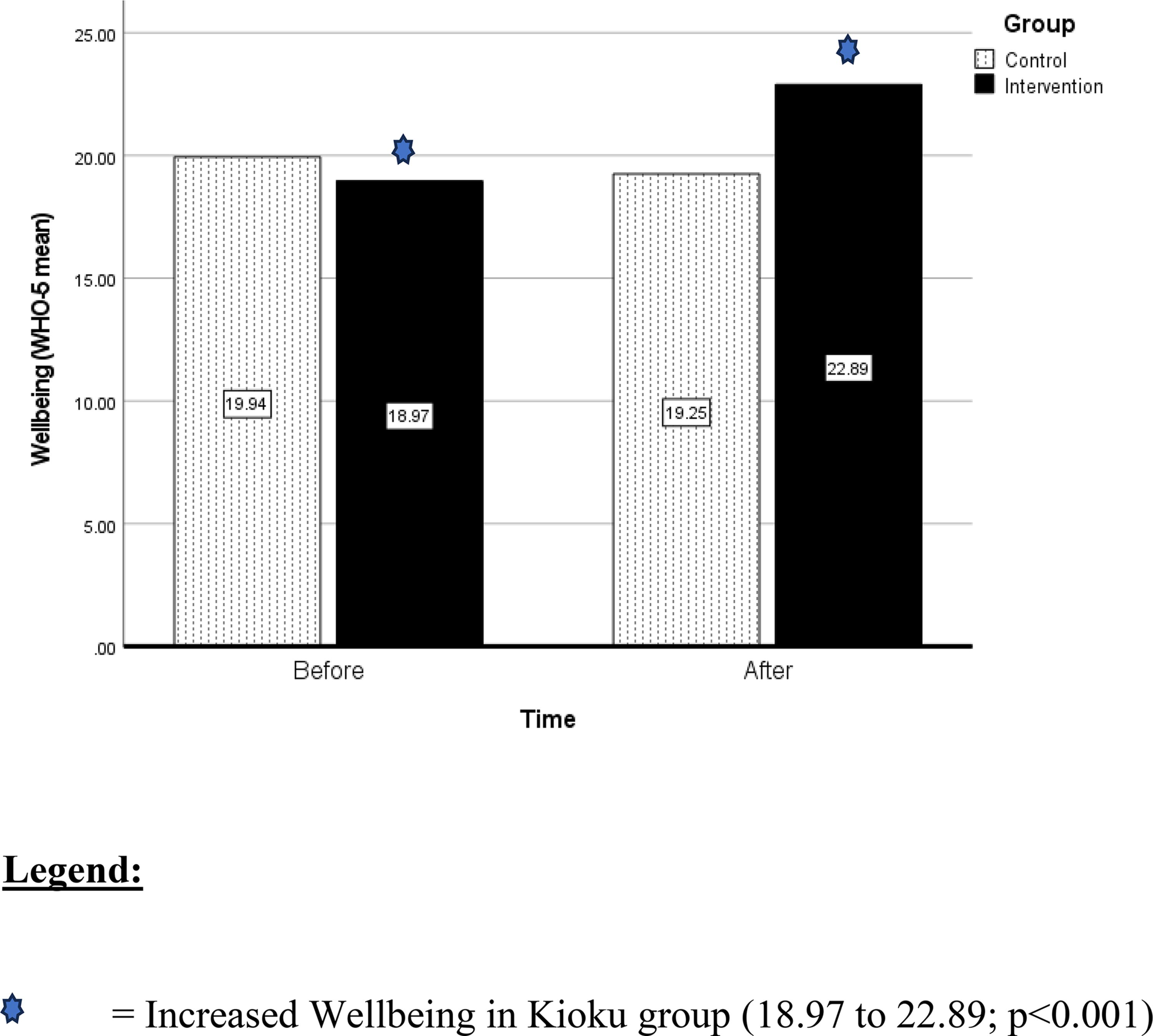
The interaction between time and group for the effect of the Kioku board game on well-being.
Discussion
This study provides the first evidence for the positive effect on loneliness of a block-word board game intervention among community-dwelling older adults. Our findings show that in the intervention group, there was a decrease in the participants’ level of loneliness and increase in their sense of well-being.
Social isolation, social disconnectedness, perceived isolation, and loneliness are known to be linked to common physical and mental health problems in older people. It is recognized that strategies to maintain social connectedness could be important in ensuring the biopsychosocial health of older people. Several small-scale trials of a variety of interventions delivered to socially isolated older people have produced encouraging preliminary results. A recent living systematic review demonstrates strong meta-analytical signal of effect in reducing loneliness in the short term. In support of these findings, it was also demonstrated that interventions designed to specifically target loneliness are likely to be more effective than unmodified psychotherapeutic approaches in reducing levels of loneliness. 25
This study demonstrates that participation in a targeted activity of creating stories in a group setting reduces loneliness and increases well-being.
This study explored the experience of participation in a shared group game. Groups of people sharing an activity, performed collectively, can be considered a unique form of the leisure culture that anyone can easily enjoy. The findings indicate that the participants’ loneliness and well-being improved as they engaged in playing Kioku. The participants’ reduced feelings of loneliness could have resulted from an increase in their sense of belonging through exchanges with other members of their groups. The participants engaged in Kioku and shared their personal associations, while creating stories together. They assisted other participants in this creative process, by relating to their input and by adding their own contribution to the story of the whole group. It is possible that each participant felt he or she was contributing to the group’s product. We tentatively suggest that Kioku reduces the distance between people by creating environments where they can connect and enhance their ability to exchange and socialize with each other.
Board games provide an opportunity for players to interact socially and create a form of enjoyment. Moreover, previous studies have demonstrated that participants gain a sense of accomplishment and excitement from board games. 26 There is evidence that around 40% of older adults in a nursery home play board games such as Parcheesi, dominoes, cards, or playing cards, among many others. 27 Following this line of thought, researchers recommend designing interventions for older adults by attending to the activities suggested by older adults themselves, which emphasize action and social engagement.
An often-underemphasized component of work with older adults is the use of storytelling and the elicitation of their memories. Memories are not just a storehouse for facts, but a creative blend of fact and fiction that helps people tell meaningful stories about their lives. Throughout history, the older members of our collective cultures have been civilization’s best storytellers. Storytelling is probably the best method for communicating important—sometimes complex—concepts in a simple and memorable way. Storytelling and listening to stories in groups are probably the most natural form of communication. The most basic and powerful way to connect to another person is to listen. 28 It has been well established that neural processes synchronize between subjects when they are being exposed to an identical narrative stimulus. 29 Moreover, it was found that telling a story to an attentive audience positively impacts the self-esteem of the storyteller. Storytelling plays a vital role in all cultures, as it keeps history and legacy alive. 30 In addition, people in independent living communities make connections through sharing stories. By giving people a way to create and share stories, they can gain a greater understanding of their fellow participants, helping them to better appreciate and become more comfortable in their shared experience. 31 Storytelling not only improves psychological well-being but has also been shown to reduce feelings of loneliness. 32
Targeted interventions aimed at combating loneliness and social isolation in older age are more and more often technology based. Targeted interventions that aim at greater social inclusion of seniors are increasingly designed and delivered as so-called “e-interventions” using internet technologies, computers, smartphones, custom-made devices, and software for seniors. A recent scoping review summarized the communication technologies used in the last decade, concluding that, while research reviews show that communication technologies can reduce loneliness and social isolation in older people, causal evidence is limited, and insights on innovative technologies such as augmented reality systems are scarce. 33 These conclusions are supported by an innovative board game with augmented reality developed and researched in Taiwan, demonstrating the positive potential of integrating augmented reality technology into cognitive-based games for older adults. 34 Finally, the research in this field need to take into account the challenges inherent in conducting remote digital trials of a social gaming intervention for older adults. 35
This study has several limitations that need to be acknowledged. Although the participants’ assignment to the study groups was randomized, sociodemographic differences between the groups had to be controlled for. Moreover, the reported level of loneliness before the intervention was higher in the intervention group than in the control group. Yet, the randomized controlled group assignment of participants negates the possibility of participants’ self-selection. The intervention involved training and engaging facilitators who not only facilitated game sessions but also maintained weekly contact with the participants between sessions. This facilitation effort may have contributed to the reported outcomes. This conversely may be seen as a strength of the intervention’s design. Games on their own are mere objects. It is the intersubjective interaction between participants and the experience created through them that can help contribute to the power of an intervention. This study was conducted during the later phases of the COVID-19 pandemic, following several lockdowns. These lockdowns may explain, in part, the increase in loneliness and the decrease in well-being in the control group. Searching databases for loneliness in combination with games as a construct may not be as productive as other proxy variables. Finally, the lack of a third control group that would have undergone a different group intervention would have potentially ruled out the alternative explanation of “Hawthorne effect.” 36
Exploring potential mechanisms through which social interactions by playing games can decrease loneliness is not often undertaken. The potential mechanisms triggered by playing games in a group setting are identified in the literature: Supporting health behaviors; providing emotional support; improving mood; cognitive stimulation and novelty; and providing opportunities for socializing. 37 These mechanisms are further supported by recent research into group membership and identification, with one group that has been found to be positively related to individuals’ health and well-being. 38
It is important to note this study’s uniqueness. Despite the importance of group board games, there is almost no study that has examined the effectiveness of these games on the level of loneliness and well-being of older adults. For example, a recent systematic review did not analyze the effects of board games, further emphasizing the novelty of our project 36 The Kioku game, whose effectiveness in alleviating loneliness and increasing well-being was demonstrated in this study, makes use of social processes of joint creation of group stories, which are unique to the group, and enable a shared experience for the group members. The encouraging findings of this study, together with the ease with which the game can be taught and played, and the possibility of using it in different languages and spreading it between different cultures—all of these reinforce the need for further research.
Footnotes
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by R.C. and A.S. Y.B. wrote most parts of the introduction, methods, and the discussion sections. E.B. preformed the analysis and wrote the results section and some parts of the methods and the discussion sections. All authors commented on previous versions of the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.