
Abstract
The aim was to analyze the effects of virtual reality-based rehabilitation (VRBR) in patients with fibromyalgia syndrome (FMS). This systematic review and meta-analysis was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A search was conducted in CINAHL, Medline (via PubMed), Scopus, and Web of Science up to January 2023. Eligibility criteria were defined with Participants, Interventions, Comparisons, Outcomes, and Study design. To assess the methodological quality, the modified Downs and Black scale was used. The risk of bias was assessed through The Cochrane Collaboration’s tool. Meta-analysis was performed using RevMan software. Seventeen studies were included in the systematic review and 11 in the meta-analysis. We obtained significant differences in favor of VRBR for FMS impact (standardized mean difference or SMD: −0.49; 95% confidence interval or CI: −0.72 to −0.26), pain intensity (SMD: −0.50; 95% CI: −0.87 to −0.12), fatigue (SMD: −0.55, 95% CI: −0.89 to −0.22), depression (SMD: −0.39; 95% CI: −0.55 to −0.23), anxiety (SMD: −0.36; 95% CI: −0.57 to −0.14), health-related quality of life (SMD: 0.56; 95% CI: 0.29 to 0.83), health perception (mean difference or MD:10.56; 95% CI: 6.23 to 14.88), functional exercise capacity (SMD: 0.60; 95% CI: 0.33 to 0.87), and physical function (MD: 10.90; 95% CI: 7.04 to 14.77). No significant differences were found for kinesiophobia. VRBR significantly improves FMS symptoms, quality of life, and physical condition. VRBR applied alone or combined with other interventions shows good results. VRBR was superior to treatment as usual. Better results were obtained when specialized VRBR was used. More research is needed to determine how to implement this treatment and to study VRBR effects on follow-up.
Introduction
Fibromyalgia syndrome (FMS) is a chronic pain syndrome characterized by diffuse tenderness. 1 FMS is associated with musculoskeletal pain, tender points, fatigue, anxiety, depression, poor physical condition, paresthesia, sleep disorders, or cognitive and somatic symptoms.1,2 These symptoms can lead to a decrease in the quality of life. 3 FMS does not have a curative treatment. 4 Pharmacological treatment is focused on pain reduction. Rehabilitation presented as therapeutic exercise, which has the highest level of evidence, aims to reduce the symptoms and consequences of disease. 5 It is considered a cheap and effective tool to improve pain relief, physical function, and well-being.6–8 However, the main limitation of therapeutic exercise is lack of adherence. 9
Virtual reality (VR) is a novel tool that is increasingly used in rehabilitation. 10 VR includes a large number of technological devices and systems with different characteristics. 11 There are two types of VR considering the device used, “specialized” VR and gaming VR. 12 VR-based rehabilitation (VRBR) is considered a very useful tool in FMS 13 for promoting health.14,15 VRBR shows benefits in modulating pain 16 and in depression symptoms 17 in FMS. In addition, VRBR provides visual and auditory feedback, can be goal-oriented, and is attractive to the patient. It has the potential to improve adherence to an exercise program and motivation. 18
Kantha et al. 19 explored the effectiveness of VRBR in chronic musculoskeletal disorders, including FMS. VRBR appeared to reduce pain, but current evidence on the type of VR remains unclear. Cortes-Perez et al. 20 concluded that VRBR is effective in reducing FMS impact, pain, fatigue, anxiety, and depression. Wu et al. 21 found similar beneficial effects. However, in both reviews the results should not be considered conclusive and should not be generalized due to the number of included studies, small sample sizes and heterogeneity.
Since Wu et al. 21 performed the search, new evidence has been published. Moreover, a complete subgroup analysis based on VRBR interventions is needed. There is no previous evidence of what type of VR is more effective specifically in patients with FMS. In addition to know if VRBR should be applied alone or combined with other interventions, it would be of interest to explore the effects of the different types of VR. The objective of this systematic review and meta-analysis was to analyze the effects of VRBR in patients with FMS.
Methods
Design
We performed a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 22 It was registered in the International Prospective Registry of Systematic Reviews (PROSPERO): CRD42020218811.
Search strategy
A search was conducted in four databases [CINAHL, Medline (via PubMed), Scopus, and Web of Science] from their inception until January 2023 (Supplementary Data S1). We reviewed the reference list of related articles. Another search was conducted for ongoing trials (Supplementary Data S2).
Study selection
We established the following PICOS criteria. 23 Participants: confirmed diagnosis of FMS according to the American College of Rheumatology criteria.2,24,25 Interventions: VRBR. Comparisons: no VRBR. Outcomes: FMS impact and other measures associated with FMS. Study design: randomized clinical trials (RCTs).
Two independent reviewers (B.B.-G. and L.P.-G.) conducted a search using Mendeley Reference Manager (Mendeley Desktop, London, UK) to recognize articles, check duplicates, and standardize references. A first screening was performed based on title and abstract. In the second screening, an analysis of the full text was made. We emailed the corresponding author if full text was not available. The studies that met the inclusion criteria were selected. A third researcher (I.T.-S.) resolved the discrepancies.
Data extraction
The following information was extracted from each study. Characteristics of studies (Table 1): reference, country, sample size, age, outcome measures, measuring instrument, main results, and timepoint assessment. Characteristics of interventions (Table 2): reference, interventions, session duration, frequency, program duration, supervision, and adverse effects.
Characteristics of Included Studies
SD, standard deviation; EG, experimental group; CG, control group; FMS, fibromyalgia syndrome; FIQ, Fibromyalgia Impact Questionnaire; BPI, Brief Pain Inventory; CPCI, Chronic Pain Coping Inventory; NS, no significant differences; BDI-II, Beck Depression Inventory II; HRQoL, health-related quality of life; QLI-Sp, Quality of Life Index; VR, virtual reality; PC, physical condition; TUG, Timed Up and Go Test; CTSIB, Clinical Test of Sensory Integration of Balance; VAS, Visual Analog Scale; VAS EQ-5D, Visual Analog Scale European Quality of Life-5 Dimensions; EQ-5D-5L, European Quality of Life-5 Dimensions-5 Levels; PANAS, The Positive and Negative Affect Scale; LOT-R, The Life Orientation Test–Revised; SPT, Subjective Probability Task; GSES-12, General Self-Efficacy Scale; FIQ-R, revised Fibromyalgia Impact Questionnaire; PCS, Pain Catastrophizing Scale; GDS, Geriatric Depression Scale; EEG, electroencephalography; 6-MWT, 6 minute walking test; MET, metabolic equivalents; IPAQ, The International Physical Activity Questionnaire; PsO2, peripheral oxygen saturation; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; MRI, magnetic resonance imaging; pvO2, peak oxygen consumption; MMSE, Mini-Mental State Examination; HRV, heart rate variability; SDNN, standard deviation of all normal-to-normal RR intervals; RMSSD, the root mean square of successive differences between RR intervals; HFD, Higuchi Fractal Dimension; EMG, electromyography; SSS, Symptom Severity Scale; FSS, Fatigue Severity Scale; HADS, Hospital Anxiety and Depression Scale; TSK, The Tampa Scale for Kinesiophobia; SF-PF, The physical functioning component of the 36-item Short-Form Survey; MSOT, Modified Sensory Organization Test; SF-36, 36-item Short-Form Survey.
Characteristics of Interventions
CBT, cognitive-behavioral therapies; VRPC, personal computer; FM, fibromyalgia; TAU, treatment as usual; BPS, best possible self; DA, daily activity; RM, repetitive maximum; IVR, immersive virtual reality; RAGU, Augmented Reality Applications in Rehabilitation; PNE, pain neuroscience education; MPP, multicomponent physiotherapy program.
Methodological quality
To assess methodological quality, the modified Downs and Black scale was used. 42 It has 27 questions divided into five sections. Scores range from 0 to 28. Higher scores suppose better methodological quality. Cut-off points were as follows: excellent (26–28), good (20–25), fair (15–19), and poor (<14).
Risk of bias
The risk of bias was assessed through the Cochrane risk-of-bias tool. 43 Bias was evaluated using seven items. Each item is classified as “low risk of bias,” “unclear risk of bias,” or “high risk of bias.”
Two independent investigators (B.B.-G. and L.P.-G.) performed the data extraction and the assessment of methodological quality and risk of bias. A third researcher (I.T-.S.) resolved the discrepancies.
Statistical analysis
Meta-analysis was performed using Review Manager software version 5.4 (The Nordic Cochrane Center, Copenhagen, Denmark). Forest plots were used to display the results. To estimate the overall effect, the pre–post differences and pooled standard deviations (SDs) were calculated according to the following formulas:
Heterogeneity between studies was assessed using the I2 test: low (I2 <25%), moderate (I2 = 25%−75%), and high (I2 >75%). We performed a subgroup analysis to explore heterogeneity. Subgroups were chosen according to comparisons, comparators, and type of VR. If 10 or more studies were available, we planned to use funnel plots with pseudo 95% confidence limits to inspect publication bias. 44
Results
Search results
We identified 571 articles. After removing the duplicates and determining eligibility, 17 articles were included (Fig. 1). Supplementary Data S3 describes the excluded studies in the last screening. We identified 11 ongoing trials. Finally, five studies met the inclusion criteria (Supplementary Data S4).
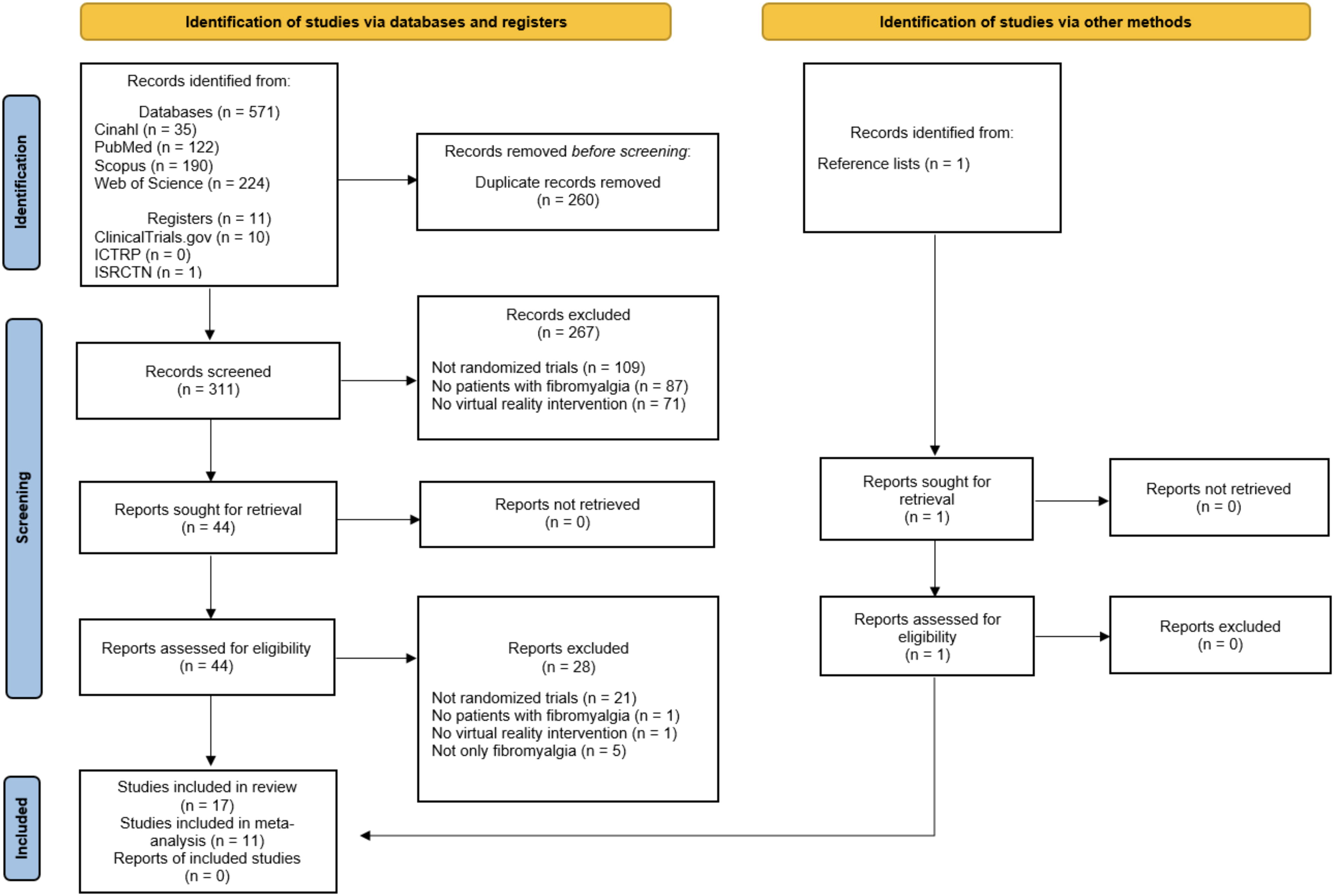
Flow diagram: database and clinical trials register search.
Characteristics of studies
See Table 1. All studies were published between 2015 and 2022.15,26–41 Studies were performed in Spain,15,26–33,35,36,39,41 Brazil,34,37 and Turkey.38,40 The number of patients was 1291. Age ranged between 38 and 55 years.
FMS impact (primary outcome)
The FMS impact was assessed with the Fibromyalgia Impact Questionnaire (FIQ)15,26,34,38,40 and the revised FIQ.28,33,39,41
Outcomes related to FMS symptoms
Symptoms related to FMS such as pain intensity and fatigue were assessed using the Brief Pain Inventory 26 or Visual Analogue Scale (VAS)32,38,40,41 and Fatigue Severity Scale,38,40 respectively. Regarding psychological symptoms, kinesiophobia was evaluated with the Tampa Scale for Kinesiophobia39–41 ; depression with Beck Depression Inventory II,26,28 Geriatric Depression Scale, 29 and Hospital Anxiety and Depression Scale (HADS)38,39,41; and anxiety with HADS.38,39,41
Outcomes related to quality of life
Health-related quality of life (HRQoL) was evaluated using the Quality of Life Index,26,28 the utility score of the European Quality of Life-5 Dimensions-5 Levels (EQ-5D-5L),15,32,38 and 36-Item Short-Form Survey (SF-36). 40 Health perception was evaluated using the VAS of the EQ-5D.15,32,38
Outcomes related to physical condition
Several outcomes were assessed among included studies. Functional exercise capacity was assessed through the 6-minute walk test,33,38,40 step test, 34 and Timed Up and Go Test.27,30 Physical activity was assessed using the International Physical Activity Questionnaire,33,40 and physical function with the physical functioning component of the SF-36.39,41
All studies evaluated outcomes pre- and postintervention. Two studies included follow-up, one of them 28 at 1 and 3 months postintervention and the other one 33 after 24 weeks. Two studies34,37 included an assessment after 10 sessions and the other study 38 after 4 weeks.
Characteristics of interventions
See Table 2. Most of the studies used specialized VR such as EMMA display, 26 VirtualEx-FM,15,27,29–33,35,36 A Book of Life, 28 FIBROWALK,39,41 and Augmented Reality Applications in Rehabilitation (RAGU) system. 40 Three studies used gaming VR: The Nintendo Wii system34,37 and Microsoft Xbox Kinect. 38 VRBR was combined with cognitive-behavioral therapies 26 and with treatment as usual (TAU).39,41 In the remaining studies, VRBR was applied alone.
VRBR interventions were compared with TAU in three studies.26,39,41 In nine studies,15,26,29–33,35,36 control group patients continued with their daily lives. Another study 28 guided exercises by a PowerPoint presentation. Four studies34,37,38,40 conducted an exercise program.
In most studies, sessions lasted 60 minutes. Time using VRBR ranged from 5 to 60 minutes. Frequency of treatment was similar among studies; 1–3 sessions were performed per week. The duration of program ranged from 3 to 24 weeks. Different professionals supervised the interventions. Seven studies27,31–33,35,36,38 declared no adverse effects.
Methodological quality
We used the modified Downs and Black scale to assess methodological quality (Supplementary Data S5). One study 38 was classified as “excellent” (26–28), 14 studies15,27–37,39,41 as “good” (20–25), and two studies26,40 as “fair” (15–19).
Risk of bias
“Random sequence generation,”29,34 “blinding of outcome assessment,”26,27 and “selective reporting”26,40 obtained “unclear risk of bias” in two studies of each one. The remaining studies obtained “low risk of bias.” Two studies27,34 had “unclear risk of bias” in “blinding of participants and personnel.” The remaining studies obtained “high risk of bias.” In “allocation concealment,” two studies30,31 obtained “high risk of bias,” seven studies27,28,35,36,38,39,41 “low risk of bias,” and eight studies15,26,29,32–34,37,40 “unclear risk of bias.” Regarding “incomplete outcome data,” three studies27,29,36 presented “unclear risk of bias” and another three studies33,39,40 “high risk of bias.” The remaining studies obtained “low risk of bias.” In “other bias,” all studies showed “unclear risk of bias” (Fig. 2).
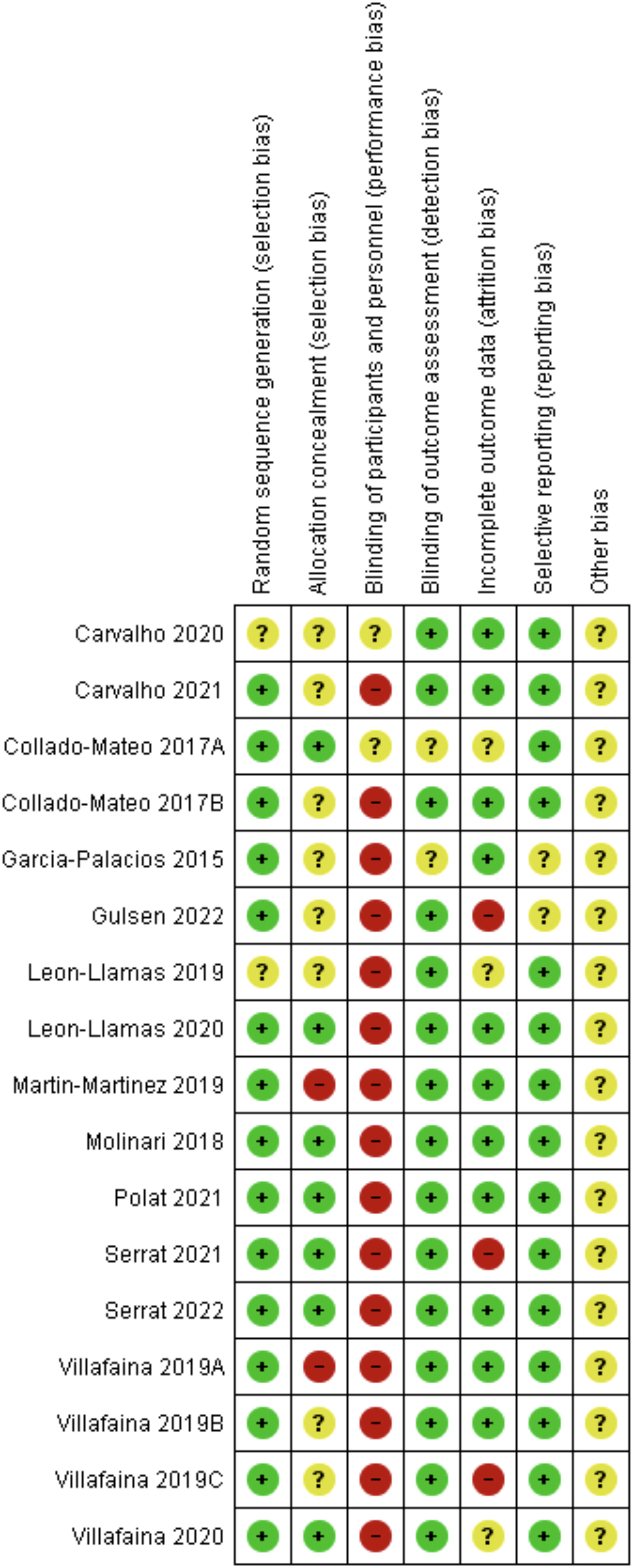
Risk-of-bias summary.
Quantitative synthesis
For meta-analysis, we considered all outcomes repeated at least in two articles. We analyzed the effects of VRBR versus no VRBR for 10 outcomes. Eleven articles were included. Gulsen et al. 40 were excluded because they did not express data in mean ± SD.
Effects of VRBR on FMS impact (primary outcome)
Eight studies evaluated FMS impact.15,26,28,33,34,38,39,41 VRBR intervention indicated a moderate effect on FMS impact (SMD = −0.49, P < 0.0001, 95% CI = −0.72 to −0.26, Z = 4.21, I2 = 47%), suggesting that VRBR is effective in improving FMS impact. The improvement reached a significant level (Fig. 3A).

Forest plot summarizing standardized mean difference (SMD) and 95% confidence interval (CI) for the effects of VRBR versus no VRBR in fibromyalgia for fibromyalgia syndrome (FMS) impact
We performed a subgroup analysis to explore heterogeneity. First subgroup analysis was based on comparisons (VRBR applied alone or combined with other interventions). We conducted a subgroup analysis based on comparators (usual daily life, TAU, or exercises). Last, a subgroup analysis was performed according to the type of VR (specialized VR or gaming VR).
Subgroup analysis showed a moderate effect size, favoring VRBR applied alone versus no VRBR (SMD = −0.33, P = 0.01, 95% CI = −0.58 to −0.08, Z = 2.57, I2 = 0%). We also observed a moderate effect size favoring VRBR combined with other interventions versus VRBR (SMD = −0.65, P = 0.0005, 95% CI = −1.02 to −0.29, Z = 3.48, I2 = 68%). The results suggested that VRBR applied alone or combined with other interventions is effective in reducing FMS impact. In both subgroups, results reached a significant level (Fig. 3B).
Regarding subgroup analysis based on comparators (Fig. 3C), the results showed a moderate effect size favoring VRBR versus usual daily life (SMD = −0.28, P = 0.09, 95% CI = −0.61 to 0.04, Z = 1.17, I2 = 20%) or versus exercises (SMD = −0.45, P = 0.09, 95% CI = −0.96 to 0.06, Z = 1.72, I2 = 0%). Although VRBR improved FMS impact, a significant level was not reached in these subgroups. The results showed a moderate effect size favoring VRBR versus TAU (SMD = −0.65, P = 0.0005, 95% CI = −1.02 to −0.29, Z = 3.48, I2 = 68%), suggesting that VRBR is effective in improving FMS impact more than TAU. The improvement reached a significant level.
In subgroup analysis based on the type of VR (Fig. 3D), we observed a moderate effect size favoring specialized VR versus no VRBR (SMD = −0.49, P = 0.0005, 95% CI = −0.77 to −0.21, Z = 3.47, I2 = 61%), suggesting that specialized VR is effective in improving FMS impact more than no VRBR. In addition, gaming VR indicated a moderate effect size (SMD = −0.45, P = 0.09, 95% CI = −0.96 to 0.06, Z = 1.72, I2 = 0%), suggesting that it may be effective in reducing FMS impact more than no VRBR. However, a significant level was not reached.
Effects of VRBR on symptoms related to FMS
Six studies evaluated pain intensity.15,26,32,34,38,41 We observed a moderate effect size favoring VRBR versus no VRBR (SMD = −0.50, P = 0.009, 95% CI = −0.87 to −0.12, Z = 2.60, I2 = 70%), suggesting that VRBR is effective in reducing pain intensity. The results reached a significant level (Fig. 4A).
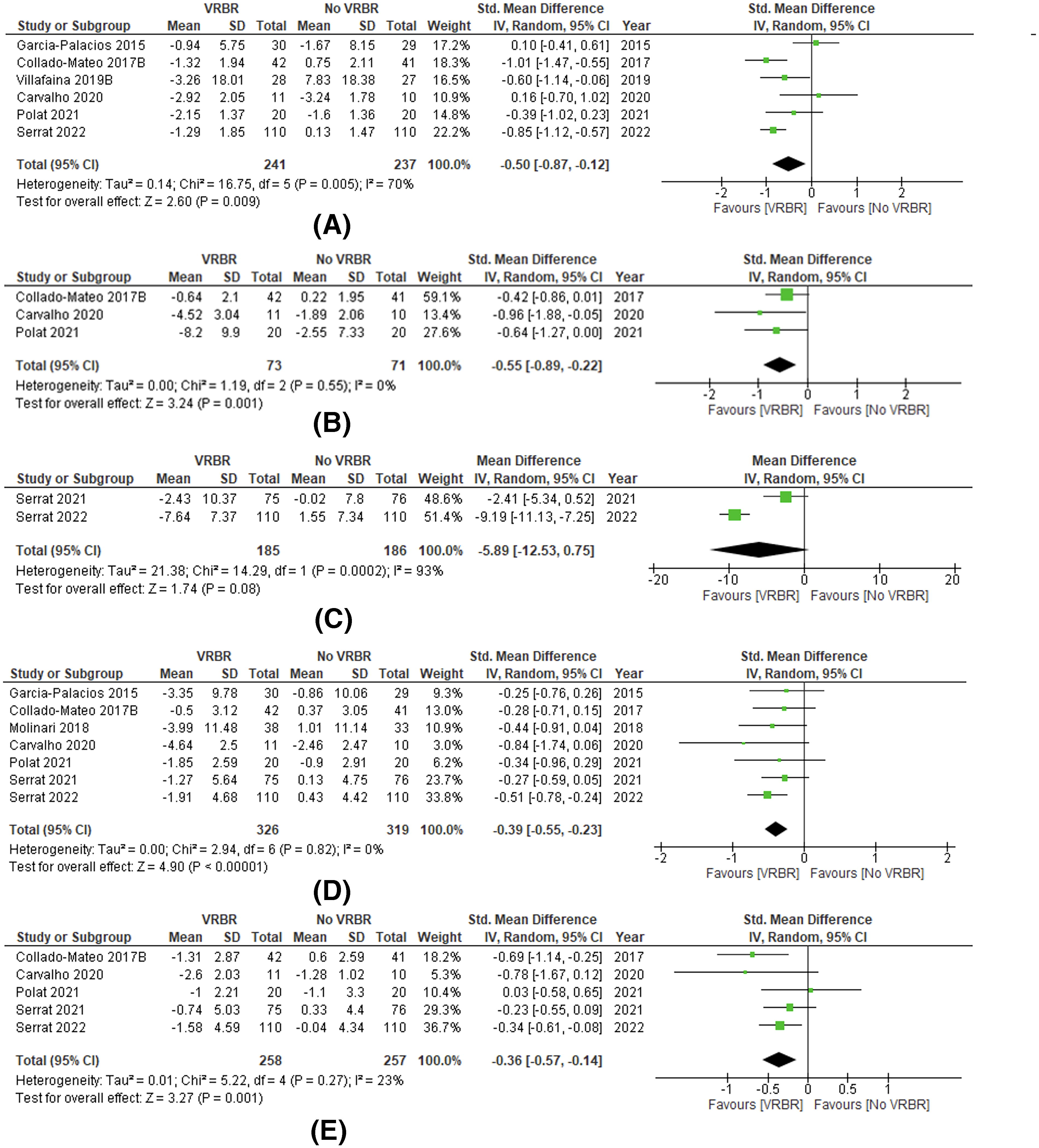
Forest plot summarizing MD or SMD and 95% CI for the effects of VRBR versus no VRBR in fibromyalgia for pain intensity
Three studies evaluated fatigue.15,34,38 We observed a moderate effect size favoring VRBR versus no VRBR (SMD = −0.55, P = 0.001, 95% CI = −0.89 to −0.22, Z = 3.24, I2 = 0%), suggesting that VRBR is effective in reducing fatigue. The results reached a significant level (Fig. 4B).
Two studies evaluated kinesiophobia.39,41 No significant differences were found between VRBR and no VRBR (MD = −5.89, P = 0.08, 95% CI = −12.53 to 0.75, Z = 1.74, I2 = 93%). However, kinesiophobia levels were lower in the VRBR group (Fig. 4C).
Seven studies evaluated depression.15,26,28,34,38,39,41 We observed a moderate effect size favoring VRBR versus no VRBR (SMD = −0.39, P < 0.00001, 95% CI = −0.55 to −0.23, Z = 4.90, I2 = 0%), suggesting that VRBR is effective in improving depression. The results reached a significant level (Fig. 4D).
Five studies evaluated anxiety.15,34,38,39,41 We observed a moderate effect size favoring VRBR versus no VRBR (SMD = −0.36, P = 0.001, 95% CI = −0.57 to −0.14, Z = 3.27, I2 = 23%), suggesting that VRBR is effective in improving anxiety. The results reached a significant level (Fig. 4E).
Effects of VRBR on quality of life
Five studies evaluated HRQoL.15,26,28,32,38 We observed a moderate effect size favoring VRBR versus no VRBR (SMD = 0.56, P < 0.0001, 95% CI = 0.29 to 0.83, Z = 4.01, I2 = 28%), suggesting that VRBR is effective in improving HRQoL. The results reached a significant level (Fig. 5A).

Forest plot summarizing MD or SMD and 95% CI for the effects of VRBR versus no VRBR in fibromyalgia for health-related quality of life (HRQoL)
Three studies evaluated health perception.15,32,38 Significant differences were found in favor of VRBR versus no VRBR (MD = 10.56, P < 0.00001, 95% CI = 6.23 to 14.88, Z = 4.79, I2 = 0%), suggesting that VRBR is effective in improving health perception (Fig. 5B).
Effects of VRBR on physical condition
Five studies evaluated functional exercise capacity.27,30,33,34,38 We observed a moderate effect size favoring VRBR versus no VRBR (SMD = 0.60, P < 0.0001, 95% CI = 0.33 to 0.87, Z = 4.40, I2 = 0%), suggesting that VRBR is effective in improving functional exercise capacity. The results reached a significant level (Fig. 6A).

Forest plot summarizing MD or SMD and 95% CI for the effects of VRBR versus no VRBR in fibromyalgia for functional capacity
Two studies evaluated physical function.39,41 Significant differences were found in favor of VRBR versus no VRBR (MD = 10.90, P < 0.00001, 95% CI = 7.04 to 14.77, Z = 5.53, I2 = 0%), suggesting that VRBR is effective in improving physical function (Fig. 6B).
Publication bias
Publication bias was not assessed because it is not recommended for fewer than 10 articles. 44
Qualitative synthesis
Cerebral and cardiac parameters could not be meta-analyzed. Villafaina et al. 31 presented significant differences at the frontal, parietal, temporal, and occipital levels, with all changes in favor of VRBR. Leon-Llamas et al. 35 did not show significant changes on volume of gray matter between groups after 24 weeks. Finally, Villafaina et al. 36 showed improvements in autonomic control in patients with FMS. However, no significant effects of VRBR were found on heart rate variability (HRV).
Discussion
This systematic review represents an update in the knowledge about the effectiveness of VRBR in FMS patients. Significant differences were found in favor of VRBR for FMS impact, FMS symptoms (pain intensity, fatigue, depression, anxiety), quality of life (HRQoL, health perception), and physical condition (functional exercise capacity, physical function). In addition, we performed a meta-analysis with a subgroup analysis that has not been conducted previously.
In most studies, interventions were conducted to reduce the FMS impact and related symptoms. Other studies were performed to improved quality of life and physical condition. In addition, some studies specifically focus on brain and cardiac parameters.
Impact on FMS and related symptoms
Meta-analysis showed significant differences in favor of VRBR for FMS impact. Two recent systematic reviews20,21 also suggested that VRBR is effective in reducing FMS impact. Regarding subgroup analysis, VRBR was statistically more effective than no VRBR when it was applied alone or combined with other interventions. Similar effects were observed in Cortes-Perez et al. 20 The combined use of VRBR with conventional therapy-based therapeutic exercise (CTBTE) is better than perform only CTBTE. They observed that VRBR is better than no intervention. Significant differences in favor of VRBR were only found when we compared with TAU. It should be noted that included articles in the TAU subgroup has a greater sample size. Finally, according to the type of VR, we observed significant differences in favor of specialized VRBR. However, gaming VR was not significantly superior to no VRBR. In most included studies, VR systems have been developed in research settings. These systems are not commercially available, or they are very expensive. Despite the found results, gaming VR has the advantages of being user-friendly and accessible, providing easily perceived feedback and most importantly, it is affordable.47,48 Nevertheless, gaming VR is not specifically designed for therapeutic purpose, which may explain the results. In addition, only two articles were included.
It was not possible to perform meta-analysis based on dosage. However, we observed among included studies some consensus regarding the session duration. On the one hand, most of the included studies applied VR alone in 60-minute sessions. On the other hand, in the remaining studies, VR was combined with other interventions and the time using VR differed between them. We observed that time using VR was considerably less (5–20 minutes). It should be considered that both types of interventions obtained good results according to the analysis mentioned above. Regarding frequency and program duration, most of the included studies conducted two sessions per week and the programs lasted 24 weeks. Nevertheless, due to the differences in these parameters, it is difficult to draw solid conclusions, although considering other pain disorders,49,50 FMS programs are the longest, which may explain the good results obtained.
Regarding specific symptoms, our findings showed significant differences in favor of VRBR for pain intensity. A previous systematic review on chronic musculoskeletal pain 19 recommends the use of VRBR for reducing pain intensity more than no rehabilitation or conventional rehabilitation, which is in line with our findings. Another very common symptom is fatigue. We observed significant differences in favor of VRBR. Results in previous reviews20,21 showed a significant reduction in pain and fatigue in favor of VRBR.
FMS patients have higher levels of kinesiophobia. 51 Meta-analysis did not show significant differences between VRBR and no VRBR, which is in line with Wu et al. 21 Regarding depression and anxiety, we observed significant differences in favor of VRBR versus no VRBR. León-Llamas et al. 29 did not present improvements in depression symptoms after conducting the intervention, but it may be associated with not considering the social component. There is evidence that partially supports our results. A recent systematic review 52 reported that gaming modalities, such as VRBR, are superior to other treatments to improve pain-related fear, and superior to no treatment to improve anxiety in chronic musculoskeletal pain. Cortes-Perez et al. 20 also found an improvement in depression and anxiety levels after the use of VRBR.
Quality of life
FMS symptoms have a negative impact on HRQoL. 3 It was expected that an improvement of these symptoms increases HRQoL. On the one hand, VRBR increases physical activity. On the other hand, VRBR has a positive impact on patients’ emotional well-being and increases motivation. We found significant differences in favor of VRBR versus no VRBR. A previous systematic review in older adults 53 indicates that VRBR has a positive effect on improving HRQoL, which is in line with our findings.
Physical condition
One of the main limitations of therapeutic exercise is lack of adherence. 9 Inactivity can aggravate symptoms in FMS patients. Improving physical condition is essential. We observed significant differences in favor of VRBR versus no VRBR for functional exercise capacity and for physical function. VRBR promotes motor learning. 54 Patients gain confidence in their physical abilities, engaging in physical activity, 19 and as a consequence improving adherence to therapeutic exercise treatment.55,56
Brain and heart
Some studies31,35,36 observed the impact of VRBR on the brain and HRV. Regarding the volume of gray matter, no significant changes were observed. 35 Previous studies indicate the importance of considering the variability of intensities, volumes or types of training. Volumetric changes have been reported after the interventions, controlling for these variables. 57 Villafaina et al. 36 showed improvements in autonomic control in patients with FMS, but not on HRV. Martínez-Lavín et al. 58 proposed that sympathetic hyperactivity could be related to insomnia, anxiety, and chronic pain suffered by FMS patients.
Discussion with other reviews
In general, results in Cortes-Perez et al. 20 and Wu et al. 21 are similar to those found in our review. Both systematic reviews supported our findings. It should be noted that meta-analyses were performed in different ways, and this could explain some differences.
Adverse effects
It is known that the use of VR may cause several adverse effects, including nausea, dizziness, disorientation, postural instability, headache, and fatigue. These unpleasant physical symptoms are often referred to as cyber sickness.59,60 Of the 17 studies included in our review, seven provided information about adverse effects. None of them reported finding adverse effects related to intervention. Most of the included studies in the review implemented a type of low-immersion VR. A recent paper 59 confirmed that the level of cyber sickness is related to the type of VR immersion, which may explain the results. However, many of the included studies did not provide any type of information about the adverse effects and some of them did not clarify the reasons for the dropouts. It is important that adverse effects leading to dropouts or clinical worsening are identified and reported.
Limitations
In most of the studies, the sample sizes were relatively small. There was no blinding of the participants due to the nature of the studies. None of the studies included long-term follow-up and only one study included midterm follow-up. There was heterogeneity among interventions and making comparable subgroups was difficult. Finally, the results must be interpreted cautiously due to heterogeneity observed in some analyses.
Considerations for clinical practice and future research
VRBR should be considered in clinical practice for improving FMS impact, symptoms, quality of life, and physical condition. Future research should focus on the effects on follow-up due to lack of data. VRBR applied alone and combined with other interventions obtained favorable results, but more research is needed. Specialized VR showed better results than gaming VR. However, gaming VR devices are commercially available and easier to implement in clinical practice, so investigating this type of VR is necessary. Although VR may involve a significant investment, its potential benefits may support its use. VRBR is believed to improve motivation, but studies do not assess this outcome. Future studies should be RCTs of large sample sizes, reporting concrete intervention protocols and assessing motivation. In addition, reporting adverse effects is particularly essential because they can significantly influence the therapeutic effect of the intervention.
Conclusions
VRBR is a promising therapy for FMS rehabilitation. VRBR significantly improves FMS impact, symptoms, quality of life, and physical condition. However, no significant differences were obtained for kinesiophobia. Regarding subgroup analysis, better results were showed for VRBR applied alone or combined with other interventions, compared with TAU and using specialized VRBR. Despite the favorable results, the interpretation must be cautious due to heterogeneity between VRBR interventions.
Footnotes
Acknowledgments
This article forms part of the doctoral thesis developed by Beatriz Brea Gómez in the context of the Clinical Medicine and Public Health Program of the University of Granada (Spain).
Authors’ Contributions
All authors substantially contributed to preparing this article. Conceptualization: B.B.-G., M.C.V., and I.T.-S. Methodology: B.B.-G., L.P.-G., I.F.-C., M.C.V., and I.T.-S. Formal analysis and investigation: B.B.-G. and I.T.-S. Writing—original draft preparation: B.B.-G., L.P.-G., I.F.-C., M.C.V., and I.T.-S. Writing—review and editing: B.B.-G., L.P.-G., I.F.-C., M.C.V., and I.T.-S. Supervision: M.C.V. and I.T.-S.
Author Disclosure Statement
The authors have no potential conflicts of interest to disclose.
Funding Information
This research received no external funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.